Microneedling for Anterior Neck Surgical Scars: A Systematic Review of Effectiveness and Evidence Gaps
Hassan Baig, Qaisar I Khan, Abdulaziz Al Failakawi, Mujahid Khan, James Lucocq

TL;DR
This paper reviews the effectiveness of microneedling for neck surgical scars, finding no direct studies but suggesting potential benefits based on evidence from other body regions.
Contribution
The paper identifies a lack of direct evidence for microneedling on anterior neck scars and proposes potential treatment parameters based on indirect evidence.
Findings
No eligible studies specifically examined microneedling for anterior neck surgical scars.
Indirect evidence from other body regions suggests microneedling may improve scar outcomes.
Three to six microneedling sessions at 1.0-1.5 mm depth are proposed for optimal results.
Abstract
Neck surgeries often leave anterior neck scars, causing cosmetic and psychological issues. These scars are more exposed to mechanical stress and the environment, potentially leading to hypertrophy, dyschromia, and scar widening. Traditionally, surgical scar interventions have been postponed until full scar maturation, usually between six and 12 months after surgery, but recent evidence indicates that early microneedling may improve collagen remodelling and scar quality. While microneedling has been studied for facial and abdominal scars, its effectiveness on anterior neck scars remains unclear. A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Searches were performed in several databases and registers. Eligible studies included randomised controlled trials (RCTs), cohort studies, and observational…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
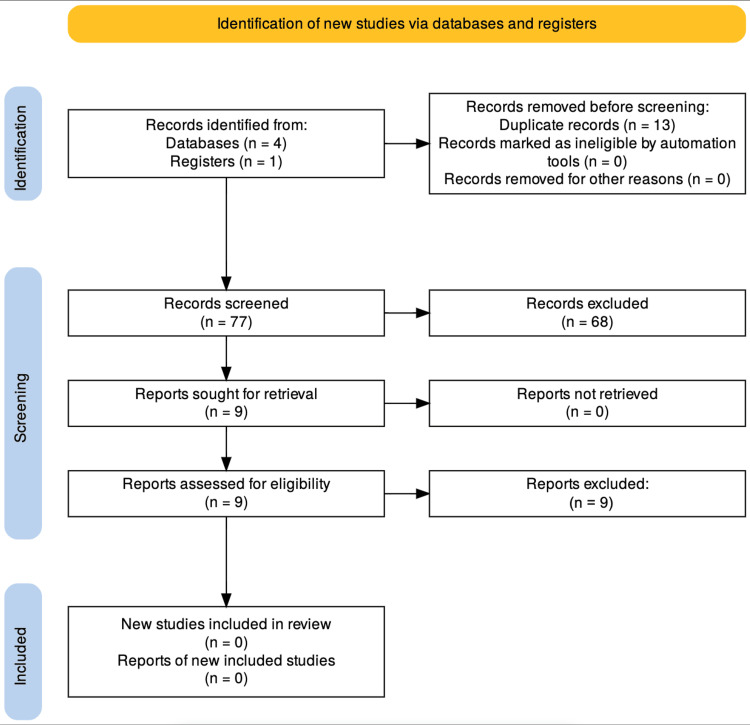 Figure 1
Figure 1| Inclusion | Exclusion | |
| Patient | Adults > 16 years old, anterior neck surgical scars | Anyone < 16 years old, surgical scars other than the anterior neck |
| Intervention | Studies focusing on microneedling for anterior neck surgical scars | Studies evaluating microneedling in combination with other interventions, such as laser therapy or PRP. Any other treatment modalities |
| Control | Placebo or no other intervention | Studies evaluating microneedling in combination with other interventions, such as laser therapy or PRP. Any other treatment modalities |
| Outcome | Studies employing objective scar assessment tools, like the Patient and Observer Scar Assessment Scale (POSAS), Vancouver Scar Scale (VSS), or Global Aesthetic Improvement Scale (GAIS) | Studies not employing objective scar assessment |
| Study | Studies published in English within the past 25 years involving human subjects were eligible. Studies focussing on anterior neck surgical scars | Studies published in languages other than English, not involving human subjects. Studies focussing on areas other than anterior neck surgical scars. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Sympathectomy and Hyperhidrosis Treatments · Laser Applications in Dentistry and Medicine
Introduction and background
Neck surgeries, such as thyroidectomies and parathyroidectomies, are frequently performed to treat both benign and malignant conditions, with post-operative scarring being an inevitable consequence [1,2]. The anterior neck is a visible and dynamic region, making surgical scars cosmetically and functionally significant. Despite advancements in surgical techniques, post-operative scarring remains a concern due to its visibility, exposure to environmental factors, and continuous movement.
