Out-of-pocket medical costs in relation to resection of colorectal liver metastases in the Australian healthcare system
Nazim Bhimani, Rebecca Seton, David Chan, Mbathio Dieng, Patrick J. Kelly, Thomas J. Hugh

TL;DR
This study examines the out-of-pocket medical costs for patients undergoing liver resection for colorectal liver metastases in Australia and their financial impact.
Contribution
The study provides new insights into patient-level out-of-pocket costs and financial stress related to liver resection for CRLM in Australia.
Findings
Liver surgical treatment had the highest median out-of-pocket cost of $1011.29.
Most patients were not worried about out-of-pocket costs and reported no significant financial impact.
Specialist consultation costs had a median out-of-pocket cost of $393.35.
Abstract
The cost of treating colorectal liver metastases (CRLM) places a financial burden on the healthcare system; however, there is limited research on the out-of-pocket (OOP) costs to patients. This study aimed to assess the direct medical OOP costs on patients who undergo liver resection for CRLM and evaluate their financial worry, stress, and difficulty. This was a retrospective cohort analysis of the OOP costs for patients who underwent potentially curative resection of CRLM in Sydney, Australia, between 2010 and June 2021. These costs were determined in Australian dollars from the diagnosis of liver metastases to their last follow-up. Patients completed a series of questions relating to financial worry, stress, and difficulty. In total, 121 patients underwent liver resection, of which 85 were alive at a median follow-up of 5.3 years (1.8–13.7). There was a 59% response rate (50/85).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
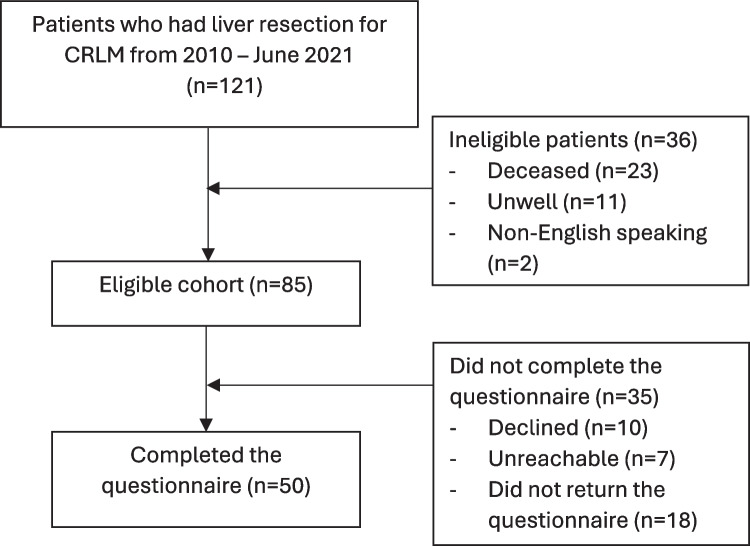 Figure 1
Figure 1- —University of Sydney
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEconomic and Financial Impacts of Cancer · Pancreatic and Hepatic Oncology Research · Colorectal Cancer Screening and Detection
Introduction
The cost of treating cancer can place a heavy burden on the healthcare system, patients, and their families [1]. From diagnosis to treatment, and then from survivorship to end-of-life care, the costs for some patients may be significant. These can be divided into medical and non-medical costs [2]. Medical costs include consultations, investigations, hospital admissions, surgical or radiological interventions, and medications [2, 3]. Non-medical costs include transport, food, and loss of productivity [2, 3], and these later are usually the sole responsibility of the patients and their caregivers.
The Australian healthcare system is complex, and there is inconsistent integration of health service delivery, which consists of both public and private entities. Public healthcare includes medication support provided by the Pharmaceutical Benefits Scheme (PBS), medical services support through the Medicare Benefits Scheme (MBS), and public hospital services funded by state governments [4]. Some health services for treating cancer are also provided by private hospitals, private clinics, and private organisations, and there is partial funding support for these from private health insurance. Regardless, patients often still incur additional out-of-pocket (OOP) costs, as the fees charged by private health service providers vary by the type of provider and their location.
