An Atypical Case of Sjögren's Syndrome: A Surprise Diagnosis
Syed Hassan, Sara Samreen, Faiz Fathima Shaik, Syeda Maariyah Hashmi, Abdul Shafi

TL;DR
A 37-year-old woman with hypokalemic periodic paralysis was diagnosed with Sjögren’s syndrome after showing signs of distal RTA.
Contribution
This paper presents a rare case of Sjögren’s syndrome diagnosed through atypical renal symptoms.
Findings
Hypokalemic periodic paralysis led to the diagnosis of distal RTA in a patient with Sjögren’s syndrome.
Renal involvement in Sjögren’s syndrome is more common than glomerular involvement.
High clinical suspicion is needed for diagnosing Sjögren’s syndrome when hypokalemia is refractory to treatment.
Abstract
Distal renal tubular acidosis (RTA) presenting as hypokalemia, metabolic acidosis, and hypokalemic periodic paralysis is a common manifestation of tubulointerstitial nephritis (TIN) in Sjögren’s syndrome. Sjögren’s syndrome is a chronic, progressive, systemic autoimmune inflammatory disease characterized by lymphocytic infiltration of exocrine glands, which results in sicca syndrome, i.e., xerostomia and keratoconjunctivitis sicca. Some patients can express sicca symptoms with other autoimmune diseases. It is mostly seen in females, and middle-aged women are more likely to be affected. Some patients can present with extra-glandular (systemic) manifestations, of which renal involvement is the most common. Renal involvement in the form of TIN is more common compared to glomerular involvement. We report a case of a 37-year-old female presenting with hypokalemic periodic paralysis, later…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
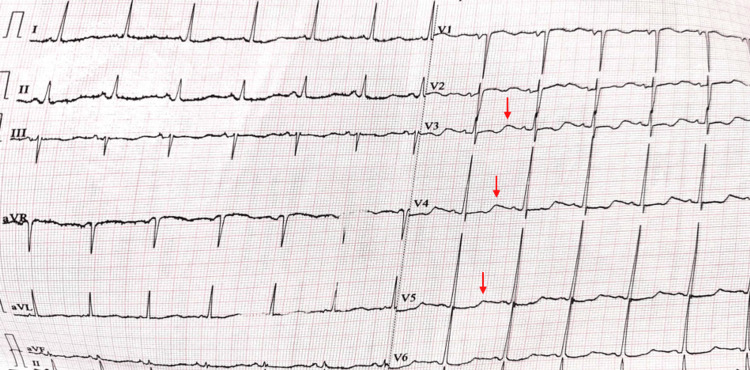 Figure 1
