Clomiphene Citrate Medication for Infertility and Risk of Stillbirth or Neonatal Death: A Population-based Cohort Study
Vivienne Moore, Alice Rumbold, Renae Fernandez, Heather McElroy, Lynette Moore, Lynne Giles, Luke Grzeskowiak, Elizabeth Roughead, Michael Stark, Darryl Russell, Michael Davies

TL;DR
This study finds that using clomiphene citrate for infertility may be linked to a higher risk of stillbirth or neonatal death.
Contribution
The study provides new evidence on the potential increased risk of perinatal death associated with clomiphene citrate use.
Findings
Singleton pregnancies conceived with CC had higher rates of stillbirth and neonatal death.
The odds ratio for perinatal death was 1.54 for CC-exposed pregnancies.
Adjustments for biological and social risk factors did not change the results significantly.
Abstract
To assess associations between clomiphene citrate (CC) use and perinatal death. Whole of population data linkage cohort. South Australia. All women giving birth between July 2003 and December 2015 (n = 242,077). All births of at least 20 weeks were linked to government records of dispensed medications. A pregnancy was considered exposed to CC if a prescription was dispensed from 90 days before through to the end of a conception window. Descriptive statistics for stillbirths and neonatal deaths were stratified by multiplicity. For singletons, multivariable logistic regression models were used to examine the association of CC exposure with the combined outcome of perinatal death. Stillbirths and neonatal deaths (with 28 days of birth) combined as perinatal deaths. Among singletons, the prevalence of stillbirth was 6.6 per 1000 births, with neonatal deaths of 2.1 per 1000 live…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
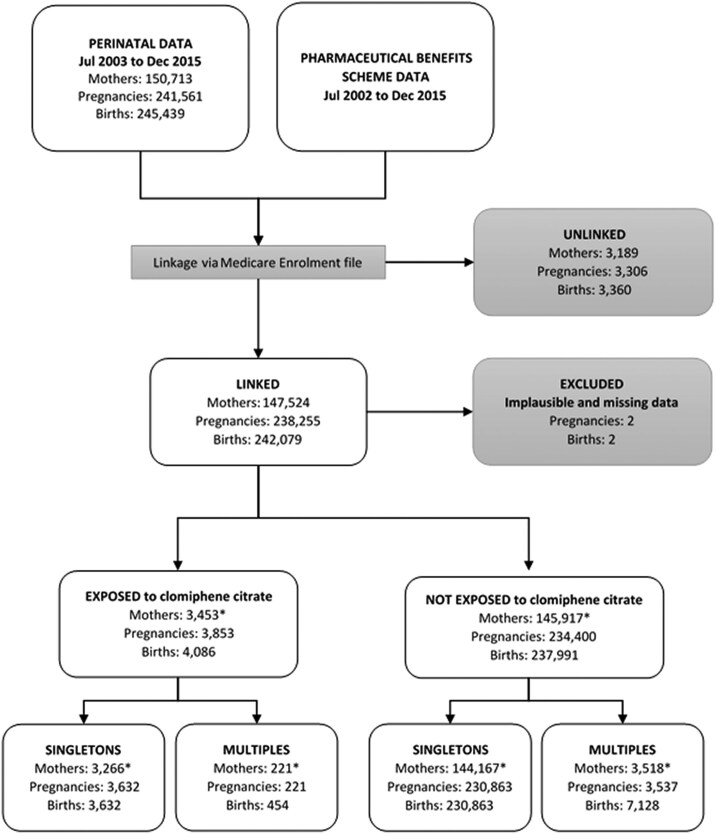 Figure 1
Figure 1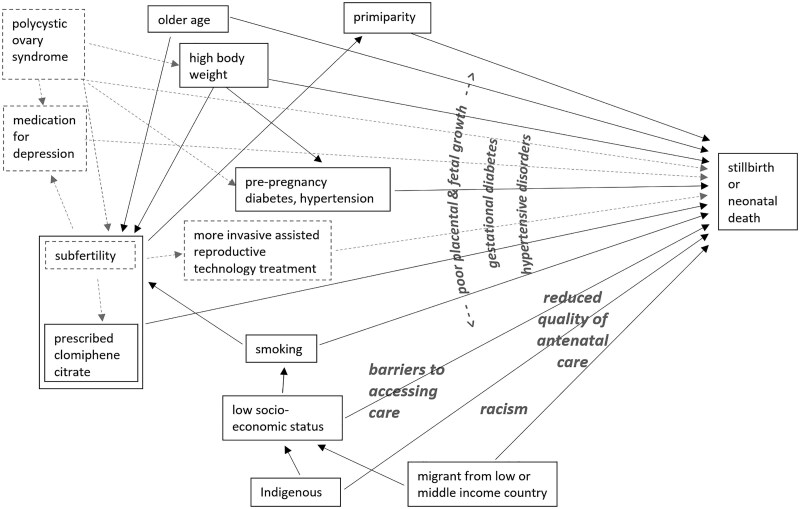 Figure 2
Figure 2| Characteristic | Singleton births (n = 234 495) | Multiple births (n = 7582) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Stillbirth | Neonatal death | Survived | Stillbirth | Neonatal death | Survived | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Age (years) | ||||||||||||
| < 25 | 347 | 22.5 | 118 | 24.5 | 44 370 | 19.1 | 12 | 10.2 | 9 | 11.7 | 861 | 11.7 |
| 25 to <30 | 403 | 26.2 | 127 | 26.4 | 66 671 | 28.7 | 36 | 30.5 | 21 | 27.3 | 1852 | 25.1 |
| 30 to <35 | 445 | 28.9 | 124 | 25.8 | 74 956 | 32.2 | 45 | 38.1 | 32 | 41.6 | 2593 | 35.1 |
| 35 to <40 | 263 | 17.1 | 92 | 19.1 | 38 199 | 16.4 | np | np | np | np | np | np |
| ≥ 40 | 83 | 5.4 | 20 | 4.2 | 8277 | 3.6 | np | np | np | np | np | np |
| Ethnicity | ||||||||||||
| Caucasian | 1225 | 79.5 | 377 | 78.4 | 195 382 | 84.1 | 102 | 86.4 | 70 | 90.9 | 6517 | 88.2 |
| Asian | 149 | 9.7 | 49 | 10.2 | 20 156 | 8.7 | np | np | np | np | np | np |
| Other | 167 | 10.8 | 55 | 11.4 | 16 935 | 7.3 | np | np | np | np | np | np |
| Region of birth | ||||||||||||
| Australia | 1220 | 79.2 | 386 | 80.2 | 186 821 | 80.4 | 105 | 89.0 | 70 | 90.9 | 6326 | 85.6 |
| Asia | 160 | 10.4 | 54 | 11.2 | 22 278 | 9.6 | np | np | np | np | np | np |
| Europe | 76 | 4.9 | 16 | 3.3 | 11 723 | 5.0 | np | np | np | np | np | np |