Despite having private insurance cover, patients treated in private hospitals may face higher OOP costs for surgical interventions and procedures compared to public hospital patients due to the gaps in coverage. These gaps may include paying the hospital excess fees or differences between scheduled rebates and actual costs charged by specialists. Despite most people knowing and accepting that there will likely be OOP costs, 44.8% of Australians elect to take out private insurance, and in New South Wales, this rate is even higher at 46.2% [5]. Reasons for selecting private treatment over public treatment vary but include a sense of certainty about timely treatment, the ability to choose a specialist, and a desire to avoid the government imposed surcharge for not having private health insurance [6].
Navigating through a fragmented healthcare system can be difficult for patients and their families, with the need to access care from different healthcare providers in different locations. This is problematic given the disease burden in the community, with 50% of Australians having at least one chronic condition requiring integrated care [6].
In Australia, colorectal cancer (CRC) is the third most common cancer [7]. Unfortunately, many patients either present with metastatic disease or go on to develop metastatic disease [8]. Those with isolated colorectal liver metastases (CRLM) may be able to undergo curative liver resection, with an expectation of a cure and a return to normal life [9]. In many countries, CRC is also associated with significant costs for both the patient and society. Internationally, the average overall cost of treating metastatic CRC ranges from 293,461 [10]. To date, there has been no research focusing on the OOP medical costs and the associated financial stress for patients treated for CRLM.
Given the multifaceted Australian healthcare system, we hypothesise that the median OOP medical costs will be variable, but that patients who achieve long-term cure are not likely to express financial burden or worry about these costs. This study aimed to identify the median OOP medical costs in patients who underwent a potentially curative liver resection of CRLM in the Australian health system and to examine any financial burden or worry about treatment costs.
Methods
A single-unit cohort study of patients who had potentially curative resection for CRLM between 2010 and June 2021 at two hospitals (Royal North Shore Hospital and North Shore Private Hospital) was undertaken. Ethics approval was given by the Northern Sydney Local Health District Human Research Ethics Committee (LNR/11/HAWKE/258). Patients with CRLM who underwent curative resection and had at least 1-year follow-up were retrospectively identified from a prospectively collected database. Patients who underwent resection before 2010 were not included in the study as biological agents (cetuximab and bevacizumab) were not available or were not routinely used before this.
The questionnaire was developed using validated financial burden questions from studies by Markman et al. and Veenstra et al. [11, 12]. A list of these questions can be found in the Appendix. Patients were contacted by telephone before posting a questionnaire. Patients who did not return the questionnaire after 3 months were contacted again and encouraged to participate. The questionnaire consisted of demographic details and financial burden and worry. Demographic details included gender, date of birth, marital status, employment status, education, household income, private health insurance, and the number of adults and children in the house. Financial burden and worry included questions on how worried patients were about their financial problems measured on a five-point Likert scale, the financial burden on the ability to make ends meet, and the impact it had on finances on a seven-point Likert scale.
A detailed patient timeline from diagnosis of liver metastases to 2022 was constructed, listing all public and private hospital admissions, private consultation visits, operation details, chemotherapy, and radiation therapy doses. Costs of imaging, blood tests, and general practitioner visits were not examined as it was assumed that Medicare (funded by the government) covered these costs and that there were mostly no OOP costs. Surgical and procedural costs only included the primary surgeon fees, not the assisting surgeon or anaesthetist’s fees. Due to the difficulty of determining what medications were taken and how much, this was also not considered for this study. For the sake of a consistent approach and because this was relatively easy to measure, the costs for consultations and operations were assumed to be the Australian Medical Association (AMA) fee, with the OOP cost calculated as the difference between the AMA fee and the Medicare scheduled rebate. Radiation therapy, chemotherapy, immunotherapy, and radiation oncology and medical oncology consultations performed in the public hospital incurred no OOP costs. For the same treatment obtained in private hospitals, patients only paid the yearly hospital excess to the private health fund and paid the OOP cost set by the PBS for chemotherapy. All costs were adjusted for inflation using an inflation calculator (https://www.rba.gov.au/calculator/) and presented in Australian dollars as of 2022.
