Hypothesis: Taurine therapy of nephropathic cystinosis may correct the deficiencies of cysteamine therapy
Jess G. Thoene

TL;DR
Taurine may address deficiencies in current cystinosis treatment by correcting metabolic and physiological issues not resolved by cysteamine.
Contribution
The hypothesis proposes taurine as a novel therapeutic approach for nephropathic cystinosis based on its potential to correct unaddressed disease features.
Findings
Cystinosis patients are severely deficient in plasma taurine.
Taurine has shown potential to correct defects in other conditions similar to those in cystinosis.
A clinical trial of taurine in nephropathic cystinosis is suggested due to its safety and potential efficacy.
Abstract
Untreated nephropathic cystinosis is a lethal autosomal recessive disease. The current specific therapy, cysteamine, ameliorates the renal function loss, but does not alter the renal Fanconi syndrome, short stature, muscle weakness, male infertility, and other concerns. The primary biochemical/physiological defect in cystinosis is failure to supply cysteine to mTOR via cystinosin. This leads mTOR to react in starvation mode, which stops cell differentiation, leading to proximal tubule loss, and ultimately renal failure. It also increases apoptosis and autophagocytosis rates, which may contribute to impaired growth. Many of the defects which occur in cystinosis are corrected by taurine in other conditions as described. Cystinosis patients have been shown to be severely deficient in plasma taurine. Although use of taurine is not yet reported in cystinosis in vitro or in vivo, given the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
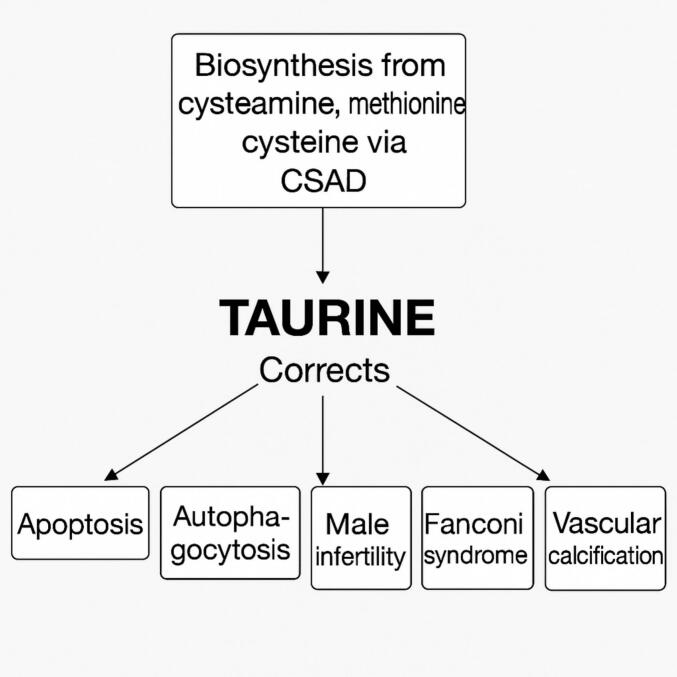 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiomedical Research and Pathophysiology · Neonatal Health and Biochemistry · Methemoglobinemia and Tumor Lysis Syndrome
Cystinosis: description, detrimental effects of CTNS mutation on mTOR, cysteamine failures
1
Cystinosis has been known as a clinical entity since early in the 20th century. Abderhalden first described two children in a family who died of inanition, and who had tiny white crystals in their liver [1]. Subsequently nephropathic cystinosis has been described with increasing detail which includes the renal Fanconi syndrome, and renal failure by about 10 years of age. Other significant clinical findings include short stature, never reaching greater than the 3rd percentile for age, hypercholesterolemia, pulmonary complications, metabolic bone disease, diabetes, cutaneous abnormalities, vascular calcifications, progressive muscle weakness, eye findings, including corneal crystals, and pigmentary retinopathy [1].
Symptomatic treatment of nephropathic cystinosis has improved over the ensuing century, but was initially limited to replacement of electrolytes and water to reduce the danger of electrolyte imbalance and dehydration. Additionally, it was found that the children develop vitamin D responsive rickets. However, no specific therapy was available to treat the underlying defect, until, in the 1970s, it was found that cystine accumulates in lysosomes of cystinotic cells [1]. In 1976, cysteamine was found to cause cystine depletion in vitro and in vivo [2,3]. Cysteamine reacts inside lysosomes in cystinotic tissues to form a new compound with cystine called cysteamine-cysteine mixed disulfide, which exits lysosomes on the intact lysine transporter [4]. The reason for the lysosomal cystine accumulation was unknown until the 1980s when it was found that the lysosomal transporter for cystine (CTNS) is mutated in cystinosis leading to an increase of cystine in lysosomes about 100-fold above normal [1].
