Endogenous Endophthalmitis Secondary to Prostate Abscess
Nada A Saleh, Shreeker Patel, Syed Quadri

TL;DR
A man with no known risk factors developed eye infection from a prostate abscess, highlighting the need for quick diagnosis and treatment.
Contribution
This case report highlights endogenous endophthalmitis caused by a prostate abscess in a previously healthy individual.
Findings
Endogenous endophthalmitis was diagnosed through fundoscopy and confirmed by blood cultures.
Prostatic abscesses were identified as the source of bacteremia via CT imaging.
Timely intravitreal and intravenous antibiotic treatment led to gradual vision improvement.
Abstract
Endophthalmitis is a severe ophthalmic emergency that necessitates immediate intervention. Most cases are exogenous, originating from eye surgeries, intravitreal injections, or penetrating injuries. Endogenous endophthalmitis occurs when the infection is spread hematogenously, usually as a result of bacteremia. We present a healthy individual with no predisposing factors who presented to the emergency department with decreased left vision. A male in his late sixties with a medical history of hypertension and hyperlipidemia presented to the ophthalmology clinic with complaints of left eye pain, redness, and decreased vision. Diagnosis of endogenous endophthalmitis was made through fundoscopy, and the patient received intravitreal injections of vancomycin and ceftazidime in the left eye. He was subsequently admitted to the hospital, where blood and urine cultures grew…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
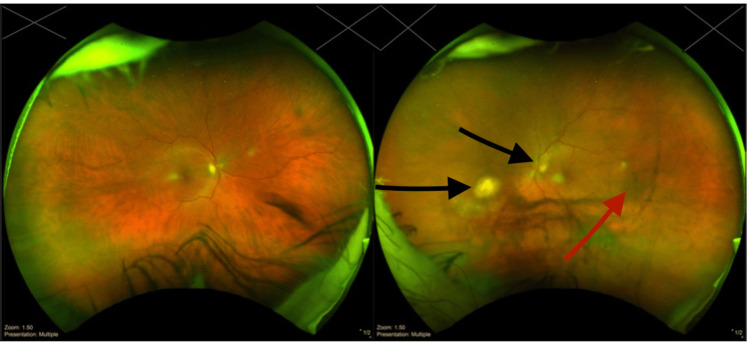 Figure 1
Figure 1 Figure 2
Figure 2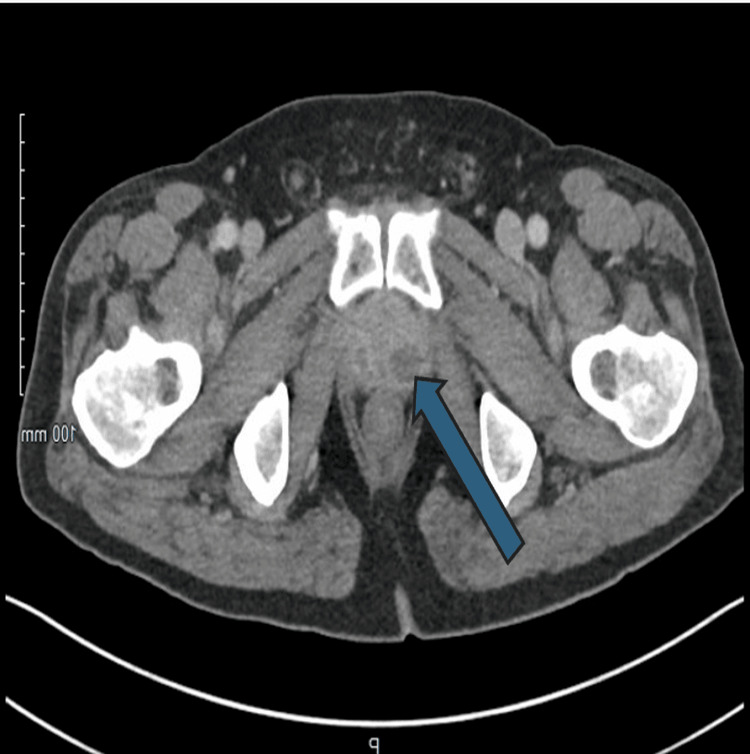 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Intraocular Surgery and Lenses · Corneal surgery and disorders
Introduction
Endophthalmitis is an ophthalmic emergency characterized by inflammation of the intraocular cavities and requires immediate diagnosis and intervention to preserve vision [1]. While most cases are exogenous, arising from surgical procedures, intravitreal injections, or ocular trauma, endogenous endophthalmitis results from hematogenous spread of infection, often in the setting of bacteremia or fungemia [1]. This form represents only 2-8% of all endophthalmitis cases, with Staphylococcus aureus and Streptococcus pneumoniae among the most frequently implicated organisms. The first reported case was in 1856, caused by recurrent Klebsiella pneumoniae in a 58-year-old male patient with a history of intravenous drug use (IVDU) [2]. Risk factors for endogenous endophthalmitis include immunosuppression, IVDU, and indwelling catheters [3].