Information obtained from the database included demographical data (age, sex, marital status, employment status, education level, household income), pre-existing medical conditions (Charlson comorbidity index (CCI) and American Society of Anesthesiologists (ASA)), radiological investigations (timing, primary side), neoadjuvant treatments (chemotherapy ± biological agents, radiotherapy, transarterial chemoembolisation (TACE), selective internal radiation therapy (SIRT), live ablation, portal vein embolisation), intra-operative details (operative technique, extent of liver resection, resection margin, tumour differentiation), post-operative outcomes (complications, length of stay, recurrence), and post-operative treatment (chemotherapy ± biological agents, liver ablation, locoregional therapy). Neoadjuvant chemotherapy or biological agent treatments were defined as treatment given at any time 6 months before the liver resection. The extent of the liver resection was defined as either major or minor, where a major liver resection was a resection of at least three contiguous Couinaud segments. Long-term survival was defined as greater than or equal to 5 years.
Categorical variables were presented as counts and percentages and analysed using Chi-squared tests or Fisher’s exact test. Continuous variables were expressed as a mean and standard deviation for normally distributed data and analysed using T tests. Continuous variables not normally distributed were expressed as a median and range and analysed using the Mann–Whitney U test. All statistical analyses were performed using Stata® BE for Windows® version 17.1 (StataCorp, College Station, TX, USA).
Results
From 2010 to June 2021, 121 patients underwent liver resection for CRLM. Of these, 23 patients (19%) were deceased, 11 patients (9%) were too unwell to complete the questionnaire, and two patients (2%) were deemed unsuitable for the study as they were unable to speak English. The cohort of interest consisted of 85 patients. Ten patients declined to complete the questionnaire for an unspecified reason, seven patients were unreachable after three attempts at contact, and 18 patients did not return the questionnaire and were therefore excluded. The final cohort included 50 respondents (59% response rate), and these are the subjects of this study, as shown in Fig. 1. The median follow-up from diagnosis of CRLM to determine OOP costs was 5.3 years (range 1.8–13.7).Fig. 1. Flow chart of patients included in the study
Demographic characteristics are shown in Table 1. Most survey participants were men (60%), and the median age at the time of completion of the survey was 69 years. Most were either married or living as a married couple (72%), were retired (60%), and had at least completed high school (84%). When the patient was the primary earner in the household, 38% were earning ≥ 19,999 39,999 59,999 79,999 99,999 119,999 139,999 159,999 179,999 Above $200,0005 (10)11 (22)6 (12)9 (18)3 (6)6 (12)1 (2)2 (4)2 (4)5 (10)Main earner in the household, n (%) Patient with cancer Spouse Shared between survivor/spouse22 (44)10 (20)18 (36)Private health Insurance, n (%) Yes No33 (66)17 (34)Adults in household, n (%) 1 2 3 or more9 (18)32 (64)9 (18)Children in household, n (%) 0 1 or 239 (78)11 (22)
Table 2 describes the tumour characteristics and treatment received. Most patients had the primary tumour removed first (82%), had a Dukes C tumour (62%), had a left-sided primary tumour (82%), presented with synchronous disease (56%), received neoadjuvant chemotherapy (82%), had a minor liver resection (76%), did not have a complication after liver resection (59%), received postoperative chemotherapy (96%), and did not develop recurrent disease (58%). Table 2. Tumour biology and treatment receivedVariablen (%)Primary resection detailsOrder of resection Primary first Liver first Combined41 (82)2 (4)7 (14)Dukes stage Dukes A Dukes B Dukes C3 (6)16 (32)31 (62)Primary site Colon Rectum30 (60)20 (40)Sidedness Left Right41 (82)9 (18)Timing of liver metastases Metachronous Synchronous22 (44)28 (56)Treatment prior to liver resection Neoadjuvant chemotherapy41 (82) SBRT OR chemoradiotherapy4 (8) TACE0 (0) SIRT0 (0) RFA or MVA0 (0) Portal vein embolisation1 (2) None5 (10)Liver operative details (n = 59)Operative technique Open Laparoscopic Laparoscopic converted to open51 (87)6 (10)2 (3)Liver resection Major Minor14 (24)45 (76)Median length of stay in days (range)7 (3–30)Complications24 (41)Tumour differentiation Well Moderate Poor Not stated5 (9)29 (51)1 (2)22 (39)Treatment and outcomes following liver resection(s) (n = 50) Chemotherapy48 (96) SBRT8 (16) Chemoembolisation/TACE1 (2) SIRT1 (2) ETOH ablation0 (0) RFA or MVA2 (4) Recurrence21 (42)