Figure 1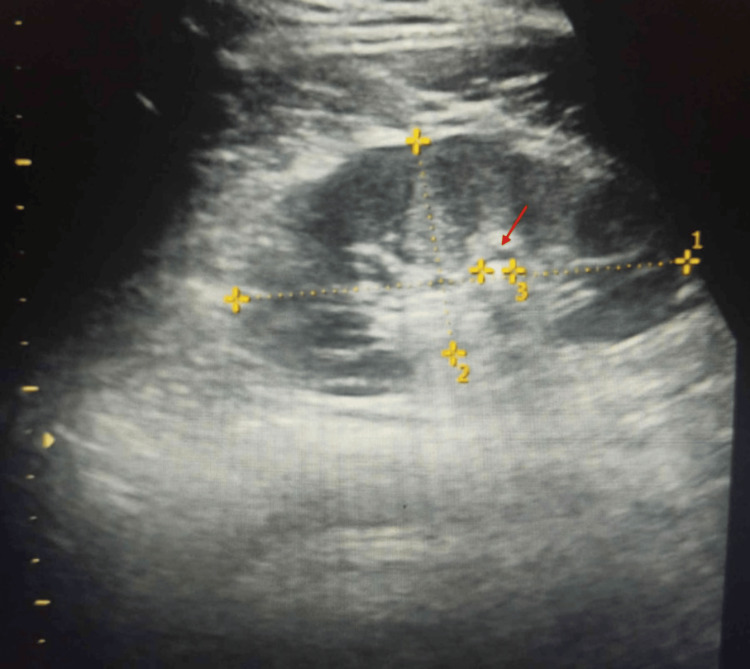 Figure 2
Figure 2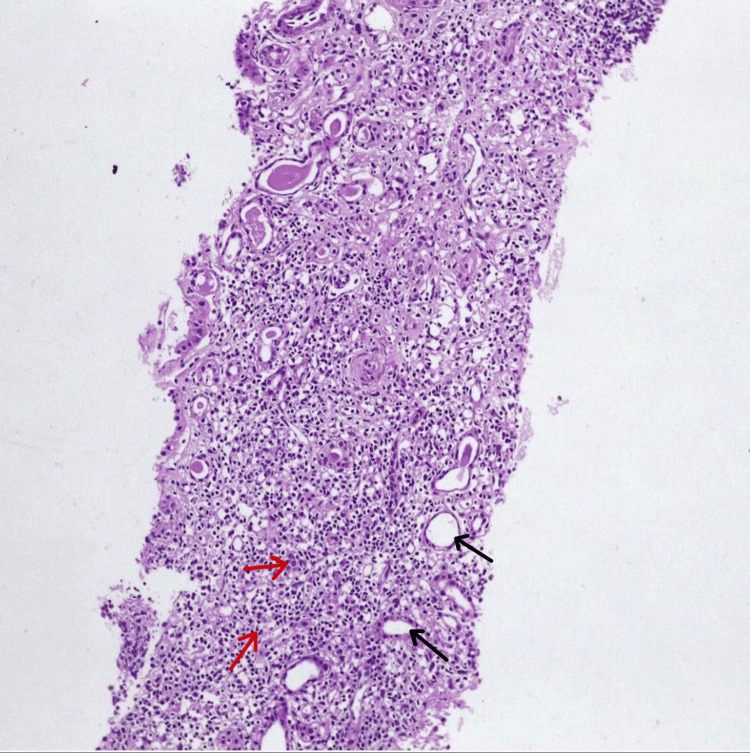 Figure 3
Figure 3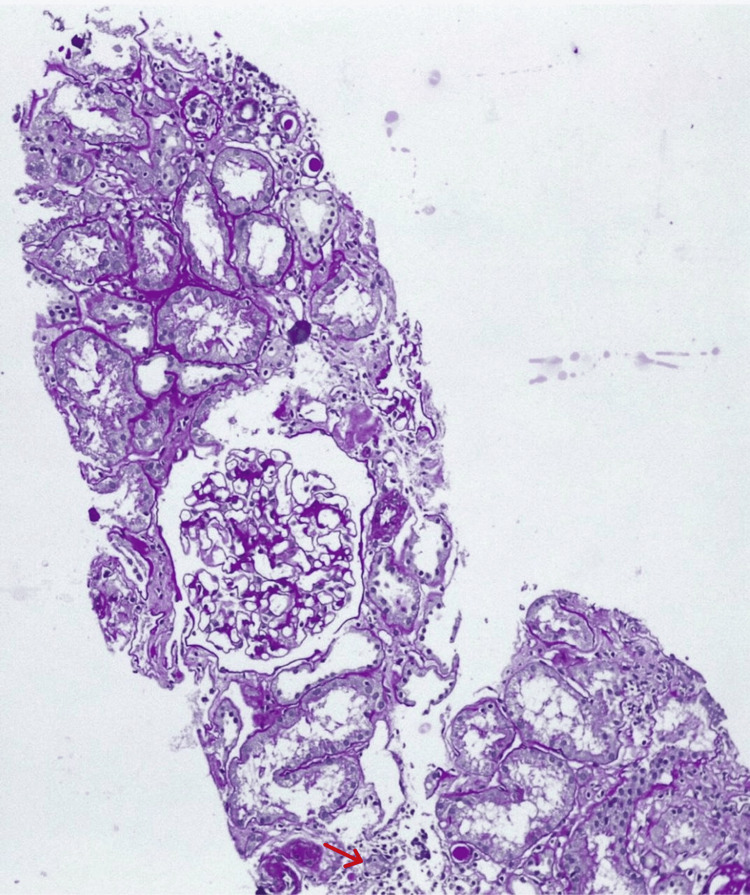 Figure 4
Figure 4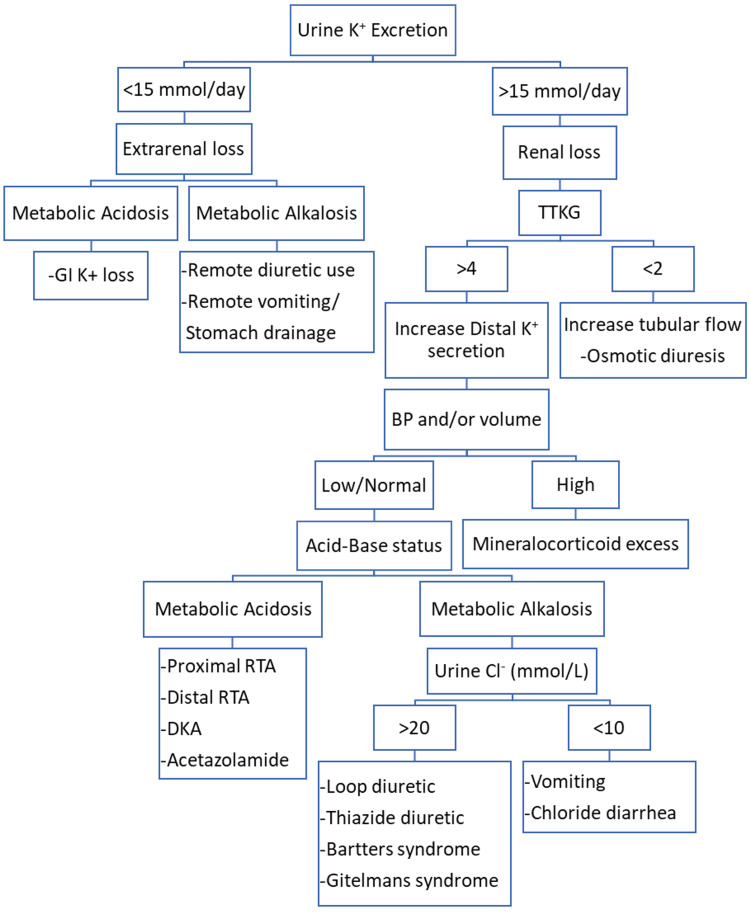 Figure 5
Figure 5| Investigations | Result | Reference range |
| Hemoglobin | 9.2 g/dl | 12.0-15.8 g/dL |
| Mean corpuscular volume | 89 fl | 83-101 fl |
| Mean corpuscular hemoglobin | 26.6 pg | 27-32 pg |
| Mean corpuscular hemoglobin concentration | 29.9 g/dl | 32-36 g/dl |
| RBC count | 3.4 million/cumm | Female: 3.8-5.0 million/cumm |
| WBC count | 4600 cumm | 4000-11000 cumm |
| Platelet count | 2.6 lakhs/cumm | 1.5-4.5 lakhs/cumm |
| Serum iron | 28 mcg/dl | 41-141 mcg/dL |
| Serum ferritin | 852 ng/ml | 10-150 ng/mL |
| Serum TIBC | 320 mcg/dl | 251-406 mcg/dL |
| Transferrin saturation | 12% | 16-35% |
| Serum Na+ | 141 mmol/l | 136-145 mmol/L |
| Serum K+ | 2.6 mmol/l | 3.5-5.0 mmol/L |
| Serum Cl- | 108 mmol/l | 95-105 mmol/L |
| Serum magnesium | 2.2 mg/dl | 1.6-2.3 mg/dL |
| Blood urea | 32 mg/dl | 10-45 mg/dl |
| Serum creatinine | 0.9 mg/dl | 0.6-1.5 mg/dl |
| Urinary potassium (24 hours) | 16 mmol/day | <15 mmol/day |
| Spot urine K+ | 15 mmol/gm creatinine | <13 mmol/gm creatinine |
| Urine pH | 7.8 | 5.5-7.5 |
| Urine sodium | 177 mmol/l | 100-260 mmol/l |
| Urine potassium | 136 mmol/l | 25-125 mmol/l |
| Urine bicarbonate | 5 mmol/L | <1-2 mmol/L |
| Urine protein | 17 mg/dl | 0-15 mg/dl |
| Urine chloride | 217 mmol/L | 110-250 mmol/L |
| Urine phosphorous | 1.2 mg/dl | 0.4-1.3 mg/dl |
| Urine creatinine | 15 mg/dl | 16-327 mg/dl |
| Urine protein creatinine ratio | 1.15 | Normal: <0.2; significant proteinuria: 0.2-3.5; nephrotic syndrome: >3.5 |
| P24 hours urinary protein | 1527 mg/day | <30 mg/day |