Surgeons often attempt to place incisions within natural skin folds to minimise the visibility of scars; however, well-placed scars can still be noticeable, particularly in individuals with lighter or darker skin tones, where pigment changes are more evident [3]. Additionally, the thin skin of the anterior neck has lower collagen density and fewer sebaceous glands, making it prone to textural irregularities and prolonged erythema [4,5].
Unlike scars in less exposed anatomical areas, anterior neck scars are subjected to mechanical forces from daily head and neck movements, leading to scar widening, hypertrophy, and dyschromia [6,7]. These factors heighten patient dissatisfaction, particularly following elective surgeries, where cosmetic expectations are high [8,9].
Current advancements in neck surgeries emphasise scarless techniques, such as transoral or transaxillary approaches. However, these methods are not yet universally implemented due to practical constraints, reduced surgical efficiency, and economic considerations. Consequently, in situations where scarless surgery is not feasible, reducing the visibility and improving the quality of scars becomes essential to achieving optimal aesthetic outcomes and patient satisfaction.
Traditionally, scar management has been postponed for six to 12 months post-operatively to allow for complete scar maturation due to concerns that early interventions may disrupt healing. However, emerging evidence indicates that early interventions, such as microneedling, may enhance collagen remodelling and improve scar quality [10,11].
Microneedling, or percutaneous collagen induction therapy, is a minimally invasive technique, yielding promising results in enhancing scars by stimulating collagen and elastin production through controlled micro-injuries [12,13]. Studies on facial, chest, and abdominal surgical scars have demonstrated significant reductions in scar thickness, improved pigmentation, and enhanced texture, fostering optimism regarding their potential application in managing anterior neck scars [14,15]. Despite these encouraging findings, its role in addressing anterior neck scars specifically remains under-explored.
Given the cosmetic significance of anterior neck scars and the increasing interest in non-invasive techniques for scar enhancement, further research is crucial to determine optimal microneedling parameters, such as the timing of initiation, session frequency, duration, and needle depth [16]. This research will be pivotal for refining clinical practice and optimising post-operative scar management for patients undergoing neck surgery.
This systematic review aims primarily to provide a clear and focused evaluation of the effectiveness of microneedling for anterior neck surgical scars, in addition to assessing the optimal timing for initiating microneedling after surgery, comparing early intervention with traditional delayed treatment. Secondary outcomes include evaluating various treatment parameters, such as session frequency, duration, and needle depth, based on existing evidence from other surgical scars.
Review
Methodology
Study Design
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to assess the effectiveness of microneedling for treating anterior neck surgical scars. The evaluation process upheld integrity and transparency.
Study Selection Criteria
The inclusion and exclusion criteria were generated using the Population, Intervention, Comparison, Outcomes, and Study design (PICOS) model, summarised in Table 1.
This review included studies that specifically examined microneedling for surgical scars on the anterior neck only. Only studies employing objective scar assessment tools, like the Patient and Observer Scar Assessment Scale (POSAS), Vancouver Scar Scale (VSS), or Global Aesthetic Improvement Scale (GAIS), were eligible for selection. To maintain methodological rigour, we included randomised controlled trials (RCTs), cohort studies, observational studies, and case reports that evaluated microneedling as the sole treatment for anterior neck surgical scars. Only studies published in English within the past 25 years involving human subjects were eligible.
Studies were excluded if they focused on non-surgical scars, such as those resulting from acne, burns, or trauma, as these scars may respond differently to microneedling than surgical scars. Studies evaluating microneedling in combination with other interventions, such as laser therapy or platelet-rich plasma (PRP), were also excluded since these adjunctive treatments could confound the assessment of microneedling as an independent intervention. Moreover, this review did not include animal studies or conference abstracts lacking robust clinical evidence.
Search Strategy
A systematic search was conducted in the Cochrane Central Register of Controlled Trials, PubMed, Embase, Web of Science, and Google Scholar to identify relevant studies. The search was limited to articles published in English within the last 25 years. The reference lists of included studies were manually screened to identify additional relevant publications. Full search terms are detailed in Appendix 1.