Table 3 summarises the median direct medical OOP costs for treating CRLM. The OOP cost of a consultation with a colorectal surgeon, liver surgeon, and gastroenterologist were similar. The complexity of liver resection was reflected in the higher OOP costs with a median OOP cost of 0 (range 0–4632.25). Another likely reason for this difference is that costs were determined from the diagnosis of liver metastases rather than the diagnosis of the primary bowel cancer, and so some costs associated with the treatment by the colorectal surgeon were not included in the analysis. There are no costs for consultations with a radiation oncologist or for radiation therapy, as all patients were treated in public hospitals and consequently would not have had an OOP cost. Similarly, the median cost for chemotherapy was only 57,500 for their treatment. The overall median OOP cost per person is 673.50 per year. In this study, 15 patients (30%) had their entire treatment in the public sector, 14 patients (28%) had their entire treatment in the private sector, and 21 patients (42%) had a mix of treatment in the public and private sectors. Table 3. Direct medical OOP costs with median and range for treating CRLM in AUD by treatment facilityTreatmentOverall OOP cost (n = 50)Liver Consultations Surgical treatment186.3 (0–363.4)1011.29 (0–7246.54)Colorectal Consultations Surgical treatment204.98 (0–1058)0 (0–4632.25)Chemotherapy29 (0–57502)Radiation oncology0 (0–0)Gastroenterologist Consultations Procedures186.7 (0–492.85)0 (0–174.95)Hospital excess750 (0–5000)Overall costs4091.88 (232–57,690.45)
Table 4 summarises the financial burden and worry in the diagnosis, treatment, and follow-up of CRLM. Most patients were not worried about OOP costs or were only slightly worried about their financial problems (60%) during or after their treatment. Similarly, most patients suggested that there was no impact on their ability to make ends meet (64%) or that there was no impact on their finances (56%). Sixty per cent of patients used their savings to pay for their OOP while another 20% used savings and other sources, including borrowing money or taking a loan, cutting down on spending on food, clothes, recreational activities or expenses in general, selling stocks or investments. One patient decided to sell their home as part of downsizing but also to help fund their cancer care. Despite some patients having to find additional funds to cover the cost of their treatment, only 22% of patients in this cohort felt that they spent more money than they had expected, while the majority (68%) thought that the amount of medical benefits received was either more than they expected or about what they expected. Only 26% of patients considered the cost when selecting a treatment course. There were no patients who decided not to have a recommended cancer treatment because of the costs. Table 4. Financial burden and worry in the diagnosis, treatment, and follow-up of CRLMVariablen (%)Worry about financial problems Not at all Slightly Moderately/somewhat Very much Extremely22 (44)8 (16)10 (20)10 (20)0 (0)Impact on the ability to make ends meet Very difficult Difficult Somewhat difficult Normal Somewhat easy Easy Very easy3 (6)3 (6)12 (24)25 (50)1 (2)3 (6)3 (6)Illness has had no impact on finances Strongly disagree Disagree Somewhat disagree Neither agree nor disagree Somewhat agree Agree Strongly agree4 (8)10 (20)8 (16)5 (10)12 (24)6 (12)5 (10)How did they pay Used savings Borrowed money or took a loan Could not make payments on credit cards or other bills Cut down on spending on food and/or clothes Cut down on spending on health care for other family members Cut down on recreational activities Cut down on expenses in general Sold some personal items/possessions, e.g. car, jewellery Sold stocks or investments Sold their home43 (86)3 (6)1 (2)5 (10)0 (0)5 (10)16 (32)1 (2)3 (6)1 (2)Describe your reaction to the cost of treating cancer Spent more money than I had expected Spent about what I expected Spent less than I expected13 (26)21 (42)16 (32)Describe your reaction to how your medical benefits covered the cost of treating cancer Contributed more money than I expected Contributed about what I expected Contributed less money than I had expected12 (24)22 (44)16 (32)When choosing a treatment course for your cancer, did you consider the cost of treatment? No, not at all Yes, a little bit Yes, a great deal37 (74)11 (22)2 (4)Did you decide not to have a recommended cancer treatment because it was too expensive? No Yes Do not know/not sure48 (96)0 (0)2 (4)