| Other | 85 | 5.5 | 25 | 5.2 | 11 651 | 5.0 | np | np | np | np | np | np |
| Low- to middle-income country of birth | 227 | 14.7 | 69 | 14.3 | 30 407 | 13.1 | 13 | 11.0 | 5 | 6.5 | 617 | 8.3 |
| Area index of relative socioeconomic disadvantage quintile | ||||||||||||
| 1 (most disadvantaged) | 463 | 30.1 | 134 | 27.9 | 60 173 | 25.9 | 28 | 23.7 | 20 | 26.0 | 1665 | 22.5 |
| 2 | 498 | 32.3 | 162 | 33.7 | 71 123 | 30.6 | 35 | 29.7 | 30 | 39.0 | 2252 | 30.5 |
| 3 | 139 | 9.0 | 54 | 11.2 | 25 265 | 10.9 | 6 | 5.1 | 6 | 7.8 | 817 | 11.1 |
| 4 | 256 | 16.6 | 86 | 17.9 | 49 304 | 21.2 | 34 | 28.8 | 14 | 18.2 | 1714 | 23.2 |
| 5 (least disadvantaged) | 185 | 12.0 | 45 | 9.4 | 26 608 | 11.5 | 15 | 12.7 | 7 | 9.1 | 939 | 12.7 |
| Tobacco smoker at first antenatal visit | ||||||||||||
| Yes | 338 | 21.9 | 127 | 26.4 | 42 616 | 18.3 | 16 | 13.6 | 6 | 7.8 | 1210 | 16.4 |
| No | 1100 | 71.4 | 334 | 69.4 | 187 189 | 80.5 | 98 | 83.1 | 64 | 83.1 | 5900 | 79.9 |
| Unknown | 103 | 6.7 | 20 | 4.2 | 2668 | 1.2 | 4 | 3.4 | 7 | 9.1 | 277 | 3.8 |
| Body mass index (kg/m2) | ||||||||||||
| Underweight and healthy weight (<25) | 395 | 25.6 | 102 | 21.2 | 65 034 | 28.0 | 28 | 23.7 | 11 | 14.3 | 1574 | 21.3 |
| Overweight (25 to <30) | 232 | 15.1 | 77 | 16.0 | 36 979 | 15.9 | 22 | 18.6 | 10 | 13.0 | 1005 | 13.6 |
| Obese (≥30) | 223 | 14.5 | 65 | 13.5 | 32 552 | 14.0 | 12 | 10.2 | 15 | 19.5 | 1080 | 14.6 |
| Unknown | 691 | 44.8 | 237 | 49.3 | 97 908 | 42.1 | 56 | 47.5 | 41 | 53.3 | 3728 | 50.5 |
| Metabolic health | ||||||||||||
| Prepregnancy diabetes | 39 | 2.5 | 9 | 1.9 | 1544 | 0.7 | — | np | np | np | np | np |
| Prepregnancy hypertension | 29 | 1.9 | 11 | 2.3 | 2677 | 1.2 | np | np | np | np | np | np |
| Obstetric history and pregnancy complications | ||||||||||||
| No previous pregnancy | 696 | 45.2 | 210 | 43.7 | 97 505 | 41.9 | 44 | 37.3 | 39 | 50.7 | 3096 | 41.9 |
| Previous miscarriage | 400 | 26.0 | 136 | 28.3 | 54 704 | 23.5 | 31 | 26.3 | 16 | 20.8 | 1920 | 26.0 |
| Previous neonatal death | 17 | 1.1 | 14 | 2.9 | 1015 | 0.4 | Np | np | np | np | np | np |
| Gestational diabetes | 45 | 2.9 | 23 | 4.8 | 14 559 | 6.3 | 5 | 4.2 | 5 | 6.5 | 704 | 9.5 |
| Hypertension during pregnancy | 88 | 5.7 | 33 | 6.9 | 17 922 | 7.7 | Np | np | np | np | np | np |
| Gestation at birth (weeks) | ||||||||||||
| Under 32 | 1088 | 70.6 | 294 | 61.1 | 1969 | 0.9 | 86 | 72.9 | 68 | 88.3 | 759 | 10.3 |
| 32 to 36 | 184 | 11.9 | 67 | 13.9 | 13 390 | 5.8 | 18 | 15.3 | 6 | 7.8 | 3783 | 51.2 |
| 37 to 40 | 237 | 15.4 | 103 | 21.4 | 190 189 | 81.8 | np | np | np | np | np | np |
| ≥ 41 | 32 | 2.1 | 17 | 3.5 | 26 925 | 11.6 | np | np | np | np | np | np |
| Male baby | 800 | 51.9 | 265 | 55.1 | 119 538 | 51.4 | 56 | 47.5 | 41 | 53.3 | 3669 | 49.7 |
| Characteristic | Exposed to CC | Not exposed to CC | ||
|---|---|---|---|---|
| n | % | n | % | |
| Age (years) | ||||
| Under 25 | 277 | 7.6 | 44 558 | 19.3 |
| 25 to <30 | 1182 | 32.5 | 66 019 | 28.6 |
| 30 to <35 | 1426 | 39.2 | 74 099 | 32.1 |
| 35 to <40 | 624 | 17.2 | 37 930 | 16.4 |
| ≥ 40 | 123 | 3.4 | 8257 | 3.6 |
| Ethnicity | ||||
| Caucasian | 3285 | 90.4 | 193 699 | 83.9 |
| Asian | 228 | 6.3 | 20 126 | 8.7 |
| Other | 119 | 3.2 | 17 038 | 7.4 |