Oral systemic cysteamine therapy for nephropathic cystinosis was subsequently approved by the US FDA in 1994. It did not prevent renal failure, but improved growth, and delayed the need for renal transplantation by about 10 years [5].
Many clinical issues are not resolved by systemic cysteamine treatment of nephropathic cystinosis. These include the renal Fanconi syndrome, which is one of the most persistent and potentially debilitating elements of the cystinotic phenotype and, although it may be partially corrected by cysteamine. Massive polyuria and failure to reabsorb electrolytes and other essential small molecules remain and cause the children to be at risk for serious dehydration and electrolyte imbalance [1]. Other adverse phenotypic developments not responsive to systemic cysteamine therapy include corneal crystals, inflammation, short stature, hypercholesterolemia, premature skin aging, metabolic bone disease, male infertility, vascular calcifications, muscle weakness, pulmonopathy, and diabetes (Table 1). Some of the abnormalities develop in adolescence or adulthood [5,6].Table 1. Clinical elements in the nephropathic cystinosis phenotype uncorrected by systemic cysteamine.Table 1. Renal Fanconi SyndromeInflammationCorneal crystalsRetinopathyDelayed renal failure (not averted)Short statureHypercholesterolemiaMale infertilityElements premature aging• Skin• Vascular calcifications• Bone changes• Muscle weakness• Pulmonary complications Diabetes• Hypothyroidism
In addition to the clinical abnormalities, nephropathic cystinosis displays abnormalities in cell physiology which contribute to the clinical phenotype (Table 2). These abnormalities center around mTOR, a serine/threonine kinase and major regulator of cell metabolic activity [7,8]. Cystinosin had previously been described as interacting with mTOR [9,10], but its centrality in cystinosis was noted in the Berquez paper [11] in which it was shown that proximal tubule (PT) cells in the kidney degrade disulfide containing proteins after endocytosis, generating cystine. Defective cystine transport from lysosomes due to mutated cystinosin stimulates Ragulator-Rag GTPase-recruitment of the mechanistic target of rapamycin complex 1 leading to its constitutive activation [11] and causing a shift away from cell specialization. It was already well established that cystinotic cells accumulate cystine from the lysosomal degradation of cystine-rich proteins [12,13], and that atubular glomeruli occur as proximal renal tubules are lost. In a study of cystinosis and normal renal biopsies, it was found that cystinotic kidneys at end stage had 69 % atubular glomeruli and 30 % atrophic glomeruli. Normal renal tissue had 4 % atubular glomeruli and 0 % atrophic glomeruli (p < 0.0001 for both comparisons [14]. This progression leads to global loss of renal filtration function [5].Table 2. Elements in cystinosis cell pathology leading to clinical phenotypes.Table 2. Loss of cell specialization• Create Renal Fanconi SyndromeIncreased apoptosisIncreased autophagyAberrant intermediate metabolism• Lipid synthesis• Nucleotide synthesis• Biogenesis of lysosomes• Nutrient sensing• Growth factor signalingAberrant osteocyte developmentAberrant myocyte developmentCystine crystal inflammatory processes
Thus it isn't cystine storage that does the damage in cystinosis, but deficiency of available cytosolic cysteine. Interestingly, neither extracellular cysteine, N-acetylcysteine nor cysteamine blunt the constitutive activation of mTOR in cystinotic cells nor restore the normal equilibrium of mTOR between cell differentiation and cell proliferation [11]. This agrees with the clinical finding that cysteamine does not affect the renal Fanconi Syndrome in cystinosis patients when started after ∼2 years of age [1], but improves GFR and improves, but does not correct, tubular function when started prior to two months of age [15]. Failure of cysteamine may be attributable to the mixed disulfide of cystine and cysteamine only possessing 1 mol of cysteine per mole of disulfide, reducing cysteine delivery by 50 %, and not delivering directly to the mTOR locus as functional cystinosin does.