Tables 5 and 6 examine the relationship between patient and disease factors and financial worry and financial difficulty, respectively. The following factors had no impact on financial worry or financial difficulty: having multiple liver resections, undergoing any chemotherapy, whether they were on active treatment, had recurrent disease, the annual household salary, cohabitation status, education level, who the primary household earner was, having private health insurance, or gender of the patient. Interestingly, patients who had complications following liver resection expressed greater financial difficulty (67% vs. 38%, p = 0.048); however, there was no difference in financial worry (p = 0.729). Similarly, working patients expressed greater financial difficulty compared with non-working patients (61% vs. 25%, p = 0.012); however, there was no difference in financial worry (p = 0.153). Patients with children had greater financial worry than those who did not have children (40% vs. 10%, p = 0.017); however, there was no difference in financial difficulty (p = 0.147). Younger patients were more likely to have financial worry (60% vs. 20%, p = 0.004) and financial difficulty (78% vs. 13%, p < 0.001) than older patients. Table 5. Relationship between financial worry and patient/disease factorsTotal cohort (n = 50)No or slightly worried (n = 30)Moderate or very much (n = 20)p valueLiver resection complications 0.729 Yes No24 (48)26 (52)15 (50)15 (50)9 (45)11 (55)Multiple liver resections 0.450 Yes No8 (16)42 (84)6 (20)24 (80)2 (10)18 (90)Any chemotherapy 0.118 Yes No36 (72)14 (28)19 (63)11 (37)17 (85)3 (15)Currently receiving treatment 0.676 Yes No11 (22)39 (78)6 (20)24 (80)5 (25)15 (75)Recurrence 0.349 Yes No21 (42)29 (58)11 (37)19 (63)10 (50)10 (50)Annual household income 0.812 < 80,00031 (62)19 (38)19 (63)11 (37)12 (60)8 (40)Cohabitation status 0.353 Single Couple14 (28)36 (72)10 (33)20 (67)4 (20)16 (80)Employment status 0.153 Employed Non-employed19 (38)31 (62)9 (30)21 (70)10 (50)10 (50)Education level 0.487 Tertiary educated No tertiary education27 (54)23 (46)15 (50)15 (50)12 (60)8 (40)Children in household 0.017 0 1 or 239 (78)11 (22)27 (90)3 (10)12 (60)8 (40)Main household earner 0.999 Patient with cancer Spouse Shared22 (44)10 (20)18 (36)13 (43)6 (20)11 (37)9 (45)4 (20)7 (35)Private health insurance 0.626 Yes No33 (66)17 (34)19 (63)11 (37)14 (70)6 (30)Age at survey 0.004 < 65 ≥ 6518 (36)32 (64)6 (20)24 (80)12 (60)8 (40)Gender 0.077 Male Female30 (60)20 (40)15 (50)15 (50)15 (75)5 (25)Table 6. Relationship between financial difficulty and patient/disease factorsTotal cohort (n = 50)Difficult (n = 18)Not difficult (n = 32)*p *valueLiver resection complications0.048 Yes No24 (48)26 (52)12 (67)6 (50)12 (38)20 (62)Multiple liver resections0.999 Yes No8 (16)42 (84)3 (17)15 (83)5 (16)27 (84)Any chemotherapy0.744 Yes No36 (72)14 (28)14 (78)4 (22)22 (69)10 (31)Currently receiving treatment0.147 Yes No11 (22)39 (78)6 (33)12 (67)5 (16)27 (84)Recurrence 0.145 Yes No21 (42)29 (58)10 (56)8 (44)11 (34)21 (66)Annual household income0.055 < 80,00031 (62)19 (38)8 (44)10 (56)23 (72)9 (28)Cohabitation status0.999 Single Couple14 (28)36 (72)5 (28)13 (72)9 (28)23 (72)Employment status0.012 Employed Non-employed19 (38)31 (62)11 (61)7 (39)8 (25)24 (75)Education level0.178 Tertiary educated No tertiary education27 (54)23 (46)12 (67)6 (33)15 (47)17 (53)Children in household0.147 0 1 or 239 (78)11 (22)12 (67)6 (33)27 (84)5 (16)Main household earner0.298 Patient with cancer Spouse Shared22 (44)10 (20)18 (36)9 (50)5 (28)4 (22)13 (41)5 (15)14 (44)Private health insurance0.999 Yes No33 (66)17 (34)12 (67)6 (33)21 (66)11 (34)Age at survey< 0.001 < 65 ≥ 6518 (36)32 (64)14 (78)4 (22)4 (13)28 (87)Gender 0.904 Male Female30 (60)20 (40)11 (61)7 (39)19 (59)13 (41)
Discussion
The OOP costs for patients who had a potentially curative resection of CRLM in Australia are manageable, and, in general, patients do not often report financial difficulty or stress. These findings differ from the OOP costs for CRC in other parts of the world, such as China, the USA, and Malaysia [13–15]. This is the first Australian study to assess the median OOP cost from the diagnosis of CRLM and the clinical factors associated with financial worry and financial difficulty. OOP costs were highest in relation to the surgical treatment rather than medical or radiation oncological treatments. Patients who reported financial worry and difficulty were mostly younger patients who have children.