| Region of birth | ||||
| Australia | 3101 | 85.4 | 185 326 | 80.3 |
| Asia | 256 | 7.0 | 22 236 | 9.6 |
| Europe | 166 | 4.6 | 11 649 | 5.0 |
| Other | 109 | 3.0 | 11 652 | 5.0 |
| Low- to middle-income country of birth | 340 | 9.4 | 30 363 | 13.2 |
| Area index of relative socioeconomic disadvantage quintile | ||||
| 1 (most disadvantage) | 717 | 19.7 | 60 053 | 26.0 |
| 2 | 1090 | 30.0 | 70 693 | 30.6 |
| 3 | 397 | 10.9 | 25 061 | 10.9 |
| 4 | 892 | 24.6 | 48 754 | 21.1 |
| 5 (least disadvantage) | 536 | 14.8 | 26 302 | 11.4 |
| Tobacco smoker at first antenatal visit | ||||
| Yes | 274 | 7.5 | 42 807 | 18.5 |
| No | 3301 | 90.9 | 185 322 | 80.3 |
| Unknown | 57 | 1.6 | 2734 | 1.2 |
| Body mass index (kg/m2) | ||||
| Underweight and healthy weight (<25) | 815 | 22.4 | 64 716 | 28.0 |
| Overweight (25-<30) | 505 | 13.9 | 36 783 | 15.9 |
| Obese (≥30) | 597 | 16.4 | 32 243 | 14.0 |
| Unknown | 1715 | 47.2 | 97 121 | 42.1 |
| Metabolic health | ||||
| Pre-existing diabetes | 57 | 1.6 | 1535 | 0.7 |
| Pre-existing hypertension | 59 | 1.6 | 2658 | 1.2 |
| Obstetric history and pregnancy complications | ||||
| No previous pregnancy resulting in birth | 2092 | 57.6 | 96 319 | 30.0 |
| Previous miscarriage | 991 | 27.3 | 54 249 | 23.5 |
| Previous neonatal death | 23 | 0.6 | 1023 | 0.4 |
| Gestational diabetes | 413 | 11.4 | 14 214 | 6.2 |
| Hypertension during pregnancy | 383 | 10.5 | 17 660 | 7.6 |
| Gestation at birth (weeks) | ||||
| Under 32 | 75 | 2.1 | 3276 | 1.4 |
| 32 to 36 | 241 | 6.6 | 13 400 | 5.8 |
| 37 to 40 | 3030 | 83.4 | 187 499 | 81.2 |
| ≥ 41 | 286 | 7.9 | 26 688 | 11.6 |
| Male baby | 1836 | 50.6 | 118 767 | 51.4 |
| Perinatal outcome | ||||
| Survived neonatal period (28 days) | 3584 | 98.7 | 228 889 | 99.1 |
|
| 1504 |
| ||
| Stillborn | 37 | 10.2 | 1504 | 6.5 |
| Neonatal death | 11 | 3.1 | 470 | 2.1 |
| Model using generalized estimating equations and multiple imputation | Adjusted OR | 95% CI |
|---|---|---|
| Model 1: adjusted for maternal age, primiparity, smoking, body mass index, pre-existing diabetes, pre-existing hypertension | 1.56 | 1.15-2.07 |
| Model 2: Model 1 covariates and whether or not mother was Caucasian, Indigenous, migrant from low- or middle-income country as well as residential disadvantage quintile | 1.59 | 1.18-2.13 |
| Model 3: Model 2 covariates and variables that may be on the causal pathway—sex of baby, gestational diabetes, hypertension in pregnancy | 1.64 | 1.22-2.21 |
- —National Health and Medical Research Council of Australia10.13039/501100000925
- —Channel 7 Children’s Research Foundation10.13039/501100001075
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAssisted Reproductive Technology and Twin Pregnancy · Pregnancy and Medication Impact · Pregnancy and preeclampsia studies
Stillbirths and neonatal deaths are a source of grief and distress for parents and can have enduring consequences for the health and well-being of families (1-3). Many of these deaths have antecedents of compromised fetal growth and poor placental function, but identifying and managing these high-risk pregnancies remains challenging (4, 5). Understanding other risk factors could improve risk prediction (6) and could provide earlier prevention opportunities, including before pregnancy (7, 8).