Study Selection
A total of 90 records were identified through database and register searches (databases = 4, registers = 1). After removing 13 duplicate records, 77 were screened based on titles and abstracts. Of these, 68 were excluded due to irrelevance to the review focus. Nine full-text articles were assessed for eligibility, all of which were excluded for not specifically addressing anterior neck scar outcomes. Consequently, no studies met the inclusion criteria for this review (Figure 1).
PRISMA flow diagramPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Two independent reviewers then performed a thorough full-text assessment of the remaining nine articles using predefined eligibility criteria and the Scottish Intercollegiate Guidelines Network (SIGN) checklist for critical appraisal. Both reviewers agreed that none of these studies met the inclusion criteria, primarily due to the absence of research specifically evaluating microneedling for surgical scars on the anterior neck. Consequently, no studies were included in this systematic review (Appendix 2).
Results
No studies meeting the inclusion criteria were found, highlighting a significant gap in the literature regarding microneedling for anterior neck surgical scars. Given the established efficacy of microneedling in improving scars in other anatomical regions, there is an urgent need for further research to determine its effectiveness in anterior neck scars. This underscores the importance of our systematic review plan and its potential impact on scar management.
Discussion
Effectiveness of Microneedling
Studies evaluating microneedling for post-surgical scars have demonstrated significant reductions in standardised scar assessment scores. A study involving 25 patients with surgical scars found that three microneedling sessions, spaced four weeks apart, led to a 50% decrease in POSAS scores, from 23.7 ± 1.8 before treatment to 11.7 ± 1.0 at 16-week follow-up (p < 0.001) [17]. Similarly, an RCT assessing microneedling for post-abdominal surgical scars following deep inferior epigastric perforator (DIEP) flap-reconstruction found that treated scars exhibited a statistically significant improvement in POSAS scores at nine months post-treatment (median 17 vs. 21.4, p < 0.05) [18].
Although these studies did not focus on anterior neck surgical scars, they prove that microneedling can significantly enhance scar texture, pigmentation, and overall aesthetic appearance in post-surgical patients. Systematic reviews evaluating microneedling across various skin conditions, including atrophic acne scars, hypertrophic scars, keloids, and striae distensae, have also reported noteworthy improvements when microneedling is used alone or combined with adjunctive treatments. Importantly, these reviews highlight microneedling’s comparable effectiveness to other established modalities but with fewer adverse effects and shorter recovery periods, further supporting its potential application to visible and cosmetically sensitive areas like the anterior neck [19,20] Given that the neck is similarly exposed and holds high cosmetic importance, it is reasonable to hypothesise that microneedling would offer comparable benefits for anterior neck scars.
Given the similar cosmetic importance of anterior neck and facial scars, microneedling studies focusing on facial surgical scars are particularly relevant. One prospective study assessed microneedling outcomes across various scar types, including facial surgical scars, and found that all patients experienced at least a 50% improvement in scar appearance after an average of 2.5 treatments. Notably, over 80% of patients observed a 50% to 75% improvement, and 65% of patients demonstrated over 75% improvement in their scar scores (p < 0.001) [20]. These results indicate that microneedling is effective for surgical scars and especially advantageous for scars in prominent areas, such as the face and, by extension, the anterior neck.
Given that both facial and anterior neck scars share high visibility and patient concerns regarding aesthetic outcomes, these findings suggest that microneedling may be a valuable treatment for improving anterior neck scars following thyroidectomy, parathyroidectomy, and other cervical surgeries. However, due to the unique anatomical characteristics of the anterior neck, including thinner skin, fewer sebaceous glands, and increased movement, additional studies and targeted clinical trials focusing on optimal treatment parameters (needle depth, session frequency, and timing of initiation) for anterior neck scars are required to establish evidence-based clinical guidelines.
Optimal Timing for Initiating Microneedling Post-surgery
Traditionally, interventions to improve surgical scars have been delayed until the scar fully matures, typically between six and 12 months post-operatively. However, emerging evidence suggests that earlier initiation of microneedling may yield superior outcomes. One study evaluated the effects of microneedling on post-surgical scars, comparing early treatment (initiated at six to seven weeks post-operatively) with later treatment (commenced at 13 to 16 weeks post-operatively). The study utilised the POSAS to measure scar quality. Results indicated that the early treatment group experienced a significant improvement in POSAS scores, decreasing from 16.8 to 8.1, whereas the later treatment group showed a reduction from 26.1 to 14.2. The difference in improvement between the two groups was statistically significant (p < 0.04), suggesting that initiating microneedling earlier in the post-operative period may lead to better scar outcomes [21].