| pH | 7.30 | 7.35-7.45 |
| pCO2 | 24 | 32-45 |
| pO2 | 94 | 83-108 |
| Arterial HCO3 | 20.2 | 24-40 |
| Venous bicarbonate | 20.8 mEq/l | 22-29 mEq/l |
| TSH | 3.5 mIU/L | 0.4-4.0 mIU/L |
| T3 | 1.2 ng/ml | 0.8-2.0 ng/mL |
| T4 | 7.2 mcg/dl | 5.0-12.0 mcg/dL |
| Serum 25-OH vitamin D levels | 13.9 ng/ml | 15-80 ng/mL |
| Serum PO4 | 1.2 mg/dl | 2.5-4.3 mg/dL |
| Serum calcium | 7.7 mg/dl | 8.8-10.8 mg/dL |
| Serum albumin | 3.2 g/dl | 3.5-5 g/dL |
| RA factor | <8 IU/ml | <8 IU/ml - negative; ≥8 IU/ml - positive |
| CRP | <6 mg/dl | <6 mg/l - negative; ≥6 mg/l - positive |
| ESR | 1st hour: 90 mm; 2nd hour: 125 mm | Females: 0-20 mm at 1st hour |
| Viral markers (HIV, HbsAg, HCV) | Negative | Not applicable |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Diabetes and associated disorders · Salivary Gland Tumors Diagnosis and Treatment
Introduction
Sjögren's syndrome is a chronic autoimmune inflammatory disease of the exocrine glands, predominantly the salivary and lacrimal glands, leading to sicca symptoms characterized by keratoconjunctivitis sicca and xerostomia. It can be primary (occurring in isolation) or secondary when associated with other autoimmune connective tissue diseases such as rheumatoid arthritis, systemic lupus erythematosus, and scleroderma [1]. It is known to affect middle-aged women with an average female-to-male ratio of 9:1, usually being diagnosed in the fifth decade of life, with a mean age of onset ranging from 51.6 (±13.8) to 62 (±13) years [2].