Treatment for infertility using procedures involving in vitro fertilization may be associated with increased risks of stillbirth and neonatal death (7, 9, 10). Interpretation of this finding is complex as factors related to infertility disorders per se may contribute to poor perinatal outcomes (11). Treatment for infertility can also consist of medication alone. These births lack visibility because they are incompletely captured or not recorded at all in registries of births arising from assisted reproductive technology (ART) (12). In Australia, for example, reporting is not required when medical treatment for infertility occurs outside of specialist ART clinics. However, such treatment accounts for a quarter of births conceived with all forms of medical assistance (13).
Globally, the medication most commonly used for infertility treatment outside of a specialist ART clinic is clomiphene citrate (CC). For example, in the US Nurses’ Health Study II, around 80% of women who reported infertility in the period 2000-2011 had used CC, usually as the first (and often the only) treatment (14). In Australia, CC is the only oral medication licensed for use for anovulatory infertility. Until 2023, it was a recommended first-line treatment for polycystic ovary syndrome (PCOS), now second line (15, 16).
CC is a selective estrogen receptor modulator (17). The most obvious and well-documented adverse outcome of CC use is multiple pregnancy; this can be minimized by following the recommendation for ultrasound in at least the first cycle of treatment to determine the number of dominant follicles (eg, 18). Beyond that, questions about the safety of CC for the fetus are unresolved (19), with little research on possible adverse perinatal outcomes of CC, such as perinatal death.
Infertility treatment continues to change as evidence accumulates. For instance, CC is no longer recommended as an isolated treatment for unexplained infertility (20, 21). However, clinicians in the UK have reported that they continue to prescribe CC under pressure from couples preferring treatment to expectant management (22). Practice elsewhere is largely unknown. This highlights a need to investigate the possible adverse outcomes associated with this treatment so that potential harms are appreciated as well as benefits.
Here we investigate outcomes of pregnancies following CC by linking records of dispensed medications to a perinatal registry. The aim of this study was to quantify the fetal and neonatal death rates for births conceived in proximity to CC dispensing. For singletons, a further aim was to compare the combined perinatal death rate with that for the wider population, taking into account potential confounding factors.
Materials and Methods
A population-based cohort study was undertaken based on births in the state of South Australia from July 2003 to December 2015. All births of at least 20 weeks’ gestation (or 400 g) must be reported to the state government, which maintains the Perinatal Registry. Almost all births in the state occur in a hospital, and reporting to the registry is standardized.
