Hereditary Hemochromatosis and Polydactyly: A Case Report
Shloka Reddy, Steve Thomas

TL;DR
A young male with a family history of polydactyly was diagnosed with hereditary hemochromatosis due to the H63D homozygous mutation, leading to elevated iron levels and joint pain.
Contribution
This case report highlights the rare occurrence of H63D homozygous mutation in a patient with a polydactyly family history.
Findings
The patient had elevated serum iron, transferrin saturation, and ferritin levels.
HFE genetic testing confirmed the H63D homozygous mutation.
The patient and relatives underwent genetic counseling and screening.
Abstract
Hereditary hemochromatosis is a genetic disorder caused by mutations in genes regulating hepcidin, leading to increased iron absorption and progressive accumulation in the body. It is commonly encountered in the Western population, but prevalence in the Indian population, especially of the H63D homozygous mutation variant, is on the lower end. Herein is a case of a young male with a paternal hereditary trait of polydactyly, on regular follow-up for anti-hypertensives, who presented with fatigue and multiple large joint pains. Unexplained fatigue, along with a significant family history, warranted further evaluation. Serum iron levels, transferrin saturation, and ferritin levels were elevated. Hence, the patient was referred to the hematology department, for which HFE genetic mutation analysis was done, and a H63D homozygous mutant was noted. Target end-organ damage was assessed. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
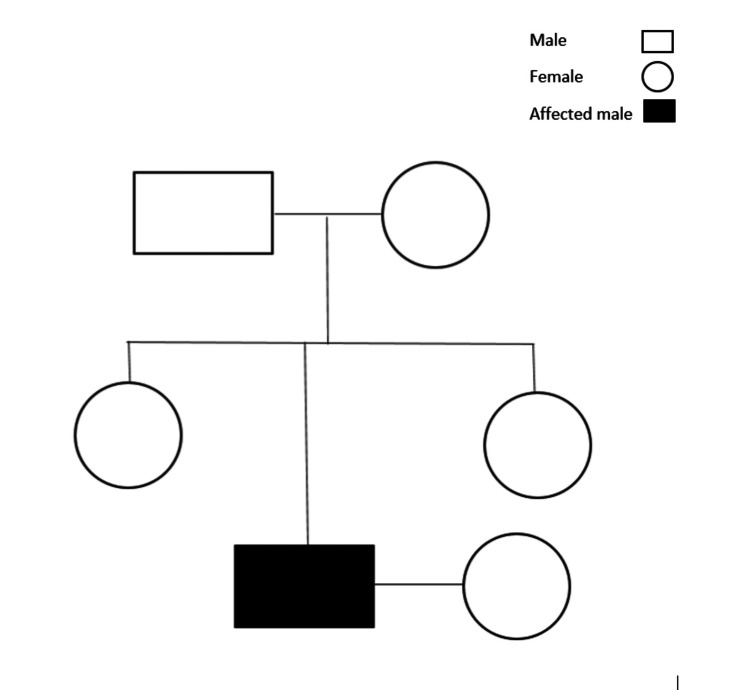 Figure 1
Figure 1| Laboratory investigation | Day 1 | Day 90 | Normal range |
| Hb | 16.5 | 15.9 | 13-17 g/dL |
| MCV | 91.6 | 91 | 83-101 fL |
| MCH | 31.5 | 31.2 | 27-33 pg |
| ESR | 1 | 7 | 0-15 mm/h |
| Serum iron | 178 | 126 | 75-150 mcg/dL |
| TIBC | 334 | 323 | 240-450 mcg/dL |
| T-saturation | 53 | 39 | 20-50% |
| Serum ferritin | 319.8 | 210 | 25-250 ng/mL |
| LDH | 172 | 160 | 100-190 U/L |
| BUN | 19 | 22 | 7-18 mg/dL |
| Serum creatinine | 1 | 1 | 0.6-1.3 mg/dL |
| Total bilirubin | 1 | 1.05 | 0.1-1.2 mg/dL |
| AST | 20 | 26 | 0-35 U/L |
| ALT | 27 | 25 | 0-41 U/L |
| ALP | 62 | 59 | 45-129 U/L |
| GGT | 27 | 25 | 0-73 U/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Hemoglobinopathies and Related Disorders · Biliary and Gastrointestinal Fistulas
Introduction
Hereditary hemochromatosis is an autosomal recessive disorder with low penetrance. It is characterized by increased iron absorption, which leads to total body iron overload. The incidence of an abnormality of increased iron absorption was historically found in the 1980s and 1990s, following the discovery of the HFE gene in 1996. Population screening has found the incidence of 6.4% in White Americans as well as 4-5% in White Europeans and is extremely rare in East Asia (<0.1%). In East Asia, variants in genes other than HFE, such as HJV, HAMP, and TFR2, together known as non-HFE hemochromatosis, are more prevalent [1]. HFE gene homozygosity takes several decades of excess iron absorption without co-existing blood loss to be clinically significant [2]. Incidence of homozygous C282Y is more than H63D, but genetic or environmental modifiers, such as blood transfusion and dietary iron intake, also contribute. Iron accumulates and causes damage through mechanisms that include oxygen free radicals in the liver, heart, pituitary gland, and pancreas; hence, monitoring is imperative [3]. As per Hemochromatosis and Iron Overload Screening (HEIRS) study, 100,000 individuals were evaluated, out of which >10% were found to be homozygous C282Y/C282Y, followed by compound heterozygous C282Y/H63D, homozygous H63D/H63D, and heterozygous (C282Y/wild type or H63D/wild type) [4]. Deposition in the liver generally occurs first, followed by other organs, as iron absorbed from the GI tract passes through the liver first. One analysis done at a tertiary referral center over a 10-year period suggested a significant male predominance among individuals with hereditary hemochromatosis [5].