Apart from classic sicca symptoms, it is also known to involve other organ systems. Extra-glandular manifestations (EGMs) of Sjögren's syndrome are complex and are divided into non-visceral symptoms, including musculoskeletal and cutaneous manifestations, and visceral symptoms, including renal, neurological, hematological, gastrointestinal, cardiovascular, and pulmonary manifestations [3]. Renal involvement in Sjögren's syndrome is rarely defined. The involvement of the kidneys is noted only in 9% of cases with primary Sjögren's syndrome [4]. It is divided into three types: (1) tubulointerstitial nephritis (TIN), characterized by peritubular infiltration of lymphocytes; (2) glomerulonephritis (GN), associated with deposition of immune complexes; and (3) disorders associated with the presence of specific autoantibodies [5]. TIN is found to be the most common histological pattern. Distal renal tubular acidosis (dRTA) is the most common presentation in these patients. Hypokalemia and metabolic acidosis in dRTA cause muscle weakness and periodic paralysis [6]. However, severe hypokalemic periodic paralysis due to dRTA in Sjögren's syndrome is very rare. Here, we report a case of Sjögren's syndrome that presented with hypokalemic periodic paralysis, which was found to be secondary to distal renal tubular acidosis as a consequence of TIN due to Sjögren's syndrome.
Case presentation
A 37-year-old female with no known comorbidities came with complaints of recurrent, relapsing, and remitting patterns of motor weakness of all four limbs for the past three years, with no history of sensory or autonomic dysfunction. She was previously treated as hypokalemic periodic paralysis of unknown cause and responded well to potassium (K+) replacement therapy. On further enquiring, she reported the presence of generalized body pains, dryness of eyes, small joint pains of both the upper limbs, and backache for the past two years.