The Australian Institute of Health and Welfare undertook data linkage between South Australian Perinatal Registry records and Australian Government records of dispensed medications. Details have been described elsewhere (13).
Briefly, the Australian Government keeps electronic records of dispensing because it subsidises the costs of approved medications. For CC, these records were complete from July 2002 apart from two 6-month periods (January to June 2009 and January to June 2012) when the cost of some brands of CC fell below the amount attracting a subsidy. Data linkage was based on identifiers of women and babies, with 2 rounds of linkage undertaken. Linkage to dispensing records was achieved for 97.9% of women (and 98.6% of pregnancies). Unlinked women and their pregnancies were excluded from the present analysis. See Fig. 1 for the flow diagram for these processes and the available data.
*Flow diagram for data linkage. Mothers may have more than 1 pregnancy between 2003 and 2015 and therefore numbers may sum to more than the total in the row above. Mothers may be counted in more than 1 group; for example, 1 pregnancy may have been exposed and another not exposed, or 1 pregnancy may have resulted in a singleton birth and another a multiple birth.
Outcome
The outcomes were stillbirth after 20 weeks’ gestation and neonatal death (within 28 days), as well as the combined outcome of perinatal death. Additionally, whether the pregnancy was singleton or multiple was considered. The main focus of this analysis was singleton pregnancies; we did not consider it appropriate to combine singleton and multiple pregnancies.
Exposure
Conception was designated as occurring proximal to CC (exposed) if a prescription for CC was dispensed from 90 days before through to the end of a preconception window (defined later). The standard quantity of medication supplied to women is 10 tablets—enough medication for 2 cycles, assuming the dose is 50 mg. We ascertained whether women were also supplied with gonadotropins in the exposure period (occasionally prescribed with CC to trigger final follicular maturation and ovulation).
It was necessary to derive a preconception window for each birth because over 20% were missing the date of last menstrual period (LMP), and births to women with anovulatory infertility may be overrepresented in this group (13). This window was based on the recorded date of birth and gestational age, with allowance for biological variation and inaccuracy of dating by routine ultrasound (13). Comparisons between available LMP dates and the derived preconception window are detailed elsewhere; where the LMP date was not missing, it was consistent with the preconception window in most cases (94.5%) (13). One missing gestational age was imputed as the 50th centile for the relevant birthweight and sex using Australian data (23).
Covariates
Covariate selection was based on our current understanding of casual pathways, as depicted in Fig. 2. Variables in boxes with a solid outline represent factors available for investigation while those in dashed boxes are theoretically relevant but not available. Variables not in boxes represent mediators. While previous adverse pregnancy outcomes are used to predict stillbirth and neonatal death for clinical purposes, these are not included in the diagram as they are considered to be outcomes of the underlying factors responsible for increased risk, not independent risk factors.
Schema illustrating our understanding of the causal structure of associations between clomiphene citrate, confounding variables, and the outcomes of stillbirth or neonatal death among singletons.
Maternal characteristics were obtained from the Perinatal Registry records. These included age, country/region of birth, ethnicity, pregnancy history, body mass index (BMI; collected from 2007), smoking, pre-existing hypertension, and diabetes (type 1 and type 2, not distinguished). Most of these variables were used in the format provided. However, age of each woman at the time of birth was categorized; region of birth was classified as Australia, Europe, Asia, or “other” for descriptive purposes; and in country of birth was classified as low or middle income (LMI) or high income (24). Postcode of residence was used to assign a socioeconomic Index of Relative Social Disadvantage (25), categorized in quintiles using the Australian distribution as the reference.
Certain medical conditions are known to contribute to stillbirth (26), but most of these do not entail need for CC. The exceptions are type 2 diabetes and hypertension, which are elevated in women with PCOS.
Direct contributions of PCOS to stillbirth or neonatal death are represented by a dashed line. For example, endometrial dysfunction that occurs in PCOS can affect fetal survival (27). Genetic factors that contribute to PCOS could also be responsible for compromised placental and fetal development, although this has not been established (28, 29). Other types of infertility with a genetic basis are known to affect fetal viability and survival (30-32), but in the Australian context it is unlikely that CC would be prescribed to women with conditions such as recurrent pregnancy loss or primary ovarian insufficiency.
There is some evidence of a small increase in the risk of death among male babies, especially in relation to maternal type 2 diabetes (33). Since CC does not appear to affect the ratio of male to female babies, conceptually this factor is a mediator rather than a confounder. Eight babies who died had indeterminate sex and were considered male for the purposes of this analysis.
Statistical Analysis
We calculated the prevalence of stillbirths and neonatal deaths and tabulated data to compare characteristics of pregnancies by outcome and plurality. Some summary statistics could not be reported due to sparse data and to ensure individuals could not be reidentified.
