Stroke, Fever, and Clot Microbiology Analysis: A Case Report
Mariana Baptista, Pedro Tavares de Almeida, Gabriela Abreu, Guilherme Jesus, Tiago Gregório

TL;DR
A young man with stroke and fever was found to have infective endocarditis, highlighting the need to consider this condition in similar cases.
Contribution
The case demonstrates the value of microbiological analysis of retrieved clots in diagnosing infective endocarditis.
Findings
The patient's stroke was caused by an embolus from infective endocarditis.
Microbiological analysis of the retrieved clot identified Streptococcus anginosus.
The patient recovered well after surgery and targeted antibiotic treatment.
Abstract
Infective endocarditis (IE) is a rare but serious life-threatening disease, often presenting with highly variable clinical symptoms. Risk factors for this condition include valvular heart disease, age, medical procedures, dental procedures, and intravenous drug use. Patients with IE may exhibit valve dysfunction, heart failure, or neurological complications such as stroke, the latter being caused by an embolus originating from valvular vegetations that occlude more distal vessels in the cerebral circulation. Diagnosis is based on the modified Duke criteria. We report a case of a 20-year-old male patient who presented to the emergency department with the acute onset of aphasia, right-sided hemiparesis, and fever. Neurological examination revealed a National Institute of Health Stroke Scale score of 10, and computed tomography (CT) angiography confirmed a left middle cerebral artery…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
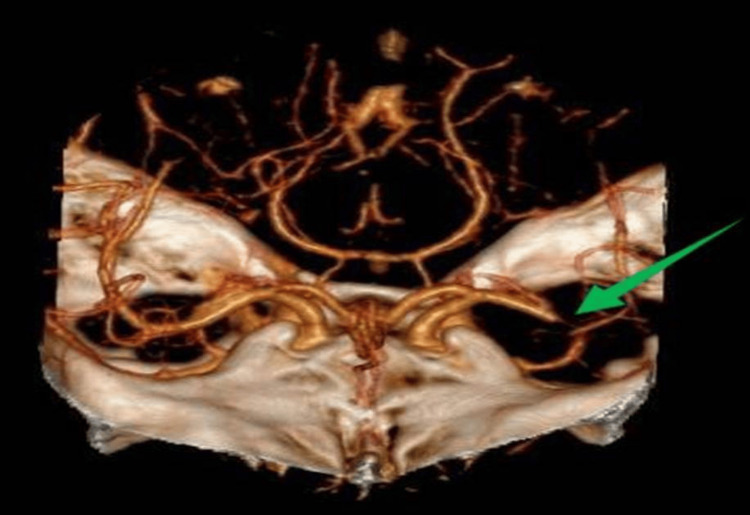 Figure 1
Figure 1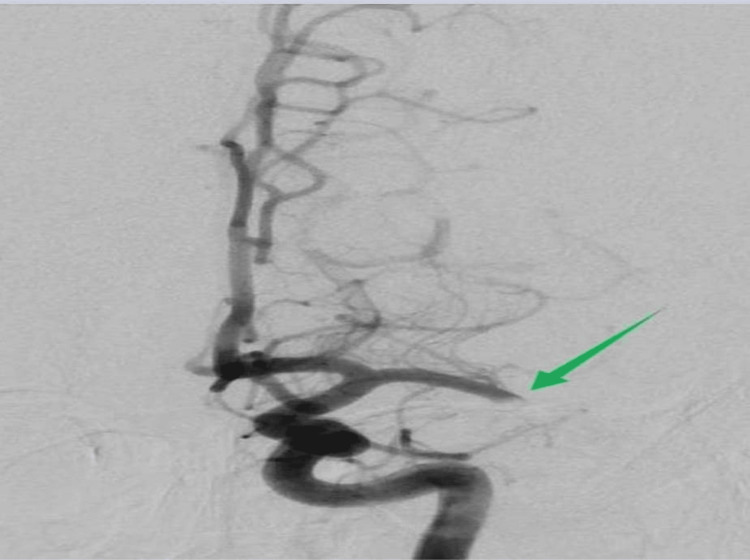 Figure 2
Figure 2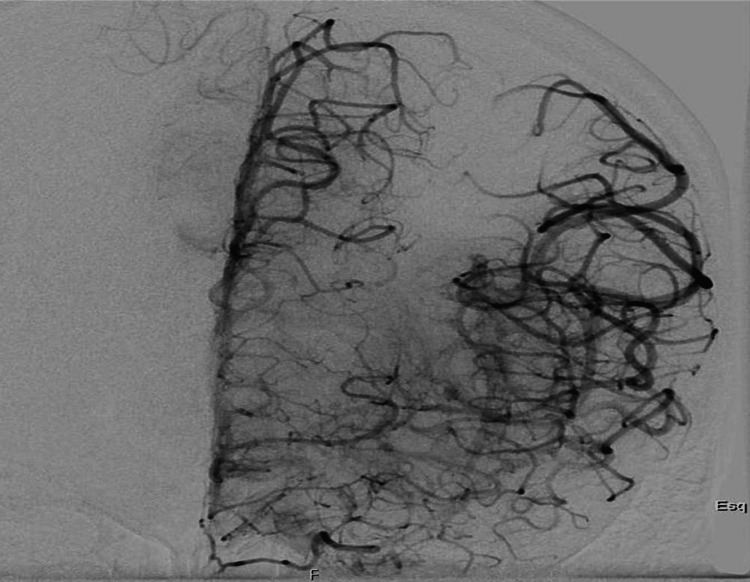 Figure 3
Figure 3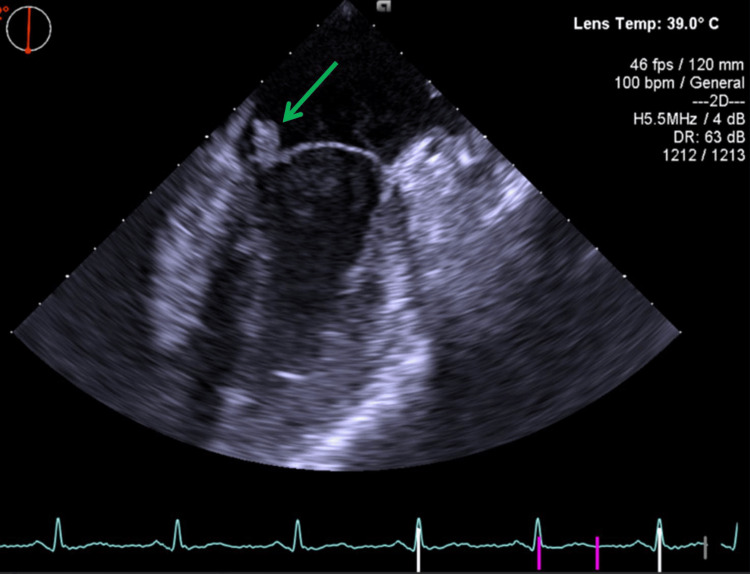 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Diphtheria, Corynebacterium, and Tetanus · Streptococcal Infections and Treatments