During the general physical examination, signs of dehydration were noted, including dryness of the mouth, and no dental caries were observed. No obvious parotid gland, submandibular gland, or lacrimal gland enlargement was noted. The thyroid gland was normal in size and non-tender. No lymphadenopathy was noted. Mild joint tenderness of the bilateral proximal interphalangeal joints and metacarpophalangeal joints was observed. Skin examination revealed dryness of the skin with no rash. Her vitals were normal. The cardiovascular, gastrointestinal, and respiratory systems showed no abnormality. Neurological examination revealed that the patient had flaccid weakness of both upper and lower limbs with power of 1/5, no cranial nerve involvement, and no sensory and autonomic dysfunction.
On laboratory investigations, she was found to have iron deficiency anemia and anemia of chronic disease, with hemoglobin at 9.2 gm/dl, mean corpuscular volume of 89 fl, mean corpuscular hemoglobin at 26.6 pg, mean corpuscular hemoglobin concentration of 29.9 g/dl, serum iron at 28 mcg/dl, serum ferritin at 852 ng/ml, serum total iron-binding capacity (TIBC) of 320 mcg/dl, and transferrin saturation of 12%.
Serum electrolytes test showed serum sodium at 141 mmol/l, serum potassium at 2.6 mmol/l, serum chloride at 108 mmol/l, serum bicarbonate at 20.2, normal anion gap (12.8, normal is 8-16), and serum magnesium at 2.2 mg/dl (1.8-2.8 mg/dl). Blood urea was 32 mg/dl, and serum creatinine was 0.9 mg/dl. Markedly decreased potassium levels led us to a workup of hypokalemia.
Urine biochemistry revealed urine pH of 7.8 (alkaline), 24-hour urinary potassium of 16 mmol/day, spot urine potassium creatinine ratio of 15 mmol/gm, transtubular potassium gradient of >5, urine bicarbonate at 5 mmol/L, chloride at 217 mmol/L, phosphorous at 1.2 mg/dl, urine creatinine at 15 mg/dl, urine protein-creatinine ratio of 1.15, and 24-hour urinary protein at 1527 mg/day (proteinuria), which in the setting of hypokalemia suggested renal potassium loss.
Arterial blood gas (ABG) analysis showed normal anion gap metabolic acidosis, with pH of 7.30, partial pressure of carbon dioxide (pCO2) of 24, partial pressure of oxygen (pO2) of 94, arterial bicarbonate (HCO3) of 20.2, and normal anion gap (12.2, normal is 8-16). Venous bicarbonate was 20.8 mEq/l. The urine anion gap was found to be 96, which, in the setting of low potassium and high urinary pH, led us to a diagnosis of type 1 renal tubular acidosis (RTA).
Serum 25-OH vitamin D level was 13.9 ng/ml (normal: >30 ng/ml), serum phosphorus was 1.2 mg/dl, and serum calcium was 7.7 mg/dl. Thyroid profile was normal, with thyroid-stimulating hormone (TSH) at 3.5 mIU/L, T3 at 1.2 ng/ml, and T4 at 7.2 mcg/dl. The renal function test was normal. The liver function test was also normal, except for albumin at 3.2 gm/dl (hypoalbuminemia). Rheumatoid factor was <8 IU/ml (negative), C-reactive protein was <6 mg/dl (negative), and erythrocyte sedimentation rate at first hour was 90 mm and at second hour was 125 mm. Viral markers (HIV, hepatitis B surface antigen, and hepatitis C virus) were negative (Table 1).
ECG showed mild ST depression and U waves (Figure 1). Ultrasound examination showed normal kidneys with 5 mm left renal calculi in the lower pole (Figure 2). Diagnosis of distal RTA was considered, given hypokalemia (vs. hyperkalemia in type 4 RTA), with normal anion gap metabolic acidosis and alkaline urine (vs. acidic urine in type 2 RTA).
ECG in hypokalemia showing ST depressions and U waves.Red arrows showing U waves.
Ultrasound showing a 5 mm kidney stone.Red arrow showing a 5 mm stone.