In multivariate models for singletons, we combined the outcomes of stillbirth and neonatal death, although we acknowledge it is preferable to analyze these separately if data permits. We used logistic regression models to estimate the odds ratio (OR) for the association of exposure to CC and perinatal death, the preferred effect measure in analytic epidemiological studies (34). To account for the correlation between births to the same mother a generalized estimating equation approach with an exchangeable correlation structure was used.
A series of logistic regression models were then fit, in which different sets of adjustment covariates were sequentially added. Model 1 was based on variables in the minimal sufficient adjustment set that referenced physiological pathways (maternal age, primiparity, smoking in pregnancy, BMI, pre-existing diabetes, and pre-existing hypertension). In model 2, which represents the complete minimal adjustment set, further variables were added reflecting influences of disadvantage or discrimination (area disadvantage, Indigenous, born in LMI country). In model 3, presented for clinical interest, variables that are arguably mediators were added: the sex of the fetus as well as gestational diabetes and hypertension in pregnancy.
Missing data were generally rare, apart from mother's smoking status (n = 2791; 1.2%) and BMI (n = 98 836; 42.1%). Maternal BMI was only collected from 2007 and has gradually become more complete (51.2% missing in 2007 reducing to 8.8% in 2015).
We imputed missing values for BMI category and smoking status using multiple imputation by chained equations (35), performed in the order stated previously with fully conditional specification of the logistic regression method (cumulative logit for BMI) and 100 burn-ins before each imputation. In addition to all variables used in modeling, we included auxiliary variables of Caucasian (yes/no) and Asian (yes/no), as these were relevant to the missing at random assumption. We generated 30 imputed datasets and combined the estimates using Rubin's rules. We also generated results using the complete cases as well as using a missing indicator approach, and we explored why these are biased.
SAS version 9.4 was used in all analyses. The procedures MI and MIANALYZE were used for the multiple imputation analyses.
Ethics Approval
Approval for the study was obtained from the ethics committees of the South Australian Department of Health [HREC/15/SAH/80] and the Australian Institute of Health and Welfare [EO2013/3/51]. Individual level consent was not required because the study entailed the use of deidentified records (managed through the Secure Unified Research Environment (SURE) facility).
Results
There were 242 077 births of at least 20 weeks’ gestation to 147 524 women in the study period. Among singletons (96.9% of births), the prevalence of stillbirth was 6.6 per 1,000, with neonatal deaths of 2.1 per 1000 live births. Corresponding prevalences for multiples were 15.6 and 10.3 per 1000.
Maternal and pregnancy characteristics are compared in Table 1. As expected, among singletons there was an excess of stillbirths where mothers were aged 40 years or more, had not previously had an ongoing pregnancy, or were smoking at the time of the first antenatal visit. Stillbirths were also elevated where mothers were disadvantaged, or migrants from a LMI country. Similar patterns were observed for neonatal deaths. Pre-existing diabetes and hypertension in mothers were clearly associated with increased occurrence of stillbirth and neonatal death. The majority of singleton stillbirths (83%) and neonatal deaths (75%) occurred before 37 weeks of gestation.
In all, there were 3853 pregnancies exposed to CC (1.6%), with 94.3% of these pregnancies being singletons. In 5.7% of the CC pregnancies, gonadotropin was also prescribed, but this did not contribute to the excess of multiples.
Singleton births that occurred after exposure to CC (Table 2) tended to involve Caucasian women and mothers over 30 years of age, with the most disadvantaged women underrepresented. The proportion of births that occurred before 37 weeks’ gestation was higher among those exposed to CC (8.7%) than in the unexposed group (7.2%).
Frequencies of stillbirth and neonatal death were elevated after exposure to CC (Table 2). The prevalence of stillbirth was 10.2 per 1000 births, while neonatal death occurred in 3.1 per 1000 live births.
The crude OR for the association between CC exposure and stillbirth was 1.57 [95% confidence interval (CI) 1.13, 2.18] for singleton births. The crude OR for CC exposure and neonatal death was 1.49 (95% CI 0.82, 2.71) for singleton live births.
The crude OR for CC exposure and the pooled outcome of perinatal death was 1.54 (95% CI 1.15, 2.07). This result was stable in model 1, in which adjustment was made for covariates contributing to perinatal death through biological pathways, and in model 2, in which social determinants were added, as shown in Table 3. For clinical interest, in model 3 variables that are arguably on the causal pathway were added: fetal sex, gestational diabetes, and hypertension in pregnancy. The magnitude of the OR increased in this last scenario.
We note that if we had restricted our analysis to complete cases, we would have observed somewhat stronger associations (OR = 1.85, 95% CI 1.25, 2.74) for the equivalent of model 2. Investigation of this indicated that it was driven by a relatively high occurrence of perinatal death in pregnancies of women whose smoking status or BMI was unknown (and who were unexposed). Using a missing indicator approach yielded results that were closer to multiple imputation (OR = 1.57, 95% CI 1.16, 2.11 for the equivalent of model 2).