Case presentation
Presenting history
A young male in his mid-30s, who was a resident of Chennai, India, and a software engineer by profession, with a history of systemic hypertension, being a reformed smoker, and occasional alcohol consumption, presented to our outpatient department for a refill visit. As he entered, at first glance, he appeared to be moderately built and nourished. As a routine check-up, his vitals were checked and recorded as follows: a pulse rate of 86/min and BP of 140/90 mmHg. While going through his history, his regular visits to the orthopedics department in view of complaints of multiple large joint pains sparked concern. The patient had complaints of generalized fatigue.
Examination findings
Examination revealed the evidence of bilateral post-axial polydactyly. On further probing, the patient divulged that it has been a paternal hereditary trait passed on across generations. The patient also mentioned that his father had similar complaints at about the same age, and he also suggested that he had a characteristic skin pigmentation, which led to a lot of stigma. His father was not evaluated for the same. Regarding his family tree, the patient was born of a non-consanguineous marriage; he was the youngest of three siblings, recently married, and planning to have children. With the background of young-onset systemic hypertension, a significant family history, and non-resolving non-specific large joint pains, we further proceeded with a general examination. There were no signs of jaundice, hyperpigmentation, joint tenderness, or subcutaneous nodules. Systemic examination was unremarkable, with no evidence of hepatomegaly.
Diagnostic tests
The patient had brought a file of his recently done blood work-up, complete blood count, renal profile, and liver function tests, all within normal range. The patient had not been on oral iron supplements, with no history of blood transfusion. Considering a paternal hereditary trait of polydactyly, raising suspicion of a coexisting genetic disorder due to a significant family history of skin pigmentation, further work-up done revealed elevated serum iron levels of 178, a transferrin saturation of 53%, and serum ferritin level of 319.80, which prompted a hematology consultation.
HFE genetic mutation analysis by the real-time PCR method was done, which detected H63D homozygous mutant, whereas C282Y and S65C gene mutations were not detected. Further target organ damage assessment revealed USG abdomen, which showed grade 1 fatty liver. A peripheral smear done showed normocytic normochromic anemia, with viral markers being non-reactive. A 2D echo test showed normal chamber dimensions and normal LV function. The CT coronary angiography was normal.
Management plan
The patient’s siblings, parents, and partner were advised to undergo genetic mutation analysis. Though the risk of iron overload in first-degree relatives is low with the H63D homozygous mutant, genetic testing is imperative. As there is a 25% risk of offspring being affected if his partner is a carrier/affected, the patient was counseled along with his partner regarding the implications (Figure 1). Prenatal testing may be considered if both parents are carriers and there is a strong family history. The patient was advised to wait and watch, and a reduction in iron intake and alcohol consumption was advised. The patient has been on regular follow-ups, and the repeat serum iron level after two months was 126, with transferrin saturation levels of 39, which is clinically asymptomatic (Table 1). Genetic mutation analysis, as suggested for the patient’s first-degree relatives and partner, is awaited.
Pedigree analysisSquares represent males, circles represent females, and filled shapes indicate affected individuals. A horizontal line between a square and a circle represents mating. Vertical lines connect parents to offspring.
Discussion
Epidemiology
In young-onset hypertensives with presenting symptoms of generalized fatigue, arthropathy, and screening for hemochromatosis, especially in populations of European descent, is warranted. In India, it is a rare entity, and genetic screening is not routinely recommended. Although studies on primary hemochromatosis in India are underway, associated genetic mutation detection has been a task. HFE gene C282Y mutation has not been found except in one family from South India [6]. Case reports on H63D mutation analysis in North India reported no significant iron overload, but similar reports on South India statistics are limited [7].