Elements in cystinosis cell pathology attributable to constitutively active mTOR include AKT, protein kinase C, insulin growth factor receptor (IGF-1R), 4E binding protein 1 (4E-BP1), ribosomal protein S6 kinase (S6K), transcription factor EB (TFEB), sterol-responsive element-binding proteins (SREBPs), Lipin-1, and Unc-51-like autophagy activating kinases. mTOR signaling plays a major role in regulating many critical factors including translation, lipid synthesis, nucleotide synthesis, biogenesis of lysosomes, nutrient sensing, and growth factor signaling [7]. This wide-ranging aberrant cell physiology encompasses much of the cystinosis phenotype (Table 3).Table 3. Elements in cystinosis cell pathology attributable to constitutive mTOR malfunction.Table 3. Loss of cell specialization• Create Renal Fanconi SyndromeIncreased apoptosisIncreased autophagyAberrant intermediate metabolism• Lipid synthesis (cholesterol)• Nucleotide synthesis• Biogenesis of lysosomes• Nutrient sensing• Growth factor signalingAberrant osteocyte developmentFailure of proximal renal tubule cells to reabsorb small molecules
Hyperactive apoptosis has been reported in nephropathic cystinosis cells since first described by Thoene in fibroblasts in 2002 [16] and subsequently found to affect proximal renal tubule cells [17]. It was also suggested to be associated with phenotype development [18]. Initially, increased apoptosis in cystinotic cells was attributed to increased activity of PKC∂ after cysteinylation from cystine released from lysosomes [17]. Increased apoptotic activity was found to be associated with AMP kinase [19].
Autophagy is also increased in cystinotic cells [20,21], resulting from mTOR response to the erroneous assessment of starvation state in which cells revert to lysosomal degradation of endogenous proteins, particularly mitochondria, to provide a supply of free amino acids to allow continuation of protein synthesis [7,11].
Taurine
2
Taurine (2-aminoethanesulfonic acid), is a zwitterion non-protein forming, non-carboxy amino acid which is synthesized from cysteamine, methionine, and cysteine, (Fig. 1) and is classified as generally recognized as safe by the US FDA and sold in health food stores both in the USA and Europe. Taurine is the most abundant amino acid in mammalian tissue, with significant effects on ion regulation, osmoregulation and cell development [22].Fig. 1. Metabolic source of taurine, and abnormalities taurine has been shown to correct in vitro and in vivo (see Table 3).Abbreviations: Mt - mitochondrial. ROS - Reactive oxygen species. RTE - renal tubule epithelial cells. Tau(T) - Taurine transporter. CSAD - cysteine sulfinic acid decarboxylase.Fig. 1
A review of the abnormal elements in cystinosis shows that many of them may be correctable by taurine. A wide variety of cells, tissues and cell pathways in which taurine acts to alleviate these abnormalities are known [[23], [24], [25], [26], [27], [28], [29], [30], [31], [32], [33], [34], [35], [36], [37], [38], [39], [40], [41], [42], [43], [44]] (Table 4). Studies in 13 out of 14 cell or tissue types showed taurine decreased, inhibited, or ameliorated apoptosis. In one, free taurine did not decrease apoptosis, but apoptosis increased when the taurine transporter Tau(T) was knocked out [31]. Taurine suppressed or attenuated increased autophagocytosis in three studies in 3 cell types [[37], [38], [39]]. Other factors improved by taurine include deficient myoblasts [40,41], vascular calcification [42], male infertility [43], and obesity [44] (Fig. 1).Table 4. Summary of Taurine Correction of Aberrant Cell Physiology.Table 4. Aberrant physiologyPathway EffectedTissue studiedEffect of TaurineReferenceIncreased apoptosisAKT pathwayDiabetic rat kidneyAmeliorate apoptosis[23]Decreases upregulated Bax and FasStreptozotocin treated pancreatic islandReduced apoptosis[24]Decreased mt permeabilityHypoxic rat retinal ganglion cellReduced apoptosis[25]CaspasesJurkat T-lymphocytesInhibit DNA fragmentation[26]Tau(T)Retinal glial cellsReduced apoptosis[27]FasLIL 2 stressed Anti-CD3-activatedJurkat cellsReduced apoptosis Downregulation of FasL protein[28]Reduced p53 content, and enhanced cellular Bcl-2 content.Ischemic neonatal mouse cardiomyocytesresistant to ischemia-induced necrosis and apoptosis.[29]Prevention of apoptosome formationIschemia in CardiomyocytesInhibits apoptosis.