Discussion
In our population-based cohort study, there was a 50% increase in the risk of singleton stillbirth or neonatal death among women who were dispensed CC around the time of conception. This was stable in models that accounted for established confounding variables. The frequency of multiple pregnancy (mostly twins) among those dispensed CC was consistent with consumption of medication. However, multiples were not included in our main analyses because their risk of adverse perinatal outcomes is substantially greater for different reasons.
To our knowledge, there are few well-designed studies assessing a possible link between CC (without other fertility treatment procedures, such as intrauterine insemination) and stillbirth or neonatal death. There are several reasons for this knowledge gap: early cohort studies were too small for differences in these outcomes to be detected (see 36); until recently, the focus of trials was on achieving clinical pregnancy, so most trials did not continue to birth (37); and in registry-based studies, information on medications used in isolation to treat infertility is rarely available (11, 38).
Fertility medications were considered in a case-control study (>300 cases) of stillbirths and deaths within 24 hours of birth, undertaken by Pastore et al (39). Among case mothers, 4.8% had taken fertility medication around the time of conception, with an adjusted OR for stillbirth of 1.9 (95% CI 0.8, 4.5). Of 26 women reporting the use of fertility medications, 20 provided the name, which for 14 was a brand of CC.
Established confounding factors included in our analyses were associated with risks of perinatal death in line with published findings (7). There is some uncertainty around the role of gestational diabetes and hypertension, each of which potentially confers a 30% to 40% increase in risk of stillbirth but may not do so when proactively identified and treated (40, 41). In our study, the apparently protective effect of these conditions probably reflects good access to high-quality antenatal care.
It is possible that CC has a direct effect on the risk of stillbirth and neonatal death. CC is a selective estrogen receptor modulator with both agonist and antagonist effects in different contexts. Concerns about safety for the fetus are longstanding, partly due to the long persistence of CC and its metabolites in the body and the potential for bioaccumulation over successive cycles (19, 42). Overlapping potency in the cytotoxic and estrogen receptor antagonist activities of CC has been reported (43). CC exposure can cause epigenetic changes (44) and DNA strand breaks (45, 46). CC is reported to cause reduced endometrial thickening (47) and has known off-target effects (44, 48, 49) that could affect placental and fetal development. Recent work has demonstrated biological plausibility of adverse pregnancy outcomes with observed dose-response relationships of clomiphene and developmental anomalies and fetal death in a mouse model (50).
It has been suggested that parental infertility contributes to adverse perinatal outcomes in offspring conceived with medical assistance. Genetic factors that underlie some types of infertility are related to fetal survival and perinatal outcomes (30, 51), as are conditions such as type 1 and type 2 diabetes (52). Research aiming to disentangle “patient” from “treatment” factors has been occurring in relation to ART (11, 53), although, to date, most investigations do not consider perinatal death.
Research examining parental and treatment influences on other perinatal outcomes after ART suggests that findings pointing to infertility per se as a risk factor may be inflated by a lack of data on parents’ wider health profiles. For example, Messerlian et al (54) showed that most types of infertility did not have a direct effect on risk of preterm birth after established maternal risk factors were taken into account, the exceptions being when infertility reflected uterine abnormalities (eg, fibroids), endometriosis, or tubal blockages. However, results of Duneitz et al (55) suggested preterm birth in singletons was increased with all underlying infertility diagnoses in parents as well as with each step in ART treatment. Of note, these studies differed in available data, with Duneitz et al (55) lacking maternal smoking and BMI. Health profiles of parents are thus relevant in both studies, including aspects that contribute to infertility, but the residual contribution of infertility per se may be small after other aspects of parental health are well characterized.
In our study, we had substantial information on maternal factors, including maternal smoking and BMI. It is unlikely that women taking CC had infertility due to uterine abnormalities, endometriosis, or tubal blockages. Most likely, women had PCOS or the infertility was unexplained; the residual risk conveyed by these conditions remains unclear. A recent study found that the risk of stillbirth in women with PCOS was increased by 50% (OR = 1.50, 95% CI 1.28, 1.77), but treatment for infertility was not explored as a contributing factor (56).
There are several factors that we did not take into account that might represent confounding variables, with evidence in relation to stillbirth emerging. Arguably, these would have a minor influence on results. For example, alcohol and cannabis may contribute to stillbirth (7, 57, 58), but women desiring pregnancy and requiring fertility treatment are highly likely to abstain from use (eg, 59). Most medications for which risks to the fetus are known, or suspected, are not likely to be differentially used by women who need CC. An exception is medication for depression, which may be relatively more common among women with PCOS (60) and those experiencing infertility (61), although the association with stillbirth is uncertain (62).