Needle Depth
The appropriate needle depth for microneedling varies depending on scar thickness, skin structure, and anatomical region. Studies on post-surgical facial and abdominal scars suggest that a depth of 1.5-2.0 mm effectively penetrates the dermis to stimulate collagen remodelling while minimising adverse effects such as prolonged erythema or epidermal damage (p < 0.05) [14]. Given that the anterior neck has thinner skin than the abdomen but shares similarities with the face, a needle depth of 1.0-1.5 mm may be optimal for microneedling in this area, allowing for adequate collagen stimulation without excessive tissue trauma.
Session Frequency
The frequency and total number of microneedling sessions significantly impact treatment efficacy. Studies assessing post-operative microneedling in surgical scars recommend a minimum of three to six sessions, spaced four to six weeks apart, to achieve statistically significant improvements in POSAS and VSS scores (p < 0.001) [22]. This interval allows for sufficient dermal remodelling between sessions while ensuring progressive scar pliability, pigmentation, and texture improvement. Given the high cosmetic importance of the anterior neck, a similar treatment schedule is likely appropriate for optimising scar remodelling in this region.
Overall, the findings highlight the potential role of microneedling as an effective intervention for surgical scars on the neck, with promising evidence from other surgical sites suggesting that early treatment initiation, appropriate needle depth, and optimal session frequency may significantly enhance scar remodelling and aesthetic outcomes. However, further research is required to establish definitive clinical guidelines specific to anterior neck scars.
Conclusions
This review emphasises the potential effectiveness of microneedling as a minimally invasive option for treating surgical scars on the anterior neck. Although no direct studies have assessed its use in this area, evidence from other types of surgical scars indicates that microneedling can significantly enhance scar texture, pigmentation, and overall appearance, resulting in high patient satisfaction and minimal complications. Findings suggest that starting early microneedling treatment, approximately six weeks post-operatively, enhances scar remodelling compared to traditional delayed interventions. Moreover, treatment protocols consisting of three to six sessions, spaced four to six weeks apart, with needle depths adjusted to 1.0-1.5 mm, appear optimal for anterior neck scars. These parameters account for the uniquely thin and delicate nature of the anterior neck skin, thus maximising therapeutic efficacy. Clinicians should consider integrating microneedling into standard neck surgery scar management protocols to enhance aesthetic outcomes. Further research is needed to establish long-term effects beyond 12 months and to develop specific guidelines for anterior neck scars. Future studies should focus on RCTs to confirm ideal treatment timing, frequency, and needle depth for this anatomical region.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Scar formation and patient satisfaction after thyroidectomy with and without surgical drains Int Surg J Kim HY Kim HS Kim HI Park JH Yi HS 2692269762019
- 2The perception of scar cosmesis following thyroid and parathyroid surgery: a prospective cohort study Int J Surg Arora A Swords C Garas G 38432520162660296710.1016/j.ijsu.2015.11.021 · doi ↗ · pubmed ↗
- 3The natural neck crease as an anatomic landmark for thyroid surgery incision Surgeon Elkanovich T Hajouj M Ronen O 07119202110.1016/j.surge.2020.09.00633139198 · doi ↗ · pubmed ↗
- 4Skin: anatomy and healing Plastic Neurosurgery Winston KR French B Ketch LL 337Cham Springer 2023
- 5Impact of endocrine disorders on skin disorders Endocrinology and Systemic Diseases Bonamonte D Filoni A 399434 Cham Springer 2021
- 6Recontouring, resurfacing, and scar revision in skin cancer reconstruction Facial Plast Surg Clin North Am Brenner MJ Perro CA 4694871720091969892410.1016/j.fsc.2009.04.006 · doi ↗ · pubmed ↗
- 7Neck lifting variations Facial Rejuvenation: Art and Clinical Practice Mittelman H Rosenberg JD 653670 Berlin Springer 2011
- 8Scar treatments: preclinical and clinical studies J Am Coll Surg Reish RG Eriksson E 71973020620081838747910.1016/j.jamcollsurg.2007.11.022 · doi ↗ · pubmed ↗