Two other international studies of patients with CRC found that OOP costs related to surgical treatment are high compared to radiotherapy and chemotherapy costs [16, 17]. Azzani et al. found similar findings across all cancer stages. Newton et al. looked at four different cancer types, including CRC, in rural Western Australia and found that surgery OOP costs were the highest [18]. Surprisingly, the total appointment OOP costs for all specialists were more expensive than the OOP costs of chemotherapy and radiotherapy individually. This may be because many specialists see patients in their private rooms as the public hospital outpatient clinics may not be available or be suitable. Private rooms are expensive to maintain, and so specialists need to charge to cover their costs. Furthermore, OOP costs are influenced by the fact that medical scheduled rebates have not kept up with inflation, with only an annual average indexation of 1.1% [19].
Interestingly, in a country with a universal healthcare system such as Malaysia, Azzani et al. showed that patients had some level of financial difficulty at the time of their diagnosis (94.2%), and at the 6-month (85.5%) and 12-month follow-up period (77.2%) [17]. To cope with the financial burden, most patients used their current income and savings, like the findings of the present study. Similarly, Veenstra et al. identified patients with CRC from the surveillance, epidemiology and end results cancer registry and found that most had some level of financial burden (62%) and had to cut down on expenses in general and use savings [12].
Studies from countries such as Ireland, which has a broadly similar mixed public–private healthcare system as Australia, show that the majority of patients with CRC have no financial stress (59.1%) or financial strain (60.7%) during their treatment [20]. However, and consistent with the present study findings, 20% of patients relied on other sources of funds to cover any OOP costs [20]. This suggests there is still more work to be done to improve financial support for patients. In the Australian setting, one option to address this is through the various state cancer councils. Finally, Gordon et al. used a state-based cancer registry to identify patients with CRC in Australia, and consistent with our findings, they showed that most patients were financially comfortable (> 70%) and were not experiencing financial strain (> 85%) both at 6 and 12 months after diagnosis. Many patients used their savings to pay for any OOP expenses [21]. Overall, this reflects well on the Australian healthcare system, which mostly provides treatment in a timely and effective manner with minimal OOP costs and a taxpayer funded safety net (Medicare) for uninsured patients. However, it may also because Australia is a developed country, and many in the community have the financial means to cover OOP expenses. It is not possible to determine from the data in the present study whether patients who paid higher OOP costs than others had received either more timely or more effective treatment. The example of the single patient who self-funded their medical oncology treatment ($57,500) highlights the fact that the PBS in Australia shields many patients from potential large OOP costs when undergoing cancer treatment.
Certainly, those who had children and were young were more likely to express financial burden or stress than older patients or those without children. Hanley et al. also found that patients with dependents expressed a greater likelihood of financial strain, consistent with our findings [20]. This is likely explained by the financial burden usually associated with supporting a growing family. This was also consistent with a study by Veenstra et al., where younger patients had a higher financial burden for treating CRC than older patients [12]. Similarly, Huang et al. in China found that younger patients who were employed were more likely to have a higher financial burden than retirees [22]. This may be due to the unpaid time taken off from work for treatment or the financial impact of developing complications following treatment. Brink et al. assessed the employment status of patients with different cancer types in Denmark. They showed that patients were less likely to return to work 1 and 3 years after a cancer diagnosis in comparison to non-cancer patients [23]. In Australia, loss of income as a result of a diagnosis of cancer is not just personal but also has an indirect negative impact on the wider community, with an estimated reduction of $1.7 billion annually in the gross domestic product as a consequence of lost productivity [24].