The possibility has been raised that elevated risk of adverse perinatal outcomes, in general, in children conceived with various forms of medical assistance reflects greater reluctance on the part of their parents to terminate for congenital anomalies (63). However, this does not seem to be the case in practice (64).
Turning to the implications of our findings, it has been suggested that overdiagnosis and overtreatment of infertility could be reduced if couples desiring pregnancy were encouraged to attempt to conceive naturally for at least 2 years, appropriate in many circumstances (65). For women with PCOS, lifestyle intervention, particularly directed toward reducing body weight, might improve the chance of natural conception, but greater effort is needed to generate the evidence base and practical supports for women (66, 67). Letrazole is now recommended as the first-line treatment for women with PCOS, replacing CC (16). When CC is contemplated, consideration of possible risks as well as benefits should be part of informed decision-making. Pregnancies achieved with CC, like those in women with PCOS more broadly (16), should be considered high risk with women supported and monitored.
Strengths and Limitations
A strength of our study is the high-quality data in terms of population coverage, reporting consistency, and the high proportion of linked records. Data on terminations is of high quality in South Australia, so it is unlikely that terminations have been misclassified as stillbirths. Established risk factors for stillbirth that might inflate the association between CC exposure and perinatal death were taken into account.
We cannot be certain that the dispensed CC medication was consumed, but motivation to take this medication is high and the simple regimen was shown to facilitate adherence in a clinical trial (68). The frequency of multiple pregnancy in the group dispensed CC was consistent with widespread consumption. Any misclassification from assuming medication was consumed when that was not the case would bias results toward the null.
There were 2 periods of 6 months’ duration in the 13 years of exposure data when dispensing was underascertained. Thus there may be additional CC pregnancies, but any misclassification would lead to underestimation of the association between CC and perinatal death. Information on other forms of ART treatment was lacking, but this represents a conservative bias, since women who became pregnant by this means (with an increased risk of perinatal death) were included in the group unexposed to CC; such women would constitute only a small fraction of that group (around 4%) (69).
Conclusion
One in every 60 births in South Australia was conceived proximal to CC dispensing during the study period. The risk of perinatal death was 50% higher in these births than in the wider population, after taking into account established risk factors for this adverse outcome, including maternal smoking and high BMI. The effect of CC on perinatal death seems unlikely to be wholly explained by parental infertility. Most medical treatments have potential harms as well as benefits, and greater appreciation of this could be used to extend the time frame in which couples attempt to conceive naturally, where appropriate.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frøen JF, Gordijn SJ, Abdel-Aleem H, et al Making stillbirths count, making numbers talk—issues in data collection for stillbirths. BMC Pregnancy Childbirth. 2009;9:58.20017922 10.1186/1471-2393-9-58PMC 2805601 · doi ↗ · pubmed ↗
- 2Jones K, Robb M, Murphy S, Davies A. New understandings of fathers’ experiences of grief and loss following stillbirth and neonatal death: a scoping review. Midwifery. 2019;79:102531.31493675 10.1016/j.midw.2019.102531 · doi ↗ · pubmed ↗
- 3Obst KL, Due C, Oxlad M, Middleton P. Men's grief following pregnancy loss and neonatal loss: a systematic review and emerging theoretical model. BMC Pregnancy Childbirth. 2020;20(1):11.31918681 10.1186/s 12884-019-2677-9PMC 6953275 · doi ↗ · pubmed ↗
- 4Kingdom JC, Smith GC. Next steps to prevent stillbirth associated with growth restriction. BJOG. 2020;127(9):1081.32237039 10.1111/1471-0528.16237 · doi ↗ · pubmed ↗
- 5Iliodromiti S, Smith GCS, Lawlor DA, Pell JP, Nelson SM. UK stillbirth trends in over 11 million births provide no evidence to support effectiveness of Growth Assessment Protocol program. Ultrasound Obstet Gynecol. 2020;55(5):599‐604.32266750 10.1002/uog.21999 · doi ↗ · pubmed ↗
- 6Townsend R, Manji A, Allotey J, et al Can risk prediction models help us individualise stillbirth prevention? A systematic review and critical appraisal of published risk models. BJOG. 2021;128(2):214‐224.32894620 10.1111/1471-0528.16487 · doi ↗ · pubmed ↗
- 7Flenady V, Koopmans L, Middleton P, et al Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet. 2011;377(9774):1331‐1340.21496916 10.1016/S 0140-6736(10)62233-7 · doi ↗ · pubmed ↗
- 8Flenady V, Wojcieszek AM, Middleton P, et al Stillbirths: recall to action in high-income countries. Lancet. 2016;387(10019):691‐702.26794070 10.1016/S 0140-6736(15)01020-X · doi ↗ · pubmed ↗