After working up the case for various causes of responsive hypokalemia and persistent proteinuria, with ABG showing acidosis, an antinuclear antibody (ANA) profile was ordered (ANA titers ≥ 640), which revealed anti-Ro52-3+ (strongly positive), and anti-SSB-3+ (strongly positive).
Based on the clinical picture and ANA profile, a renal biopsy was done, which revealed features of TIN with interstitial inflammation and tubular injury and no significant immune deposits on immunofluorescence. This suggested the diagnosis of Sjögren's syndrome with tubulointerstitial disease (Figures 3, 4).
Renal biopsy showing tubulointerstitial nephritis.Hematoxylin & eosin stain showing infiltrate of mononuclear cells in the interstitium. Magnification is 40x. Black arrows pointing to tubules, and red arrows to inflammation in the interstitium.
Renal biopsy showing tubulointerstitial nephritis.Periodic acid-Schiff (PAS) stain showing few tubules revealing flattened and denuded epithelium with focal mononuclear inflammation in the interstitium. Also, a few tubules showing hyaline casts. Magnification is 40x. Red arrow pointing to tubulitis.
The patient was symptomatically treated for hypokalemia with potassium chloride. She was started on an oral low dose of prednisone 1 mg/kg once daily for four to six weeks, then tapered by 5-10 mg every one to two weeks over three months due to renal involvement (extra-glandular) along with hydroxychloroquine 200 mg once daily, and steroid-sparing drugs. Disease-modifying antirheumatic drug (DMARD), such as methotrexate 10 mg, was started once weekly to prevent long-term usage of steroids and their complications. Sodium bicarbonate was started at 3-4 mEq/kg/day. Artificial eye drops (hydroxypropyl methylcellulose) were used for ocular symptoms. Plenty of oral fluids were advised. The patient was instructed to refrain from using diuretics, tricyclic antidepressants (TCA), and antihistamines. The patient was also told about the high risk of developing lymphoma in the future.
The patient responded well to the treatment and showed significant improvement in her symptoms, with her motor strength being 5/5, and she was able to walk home. Labs were repeated, and potassium levels increased to 3.8 meq/l, which indicated an overall favorable prognosis. The patient was scheduled for a follow-up after three to four weeks, with lab investigations of serum potassium, urine potassium, and 24-hour urine protein to check for her treatment progress.
Discussion
Primary Sjögren's syndrome is a systemic autoimmune disorder that is characterized by focal infiltration of lymphocytes in the exocrine glands, causing symptoms like dry eyes and dry mouth. However, glandular features similar to this can also appear as a late complication in patients having other rheumatic disorders such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and scleroderma (known as secondary Sjögren's syndrome). In approximately 70% of patients with primary Sjögren’s syndrome, anti-Ro and anti-La antibodies are found, usually with ANA positivity [7]. The underlying mechanism is an abnormal response of B and T cells to the autoantigens Ro/SSA and La/SSB, which destroy the exocrine gland epithelium [8]. The prevalence of Sjögren's syndrome is worldwide, with more cases being reported in adults than children, and no racial or geographic bias in incidence. The disorder has a marked predilection for females. It can affect any age group, but usually, symptoms appear in middle age, i.e., between the ages of 45 and 55 years [9].
Clinicians often find it difficult to diagnose Sjögren's syndrome as it exhibits a broad spectrum of clinical manifestations, ranging from mild exocrine symptoms of dry eyes, dry mouth, and myalgias to severe systemic disease leading to potentially life-threatening complications [10]. Thus, the disease usually goes undiagnosed when the patient’s initial presentation differs from the commonly encountered exocrine symptoms of dry eyes and mouth. This is due to the general emphasis on ocular and oral findings as diagnostic criteria. The American-European Consensus Group classification criteria require the presence of four of six criteria for the diagnosis of Sjögren's, which include (a) ocular or oral symptoms, (b) objective ocular or oral signs, (c) the presence of autoantibodies, and (d) histopathology from lip biopsy. In our patient, we found three out of the six criteria (dry eyes and mouth, and positive anti-SS-A and anti-SS-B antibodies), suggesting a possible diagnosis of primary Sjögren’s. Renal biopsy findings are not a part of the diagnostic criteria for Sjögren’s, but they can aid in diagnosis [11]. Renal involvement in primary Sjögren’s syndrome (pSS) was first documented in the 1960s, describing typical tubular defects [12]. The kidney is known to be the most affected non-exocrine organ, with the prevalence ranging between 2% and 67%. Interstitial nephritis is the most common type, followed by dRTA, nephrogenic diabetes insipidus, and glomerular diseases, which commonly include membranoproliferative glomerulonephritis (MPGN) and membranous nephropathy (MN) [13]. Interstitial nephritis (IN) evolves slowly, causing low-grade inflammation and occurs before or near the onset of typical sicca symptoms. Cryoglobulinemic glomerulonephritis in Sjögren's syndrome results from immune complex deposition. GN has an abrupt onset than IN but occurs late in the course of Sjogren's disease as nephritic syndrome with impaired renal function [14].