Clinical features
Fatigue, especially in the absence of anemia, joint pains, and non-specific symptoms, is commonly seen. Clinical features of iron overload depend on tissue iron amount and contributing factors that can lead to organ dysfunction. The liver, being the principal site of normal iron storage, is the primary site of iron deposition. Cardiac manifestations include dilated cardiomyopathy, diastolic dysfunction, and conduction disturbances. Pancreatic iron overload can lead to type 2 diabetes mellitus, which, combined with skin discoloration, has led to the popular term “bronze diabetes.” Pituitary involvement leads to secondary hypogonadism or hypothyroidism. Other findings include cognitive disturbances and increased susceptibility to infections.
In males, symptoms develop approximately 10 years earlier than females, most likely between 40 and 60 years. In the case discussed, early diagnosis in his mid-30s with no evidence of target end organ damage reduces the risk of life-threatening complications. Hereditary hemochromatosis may be suspected, as in this case, with the presentation of unexplained fatigue, with a probable first- or second-degree relative diagnosed with the same, with high serum ferritin and transferrin saturation (>45%). MRI of the liver and heart, or combined approach, can be used to estimate body iron stores.
Genetic considerations
The presence of post-axial polydactyly with a significant family history raised the possibility of a syndromic presentation. Some genes, like GLI3, have been linked to both post-axial polydactyly and hereditary hemochromatosis [8]. Although the H63D homozygous mutation has lower penetrance, the patient is at risk for iron overload [9]. This case emphasizes the co-occurrence of two distinct genetic conditions in the same individual and the importance of genetic evaluation.
Management options
The goal of treatment is to prevent organ damage due to excess iron [10]. Hence, individuals with iron overload are best treated with phlebotomy. Patients without iron overload who have a homozygous mutant can be monitored regularly, as in the case discussed. In the case of heterozygous mutants, other contributing factors must be addressed.
In this case, the patient’s symptoms were non-specific, but timely diagnosis and genetic counseling have reduced the incidence of complications and the need for phlebotomy. It allows for targeted screening evaluation for asymptomatic relatives at risk [11].
Conclusions
This case highlights the importance of not disregarding any symptom and timely diagnosis of hereditary hemochromatosis, which is a rare entity in India, and regular follow-up will ensure that the patient can live symptom-free without complications. Genetic counseling, especially of first-degree relatives and partners of individuals affected, is imperative. If left untreated, it can lead to early death, including heart failure, cirrhosis, diabetes mellitus, and hepatocellular carcinoma. As reports on hereditary hemochromatosis in South India are limited, this case discussion brings to light the importance of genetic screening tests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The global prevalence of HFE and non-HFE hemochromatosis estimated from analysis of next-generation sequencing data Genet Med Wallace DF Subramaniam VN 6186261820162663354410.1038/gim.2015.140 · doi ↗ · pubmed ↗
- 2HFE gene and hereditary hemochromatosis: a Hu GE review Am J Epidemiol Hanson EH Imperatore G Burke W 1932061542001 https://academic.oup.com/aje/article-abstract/154/3/193/125766?redirected From=fulltext 1147918310.1093/aje/154.3.193 · doi ↗ · pubmed ↗
- 3Iron metabolism: the pathophysiology of iron storage Blood Finch CA Hegsted M Kinney TD 983100851950 https://www.sciencedirect.com/science/article/pii/S 000649712066301714791580 · pubmed ↗
- 4Hereditary hemochromatosis: insights from the Hemochromatosis and Iron Overload Screening (HEIRS) Study Hematology Am Soc Hematol Educ Program Mc Laren GD Gordeuk VR 19520620092000819910.1182/asheducation-2009.1.195PMC 3829617 · doi ↗ · pubmed ↗
- 5Clinical penetrance in hereditary hemochromatosis: estimates of the cumulative incidence of severe liver disease among HFE C 282Y homozygotes Genet Med Grosse SD Gurrin LC Bertalli NA Allen KJ 3833892020182877124710.1038/gim.2017.121PMC 5797490 · doi ↗ · pubmed ↗
- 6Hemochromatosis in India: first report of whole exome sequencing with review of the literature J Clin Exp Hepatol Koshy A Mukkada RJ Chettupuzha AP Francis JV Kandathil JC Mahadevan P 1631691020203218993210.1016/j.jceh.2019.04.051PMC 7067988 · doi ↗ · pubmed ↗
- 7Prevalence of the H 63D mutation of the HFE in north India: its presence does not cause iron overload in beta thalassemia trait Eur J Haematol Garewal G Das R Ahluwalia J Marwaha RK 3333367420051577734610.1111/j.1600-0609.2004.00390.x · doi ↗ · pubmed ↗
- 8GLI 3: a mediator of genetic diseases, development and cancer Cell Commun Signal Matissek SJ Elsawa SF 541820203224549110.1186/s 12964-020-00540-x PMC 7119169 · doi ↗ · pubmed ↗