Introduction
Infective endocarditis (IE) is a rare but serious infectious disease with high morbidity and mortality [1]. The incidence of IE ranges from three to fifteen cases per 100,000 persons per year [1,2]. This variation in incidence likely reflects differences in the prevalence of risk factors in the studied populations, such as structural heart disease, intravenous drug use, medical procedures, and comorbidities like diabetes or chronic kidney disease [3]. Clinical presentation is highly variable and depends on the underlying cardiac condition and preexisting comorbidities. Up to 90% of patients present with constitutional symptoms; however, other possible presentations include valve dysfunction, heart failure, or symptoms due to peripheral embolization, including stroke [4,5]. Stroke is reported to complicate up to 35% of IE cases, with the risk being higher for patients with large mobile vegetations and Staphylococcus aureus infection. However, other potential embolization sites include the bone, joints, kidney, and spleen [2]. Diagnosis of IE is based on the modified Duke criteria, which include clinical (fever, predisposing heart disease, and vascular phenomena), imaging (echocardiographic signs of vegetation or new-onset valvular insufficiency), immunological (rheumatoid factor, Osler's nodes, Roth's spots), and microbiological (blood cultures) criteria [2,4]. S. aureus is the most frequent cause of IE, representing approximately 26.6% of all cases, followed by viridans group streptococci (18.7%), other streptococci (17.5%), and enterococci (10.5%) [1]. In this case report, we address a case of large vessel occlusion stroke in a patient with endocarditis and explore the potential of microbiological analysis of the clot retrieved with thrombectomy in identifying the causative microorganism and guiding antibiotic therapy.