Clinically, the most common electrolyte imbalance observed is hypokalemia. Figure 5 shows an approach to hypokalemia [15]. There are many causes of hypokalemia, which can be classified into three types: excessive excretion, insufficient intake of potassium, or changes in the distribution of intracellular and extracellular potassium levels. Endocrine diseases with renal potassium loss cause hypokalemia, which includes congenital adrenal hyperplasia, primary aldosteronism, RTA, Bartter syndrome, and Liddle syndrome. Thus, it is necessary to identify whether renal potassium loss has occurred [16]. RTA in Sjögren’s due to TIN is characterized by distal (type I) RTA, which is more common than proximal (type II) RTA (Fanconi syndrome) [17]. Pathogenesis of hypokalemia in RTA includes decreased delivery of sodium and hydrogen in the distal tubule, defective H+-ATPase activity, bicarbonate excretion, and secondary hyperaldosteronism leading to alkaline pH. Hypokalemic paralysis is usually seen three months to four years before the onset of typical symptoms of keratoconjunctivitis sicca in patients with Sjögren’s syndrome secondary to distal RTA [4]. Autoantibodies to NaCl cotransporter and carbonic anhydrase enzymes have been identified in patients with primary Sjögren’s syndrome and correlated with RTA [18].
Approach to hypokalemia.TTKG: transtubular K+ concentration gradient; GI: gastrointestinal; RTA: renal tubular acidosis; DKA: diabetic ketoacidosis.Source: [15]. Figure credits: Sara Samreen and Syed Hassan.
Distal RTA occurs due to a defect in the distal nephron, which increases back-diffusion of hydrogen ions from the collecting duct lumen to the blood or inadequate transport of hydrogen ions. The defect in hydrogen ion secretion also impairs ammonia secretion from the distal tubule, which impairs the ability of nephrons to acidify the urine. Thus, the urine pH cannot be lowered normally. This results in normal anion gap metabolic acidosis with an alkaline pH of urine (greater than 5.5). It also causes hypokalemia due to potassium excretion. However, severe hypokalemia causing paralysis as an initial presentation of dRTA is a rare occurrence in secondary Sjögren’s [19].
Hypokalemic periodic paralysis, one of the inherited channelopathies, caused by mutations in the gene that regulates sodium or potassium channels, is often on the differential diagnosis as it causes episodes of weakness or paralysis secondary to low potassium levels. Other channelopathies include hyperkalemic periodic paralysis, which is caused by mutations in sodium channels, leading to paralysis that is triggered by high levels of potassium, and Andersen-Tawil syndrome, which is a rare condition caused by mutations in potassium channels, often associated with periodic paralysis, arrhythmias, and other presentations [10].
Hyperthyroidism and hypothyroidism can cause muscle weakness and episodes of paralysis, thus, it becomes essential to work up a patient to rule out these conditions, particularly in individuals who have a predisposition to periodic paralysis [10].
Chronic acidosis leads to proximal reabsorption of citrate, bone resorption, alkaline urine, and hypocitraturia, and hypercalciuria will lead to nephrolithiasis or nephrocalcinosis [18]. Patients with pSS and TIN or glomerular disease usually have a favorable diagnosis, but a high risk of chronic kidney disease is present in patients with TIN. Therefore, screening must be performed by checking the urine protein/creatinine ratio in patients with systemic pSS at least once a year to detect renal complications early [20].