Clinical presentation is variable but may include ocular pain, redness, decreased visual acuity, floaters, and photopsia. Diagnosis often requires a multimodal approach involving clinical examination, fundoscopy, ocular ultrasound, neuroimaging, and culture data. Treatment includes systemic antibiotics as well as supplemental use of intravitreal antimicrobials and, in some cases, vitrectomy [4]. Here, we present a rare case of endogenous methicillin-resistant Staphylococcus aureus (MRSA) endophthalmitis secondary to a prostatic abscess in an immunocompetent patient with no history of IVDU, highlighting the need for a high index of suspicion even in low-risk populations.
Case presentation
A male in his late sixties with a history of hypertension and hyperlipidemia presented to the ophthalmology clinic with 2-3 days of left eye pain, redness, and decreased vision. He was referred to the emergency department for further evaluation.
Initial symptoms
Two weeks prior to the ocular complaints, the patient reported progressive dysuria, urinary hesitancy, and incomplete bladder emptying.
Clinical examination
On arrival, the patient was afebrile and hemodynamically stable. Visual acuity was 20/50 in the right eye and limited to hand motion in the left eye. Intraocular pressure (IOP) was 19 mmHg in the left eye and 15 mmHg in the right. Slit-lamp exam of the left eye revealed a hypopyon, conjunctival injection, and significant vitritis. The fundus exam was notable for left eye vitreous opacities and a choroidal lesion (Figure 1). The retina was poorly visualized with an absent red reflex.
Wide fundus photo of both eyes. Fundus photo of the left eye showing vitreous opacities and vitreous veils (red arrow), which indicates an area of active infection (black arrows)
Immediate interventions
The patient received intravitreal vancomycin and ceftazidime, and vitreous fluid was collected for culture. Systemic workup was initiated with blood and urine cultures.
Imaging
Brain MRI with and without contrast was pursued to rule out any other sources of infection or intracranial complications. Imaging demonstrated scleral thickening and periorbital edema consistent with endophthalmitis (Figure 2). Abdominopelvic computed tomography revealed multiple prostatic abscesses (Figure 3).
Mild left proptosis, circumferential scleral thickening and enhancement with surrounding orbital fat and edema consistent with endophthalmitis (white arrow)
Enlarged prostate with surrounding inflammatory stranding and internal cystic lesions, the largest on the right measuring up to 1.8 cm (marked with the blue arrow)
Microbiological confirmation
Both blood and vitreous cultures grew MRSA. Urinalysis showed leukocytes and nitrates; urine culture also confirmed MRSA. Fungal cultures were negative.
Hospital course & outcome
The patient was started on intravenous (IV) vancomycin and linezolid based on susceptibility testing (vancomycin MIC 1, linezolid MIC 2). Echocardiography ruled out infective endocarditis. Serial blood cultures confirmed clearance by day 3. Visual symptoms progressively improved; on day 5, the hypopyon resolved and IOP normalized to 14 mmHg in the left eye. At discharge, the patient had near-baseline visual function. He was discharged on IV vancomycin 1.25 g BID and oral linezolid 600 mg twice a day for a six-week course, with scheduled urology follow-up.
Discussion
Endogenous endophthalmitis is a rare but vision-threatening infection, typically seen in patients with identifiable risk factors such as IVDU, diabetes, and indwelling catheters [1]. This case is notable due to the absence of traditional risk factors in an otherwise healthy patient.
Obstructive urinary symptoms likely led to prostatic abscess formation and subsequent hematogenous dissemination of MRSA. The left-sided ocular involvement is atypical. In hematogenous spread, the posterior segment is typically involved, and the right eye is more frequently affected due to direct flow from the right carotid artery [1].
The literature indicates that approximately 40% of endogenous endophthalmitis cases in the USA are due to bacteremia secondary to endocarditis [1]. IVDU is another well-documented cause [5]. A case report from 2022 described a 34-year-old man with a history of IVDU who developed endogenous endophthalmitis secondary to MRSA infection following COVID-19 pneumonia [6].
Most patients with endogenous endophthalmitis present with eye pain and/or decreased vision. However, studies suggest that many patients do not exhibit systemic symptoms (such as fever) or other pertinent physical findings, leading to misdiagnosis. Thus, clinicians should maintain a high index of suspicion when evaluating patients with risk factors such as bacteremia or IVDU who present with ocular complaints.