Case presentation
A 20-year-old male patient with no significant medical history and no chronic medication presented to the emergency department with the sudden onset of aphasia and right-sided hemiparesis that started four hours earlier. The stroke fast-track pathway was activated on admission, and the patient was quickly evaluated. On physical examination, he had a respiratory rate of 25 breaths/minute, a blood pressure of 115/62 mmHg, a heart rate of 145 beats/minute, and a tympanic temperature of 40°C. On neurological examination, the patient was alert, with mild motor aphasia, right homonymous hemianopsia, right central facial paralysis, right-sided hemiparesis, and ipsilateral sensory loss. His National Institutes of Health Stroke Scale score was 10, compatible with a moderate stroke.
Blood samples were sent for laboratory tests, and a computed tomography (CT) scan of the brain was performed, which showed only a small lateral lenticular infarct (Alberta Stroke Program Early CT Score of 9, consistent with mild ischemic changes and good prognosis). CT angiography demonstrated an occlusion of the distal M1 segment of the left middle cerebral artery, with no evidence of significant atherosclerotic plaques (Figure 1).
Occlusion of the M1 segment of the left middle cerebral artery, as shown by computed tomography angiography
Since the diagnostic criteria for IE were not met at this time, the patient underwent thrombolysis followed by thrombectomy with successful recanalization (Modified Treatment in Cerebral Infarction score of 3). The thrombus was sent for microbiological analysis due to clinical suspicion of endocarditis (Figures 2, 3). This diagnosis was suspected based on clinical criteria of fever and cerebral embolization, as laboratory tests and echocardiography results were unavailable.
Angiography prior to thrombectomy
Angiography after thrombectomy with effective recanalization
Later on, the laboratory tests revealed a leukocytosis of 16,460/uL (3,600-11,000/uL) with neutrophilia, an elevated erythrocyte sedimentation rate of 64 mm/hour (0-20 mm/hour), and an elevated C-reactive protein of 14 mg/dL (0-0.5 mg/dL), with no other significant findings. Blood cultures were obtained before any antibiotics were administered, and a transthoracic echocardiogram was performed, which showed an echodense mass on the mitral valve leaflet causing mild-to-moderate mitral regurgitation. Empiric antibiotic therapy was started with vancomycin and gentamicin, and a transesophageal echocardiogram was requested, which confirmed the presence of an 11-mm vegetation on the mitral valve and better characterized the regurgitation as moderate to severe (Figure 4).
Vegetation on the leaflet of the mitral valve in transesophageal echocardiogram
Blood cultures showed the presence of Streptococcus anginosus in all four bottles of the two sets of blood cultures taken, making the diagnosis of IE. The same microorganism was also isolated from the thrombus, and antibiotic therapy was adjusted to ceftriaxone, rifampicin, and gentamicin according to the antibiotic susceptibility testing. The patient underwent mitral valve replacement with a mechanical prosthesis on the fifteenth day of hospitalization, without complications. The timing of surgery was chosen in an attempt to strike a balance between preventing further embolization and minimizing the risk of hemorrhagic transformation of the cerebral infarct, given that anticoagulation was required for the procedure. Prior to surgery, dental care was optimized, as the patient's only identifiable risk factor for IE was poor oral health, with dental infections that had previously required tooth extraction. The patient demonstrated a good clinical evolution with complete recovery from the focal neurological deficits and completed six weeks of antibiotic therapy after blood cultures became negative.