The limitations of the present study include only providing a single time point, long-term cross-sectional representation of the financial burden and stress of patients who undergo liver resection for CRLM rather than making assessments at different time points. The cohort studied consisted of patients who had liver resection with curative intent for CRLM, and while most patients were cured, 20% of patients who completed the survey had recurrent disease and were undergoing treatment at the time of responding. While it was not possible to ask deceased patients or their family members about the financial stress and worry and whether the costs and treatment were worthwhile, this study of a blended cohort of patients who were apparently cured and those with recurrent disease provides some valuable insights. It is worth noting that the study analyses began from the diagnosis of liver metastases, which means that many patients had already undergone colorectal surgery prior to the starting point. This is likely a key reason why the OOP costs associated with colorectal surgery were lower than those for liver surgery in this analysis. Furthermore, liver resections can be more complex than the primary bowel surgery, and occasionally, patients require multiple resections, which may explain the discrepancy in OOP costs between these two types of surgery.
The mapping of each patient’s cancer journey to determine the OOP costs was performed retrospectively, and for the sake of simplicity, it was assumed that all specialists charged the AMA rates. Furthermore, an assumption was also made that imaging, blood tests, and general practitioner visits would not result in OOP and were fully funded by Medicare. Also, this study did not examine the fees of the assisting surgeon and anaesthetist, and ultimately, this may result in some underestimates and approximations in the OOP costs. Regardless, the study’s findings demonstrate manageable costs and limited patient financial burden and stress. Additionally, the study cohort was treated in a relatively affluent part of Australia where private health insurance rates are greater than the national rate (66% vs. 44.8%). Therefore, the financial toxicity from OOP costs, financial worry, and stress may not necessarily be representative of all socioeconomic groups in Australia. Future studies should examine how private insurance coverage levels affect financial burden and access to care in other Australian states and compare public and private care pathways. Furthermore, due to the cross-sectional nature with a small sample size, causal inferences with financial burden and stress could not be assessed, although an association of these factors was evaluated. The final limitation is that this study consisted of patients who underwent liver resection by a single surgeon, and the cohort was relatively small due to the number of deceased patients and non-responders. Despite this, by international standards, it is still a large sample, and the significance of the study is that this is the first in patients with CRLM to assess the OOP costs, financial burden, and stress in a cohort of patients who have undergone liver resection with long-term follow-up.
Conclusion
This study demonstrates a manageable amount of OOP costs in patients who undergo liver resection for CRLM. Most patients were not financially worried or stressed with the cost of their treatment. Understanding the costs and burden of disease can assist patients in better planning for the future and provide policymakers with areas to improve. As cancer care in Australia becomes more complex and expensive, this study may also be an important stimulus to begin discussions about the relative costs and value of specific treatments for different cancer types.
Supplementary Information
Below is the link to the electronic supplementary material. ESM 1(DOCX 17.4 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Australian Prudential Regulation Authority. Quarterly private health insurance membership and benefits summary - June 2024 2024.https://www.apra.gov.au/quarterly-private-health-insurance-membership-and-benefits-summary-june-2024. Accessed 12 Oct 2024
- 2Australian medical association (2022) Why medicare indexation matters 2022. https://www.ama.com.au/articles/why-medicare-indexation-matters. Accessed 14 Oct 2024
- 3Gordon LG, Beesley VL, Mihala G, Koczwara B, Lynch BM (2017) Reduced employment and financial hardship among middle-aged individuals with colorectal cancer. Eur J Cancer C 26(5):e 1274410.1111/ecc.1274428771857 · doi ↗ · pubmed ↗
- 4Brink E, Pilegaard MS, Bonnesen TG, Nielsen CV, Pedersen P (2024) Employment status in cancer patients the first five years after diagnosis-a register-based study. J Cancer Survivorship 8:1-310.1007/s 11764-024-01576-5PMC 1246045738587762 · doi ↗ · pubmed ↗