Diagnosis can be confirmed through an ultrasound evaluation of the posterior segment, which can help detect vitreous involvement by identifying echoes within the vitreous. Ocular sampling, including vitreous or anterior chamber tap or biopsy, can be performed for culture and microorganism isolation [7]. While fundoscopy and ocular ultrasound remain the mainstays of diagnosis, MRI was employed in this case to rule out intracranial pathology and confirmed orbital involvement. Though not routinely used for diagnosing endophthalmitis, MRI can offer value in complex presentations or in facilities without ophthalmology coverage. MRI may be valuable in ruling out exogenous causes, identifying structural abnormalities, and aiding in cases with an unclear source of infection.
Our patient was treated with a combination of intravitreal and systemic antimicrobials. The most effective agents for achieving therapeutic levels in the vitreous fluid include meropenem, linezolid, and moxifloxacin [8]. Systemic moxifloxacin is a viable option due to its excellent intraocular penetration and broad-spectrum coverage. However, it does not cover MRSA, which makes it unsuitable for this case [9]. Intravitreal antibiotics remain the preferred route, particularly in cases of penetrating injuries [9]. The rationale for combining vancomycin and linezolid, as previously discussed, is their ability to penetrate ocular tissues and their effectiveness against MRSA. However, there is limited literature supporting this specific combination, and further research is needed. Systemic linezolid, which has excellent intraocular penetration, was chosen alongside vancomycin due to the MRSA susceptibility profile. Given the risk of linezolid-associated optic neuropathy, baseline and follow-up visual assessments were performed. The patient remained asymptomatic, and no toxicity was observed during the six-week course.
This case reinforces the importance of early recognition and aggressive treatment, even in atypical presentations. It also illustrates the importance of a comprehensive diagnostic approach-integrating clinical exam, imaging, and culture results.
Conclusions
Endogenous endophthalmitis is a vision-threatening emergency that requires rapid recognition and aggressive management to prevent irreversible ocular damage and vision loss. This case highlights the importance of maintaining a high index of suspicion for endogenous endophthalmitis in patients with bacteremia and ocular symptoms, even in the absence of classic systemic signs. A delayed or missed diagnosis can lead to devastating complications, including blindness or even loss of the eye. Early clinical suspicion, prompt diagnostic evaluation, and timely initiation of appropriate antimicrobial therapy and surgical intervention, when necessary, are critical in optimizing patient outcomes. Increased awareness among clinicians, especially those managing patients with risk factors such as immunosuppression or IVDU, is essential to improving early detection and treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bacterial and fungal endophthalmitis Clin Microbiol Rev Durand ML 5976133020172835632310.1128/CMR.00113-16PMC 5475221 · doi ↗ · pubmed ↗
- 2An unusual case of recurrent endogenous Klebsiella endophthalmitis Eye (Lond) Tsai AS Lee SY Jap AH 16301631242010 https://doi.org/10.1038/eye.2010.952055933010.1038/eye.2010.95 · doi ↗ · pubmed ↗
- 3Endogenous endophthalmitis: diagnosis, management, and prognosis J Ophthalmic Inflamm Infect Sadiq MA Hassan M Agarwal A 32520152652556310.1186/s 12348-015-0063-y PMC 4630262 · doi ↗ · pubmed ↗
- 4The role of systemic antimicrobials in the treatment of endophthalmitis: a review and an international perspective Ophthalmol Ther Grzybowski A Turczynowska M Schwartz SG Relhan N Flynn HW Jr 485498920203261359110.1007/s 40123-020-00270-w PMC 7406615 · doi ↗ · pubmed ↗
- 5Endogenous endophthalmitis in an urban university setting: characteristics, treatment, and outcomes J Vitreoretin Dis Budoff G Zarbin MA Bhagat N 135141520213700907710.1177/2474126420951979 PMC 9979060 · doi ↗ · pubmed ↗
- 6Endogenous endophthalmitis due to methicillin-resistant Staphylococcus aureus bacteremia in a patient with COVID-19Proc (Bayl Univ Med Cent) Brotherton T Nwankwo E Das D Fritz A 1971983520223526145110.1080/08998280.2021.1990823 PMC 8865298 · doi ↗ · pubmed ↗
- 7Endophthalmitis Stat Pearls [Internet] Simakurthy S Tripathy K Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 559079/32644505 · pubmed ↗
- 8Revisiting systemic treatment of bacterial endophthalmitis: a review of intravitreal penetration of systemic antibiotics Clin Microbiol Infect Brockhaus L Goldblum D Eggenschwiler L Zimmerli S Marzolini C 136413692520193077152910.1016/j.cmi.2019.01.017 · doi ↗ · pubmed ↗