Anticoagulation with warfarin was initiated during hospitalization due to the mechanical nature of the prosthetic valve, with enoxaparin bridging at the start of anticoagulation to further reduce the risk of stroke or systemic embolization. Regular monitoring of the international normalized ratio (INR) was used to ensure therapeutic anticoagulation levels and minimize the risk of bleeding, with a target INR of 2.5-3.5. In addition, continuous clinical and laboratory monitoring was performed, with serial complete blood counts, assessment of hemoglobin and hematocrit levels, and observation for any clinical signs of hemorrhage.
At one-year follow-up, the patient remained clinically stable, without any new neurological complications, and scored zero on the modified Rankin Scale. A follow-up echocardiogram demonstrated a normofunctioning mechanical prosthetic valve in the mitral position, preserved left ventricular systolic function, and no evidence of residual vegetation or other structural abnormalities.
Discussion
It is estimated that 30% of patients with IE will develop CT-confirmed symptomatic cerebrovascular complications during their disease, but asymptomatic lesions are present in up to 80% [2]. Most clinically evident strokes are ischemic due to distal embolization of fragments from left-sided valvular vegetations, but cerebral hemorrhage can also occur due to the rupture of mycotic aneurysms [2,4,6,7]. Additionally, 10% of all strokes are associated with bacteremic infections, mostly endocarditis but also sepsis and meningitis. Although less common, strokes may be linked to viral or fungal infections [8,9].
An elevated body temperature in a patient presenting with acute stroke should raise concern about possible IE. If the diagnosis is strongly suspected, intravenous thrombolysis is not recommended due to the possible presence of mycotic aneurysms and inherent risk of cerebral hemorrhage, but mechanical thrombectomy can be beneficial in selected patients with large-vessel occlusion [2,10]. In this case report, the acute presentation of disease and the fact that diagnostic criteria were not gathered at the time of stroke treatment led to the administration of thrombolytic treatment, followed by thrombectomy. For patients with IE presenting with stroke, definitive blood culture results are typically not available at the time of disease presentation [2], and as such, clinicians should maintain a high level of suspicion for this diagnosis. Should the diagnosis have been more strongly considered on disease presentation, it would have been acceptable for this patient to proceed directly to thrombectomy and forego thrombolysis. This treatment, however, is also not exempt from risks such as cerebral hemorrhage, access site complications, distal embolization from clot dislodgment, vessel injury, and reperfusion injury [11].
Only approximately 40% of all blood cultures are positive in patients with endocarditis [12]. Potential causes for this low sensitivity include previous antibiotic treatment, IE caused by fastidious organisms, nonbacterial pathogens, or intracellular bacteria [13]. Although the diagnosis can still be made in patients with negative blood cultures, positive cultures can also assist in the selection of effective antimicrobial therapy. Our case report demonstrates that it is possible to isolate the culprit microorganism from clots obtained from thrombectomy, with other authors also reporting similar results [14,15]. Abdel-Wahed et al. reported a case of a 72-year-old woman with a bioprosthetic aortic valve who presented with a left middle cerebral artery stroke. This patient also presented with signs of infection, and endocarditis was diagnosed; the infectious agent was identified on clot analysis. Hernández-Fernández et al. [16] studied a consecutive sample of 65 patients who underwent thrombectomy for stroke over 24 months and identified bacteria in four, of these two being diagnosed with IE (50%), one with urinary tract infection, and one with respiratory septicemia. Another potentially useful test is histopathological analysis of the clot, which may allow visualization of infective bacteria with appropriate staining. This was elegantly demonstrated in a study by Bhaskar et al. involving four patients [17]. These results should be interpreted cautiously, given that they are drawn from case reports and small-scale observational studies involving a limited number of patients. Therefore, positive clot microbiology analysis should not be considered specific for IE but should be integrated with clinical, laboratory, and echocardiographic findings, which may also help determine whether the results reflect true infection or represent a contamination phenomenon. Such findings have led clinical societies to propose that embolic material retrieved from thrombectomy in such circumstances be sent for microbiological analysis [2], even though a positive microbiological growth in retrieved clots is not pathognomonic for IE.