Sjögren’s syndrome in patients with sicca symptoms requires secretagogues like hydroxypropyl methylcellulose and polyvinyl alcohol 0.5%. Topical cyclosporine eye drops can also be used for refractory sicca symptoms, and corneal patches and boric acid ointment can be used if corneal ulcerations are present. Propionic acid gels are used for vaginal dryness. To stimulate secretions, pilocarpine (5 mg thrice daily) and cevimeline (30 mg thrice daily) are used. Patients of Sjogren's with mild joint symptoms such as mild arthritis, arthralgia, and myalgia are treated with nonsteroidal anti-inflammatory drugs (NSAIDs) in anti-inflammatory doses given daily or as needed, depending upon symptom frequency. Those not responding to NSAIDs and with moderate to severe symptoms require DMARDs such as hydroxychloroquine or low-dose weekly methotrexate, depending upon the severity of symptoms. Patients with RTA are treated with sodium bicarbonate (0.5-2 mmol/kg in four divided doses). Patients with systemic manifestations will require additional monoclonal antibodies like rituximab and glucocorticoids [15]. Although corticosteroids are the preferred treatment of choice in TIN, the question of their benefit in pSS associated with TIN is still unclear. Other treatment options are considered in patients who are intolerant to steroids or those with refractory disease. The use of mycophenolate mofetil resulted in a significant improvement in kidney function [1].
Conclusions
The atypical presentation of Sjögren's syndrome with hypokalemia leads to diagnostic delay, as further investigations are not usually done in the absence of classic Sjögren's symptoms and lead to misdiagnosis of recurrent and relapsing hypokalemic periodic paralysis.
In patients presenting with hypokalemic periodic paralysis, proper evaluation should be done to determine the cause of hypokalemia. When labs suggest normal anion gap metabolic acidosis in the presence of renal potassium loss, dRTA in Sjögren's syndrome should be considered, especially in young women. Further investigation with ABG, urine analysis, serological profile for antibodies, and, if required, renal biopsy should be considered so that early diagnosis and treatment can be initiated with low-dose corticosteroid, potassium, and bicarbonate replacement to prevent life-threatening complications and death.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Renal disease in primary Sjögren's syndrome Rheumatol Ther Aiyegbusi O Mc Gregor L Mc Geoch L Kipgen D Geddes CC Stevens KI 6380820213336796610.1007/s 40744-020-00264-x PMC 7991017 · doi ↗ · pubmed ↗
- 2Sjögren's syndrome: a systemic autoimmune disease Clin Exp Med Negrini S Emmi G Greco M 9252220223410016010.1007/s 10238-021-00728-6PMC 8863725 · doi ↗ · pubmed ↗
- 3The spectrum of extraglandular manifestations in primary Sjögren’s syndrome J Pers Med Mihai A Caruntu C Jurcut C 9611320233737395010.3390/jpm 13060961 PMC 10305413 · doi ↗ · pubmed ↗
- 4Sjogren’s syndrome presenting as hypokalemic periodic paralysis, a rare manifestation: a case series Natl J Physiol Pharm Pharmacol Mohanty N Nageswar M Rout S Mishra S 11331135132023 https://www.ejmanager.com/mnstemps/28/28-1678174382.pdf?t=1748104787
- 5Current state of knowledge on primary Sjögren’s syndrome, an autoimmune exocrinopathy J Clin Med Parisis D Chivasso C Perret J Soyfoo MS Delporte C 2299920203269840010.3390/jcm 9072299 PMC 7408693 · doi ↗ · pubmed ↗
- 6Renal tubular acidosis in patients with primary Sjögren’s syndrome Electrolyte Blood Press Jung SW Park EJ Kim JS 17221520172904290310.5049/EBP.2017.15.1.17PMC 5641498 · doi ↗ · pubmed ↗
- 7Primary Sjögren's syndrome Lupus Bowman SJ 32352720183045232910.1177/0961203318801673 · doi ↗ · pubmed ↗
- 8Sjögren syndrome Nat Rev Dis Primers Brito-Zerón P Baldini C Bootsma H 16047220162738344510.1038/nrdp.2016.47 · doi ↗ · pubmed ↗