To assist in diagnosing IE, the Duke criteria were proposed in 1994 and updated in 2000 (modified Duke Criteria). These criteria are divided into pathologic (histologic or microbiological analysis of valve tissue or abscess) and clinical (bacteremia, echocardiographic evidence of vegetations or new-onset valvular insufficiency, predisposing structural heart disease, fever, embolic, and immunological phenomena), the latter being further categorized into major and minor criteria. According to this classification, a definitive diagnosis of endocarditis can be made if patients have any pathologic criterion, two major clinical criteria, one major and three minor clinical criteria, or five minor clinical criteria [18,19]. However, these criteria were proposed at a time when thrombectomy was not performed for stroke treatment, as it is today. More recently, the modified Duke criteria have been updated by the International Society for Cardiovascular Infectious Diseases. Among other changes, this new diagnostic schema includes the isolation of an infectious microorganism from an arterial embolus as a pathologic criterion, while also emphasizing the need to carefully exclude bacterial contamination (particularly for commensal bacteria of the skin) [20]. Therefore, bacteriological analysis of the retrieved thrombus, in appropriately selected patients, can be useful in diagnosing endocarditis and can also guide antimicrobial therapy, especially in cases where blood cultures are negative. It should be noted, however, that no study to date has specifically evaluated the impact of this new criterion on the diagnosis of endocarditis in the context of stroke, nor can it be recommended as the standard of care for all stroke patients. Further studies are needed to clarify the role of microbiological analysis of thrombus in stroke thrombectomy, but it should be strongly considered in patients where IE is considered a potential underlying cause.
Conclusions
Endocarditis should be suspected in patients presenting with stroke and fever, especially in those without cardiovascular risk factors who also exhibit a cardiac murmur. Thrombolysis is not recommended when endocarditis is strongly suspected. However, a definitive diagnosis is often not possible at the time of stroke presentation, as it requires correlation of clinical findings with echocardiogram imaging and blood cultures. The latter can even be negative, particularly in patients who recently received antibiotic therapy or are infected with fastidious microorganisms, intracellular pathogens, or nonbacterial pathogens. Thrombectomy remains an acceptable and effective treatment for patients with large vessel occlusion stroke, albeit it still carries a small risk of vessel injury or clot dislodgment. Microbiological analysis of the retrieved clot does not replace the need for blood cultures in the diagnosis of endocarditis but may aid in the identification of the infective agent and in guiding antibiotic therapy, particularly for patients with negative blood cultures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Infective endocarditis: a contemporary update Clin Med (Lond) Rajani R Klein JL 31352020203194172910.7861/clinmed.cme.20.1.1PMC 6964163 · doi ↗ · pubmed ↗
- 22023 ESC guidelines for the management of endocarditis Eur Heart J Delgado V Ajmone Marsan N de Waha S 394840424420233762265610.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 3Predisposing factors of infective endocarditis and their relation to microbiological findings Eur Heart J Acute Cardiovasc Care Gomez Gonzalez A Padilla Rodriguez G Nunez Ruiz M 142025
- 4An approach to a patient with infective endocarditis S Afr Med J Hitzeroth J Beckett N Ntuli P 1451501062016 https://pubmed.ncbi.nlm.nih.gov/27303769/2730376910.7196/samj.2016.v 106i 2.10327 · doi ↗ · pubmed ↗
- 5Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-prospective cohort study Arch Intern Med Murdoch DR Corey GR Hoen B 46347316920091927377610.1001/archinternmed.2008.603PMC 3625651 · doi ↗ · pubmed ↗
- 6Thrombo-embolic complications in bacteraemic infections Eur Heart J Valtonen V Kuikka A Syrjänen J 202314 Suppl K 1993 http://pubmed.ncbi.nlm.nih.gov/8131784/8131784 · pubmed ↗
- 7Heart-brain relationship in stroke Biomedicines Kelley RE Kelley BP 1835920213494465110.3390/biomedicines 9121835 PMC 8698726 · doi ↗ · pubmed ↗
- 8Prevalence and prognostic impact of stroke in a national cohort of infective endocarditis Int J Stroke Álvarez-Zaballos S Vázquez-Alen P Muñoz P 9899981920243870872210.1177/17474930241255560 · doi ↗ · pubmed ↗