[30]caspase-3 activityCisplatin Erlich ascites cellsNo effect of free taurine supplement KO Tau(T) increases apoptosis[31]Reduction in caspase-8 and caspase-9 expressionIschemic mouse supraoptic and paraventricular nucleiReduces apoptosis[32]ROS inhibition and [Ca2+]i stabilizationGlucose exposure to human umbilical vein endothelial cellsReduces apoptosis[33]Prevents p53 activity, ROS generation and Ca2+ mobilizationDoxorubicin exposed rat testisReduces apoptosis[34]decreased the expression of ER stress-activated glucose regulatory protein 78, C/EBP homologous protein and caspase-12.nucleus pulposus cellsAttenuates apoptosis[35]Decreased ROSHuman renal tubules treated with 30 mM glucoseprevents apoptosis[36]Increased autophagocytosisAkt/mTORCa Oxalate exposed renal tubule cellsSuppresses autophagy[37]LC3-IIOTA-exposed PK 15 cellsAttenuated autophagy[38]Attenuates via mTOR pathwayMeth treated PC12 cellsAttenuates autophagy[39]Deficient myoblastsPI3K-ARID4B-mTOR pathwayC2C12 myoblast cellsPromotes proliferation of myoblast cells**[40]Phosphorylated (p-)AKT–p-mTORMuscle tissuePromotes protein synthesis and restoration of functional and structural phenotypes[41]Vascular calcificationmTORC1 activity and endoplasmic reticulum stress-unfolded protein response in uremic vascular calcification.MiceShort-term treatment of CKD mice with rapamycin, an inhibitor of mTORC1, or tauroursodeoxycholic acid, a bile acid that restores ER homeostasis, normalized mTORC1 activity, molecular markers of UPR, and calcium content of aortas.[42]Male infertilityMultipleMultipletaurine can promote the endocrine function of the hypothalamus-pituitary-testis (HPT) axis, testicular tissue development, spermatogenesis and maturation, delay the aging of testicular structure and function, maintain the homeostasis of the testicular environment, and enhance sexual ability[43]ObesityMultipleMultipleSynthetic activity and concentration of taurine in adipose tissues and plasma have been shown to decrease in humans and animals during the development of obesity, suggesting a relationship between taurine deficiency and obesity[44]**
Surprisingly, patients with cystinosis not on cysteamine have significantly lower plasma taurine (5.2 ± 3.2 μM) than either cysteamine-treated cystinosis patients (25.1 ± 5.0 μM) or normal controls (109.7 ± 11.8 μM) (Mean ± SE) [45]. In this study the patients included 14 non-cysteamine treated patients with a mean age of 1.04 years, 19 cysteamine-treated patients with mean age of 3.5 years, and 30 normal controls with mean age of 1.44 years.
Why should cystinosis patients have low plasma taurine? The answer is two-fold:
- 1)Cysteine is the substrate for cysteine sulfinic acid decarboxylase (CSAD), the rate limiting step in taurine synthesis, and the major endogenous source of taurine. Cysteine availability is significantly limited by the defect in cystinosin that precludes delivery of cystine to the cytosol where it is reduced to cysteine and supplies mTOR and CSAD with cysteine [46]. Knockout (KO) mice lacking CSAD have significantly lower taurine concentrations than wild type controls, having a 90 % reduction in hepatic taurine, and 70 % reduction in renal taurine. [47].
- 2)The Fanconi Syndrome wastes small molecules including aminoacids which are usually retained by the renal proximal tubules, further decreasing the availability of taurine [1].
Although cysteamine therapy raises urinary taurine somewhat [2], it has minimal effect on the renal Fanconi Syndrome, or other phenotypic elements in Table 3. Importantly, supplementation of taurine in the diets of the CSAD (CSD) KO mice normalized solid organ taurine concentration in two to four months [47].
It was recently shown that taurine declines with age in species as diverse as C.
elegans, mice, monkey and man, and taurine supplementation increased the life span of worms, mice, and the health span of aged female mice. Taurine reduced age associated bodyweight gain, improved bone mass in female mice, increased muscle endurance, coordination, and strength [48]. Many elements of the cystinotic phenotype are consistent with premature aging. Premature aging of skin in cystinosis patients has been documented via optical coherence tomography [49]. Bone abnormalities, different than vitamin D responsive rickets [50], male hypogonadism, swallowing abnormalities, vascular calcifications, diabetes, and hypercholesterolemia all occur in cystinosis with a mean age of ∼26 years [6].
In addition to other tissues affected by taurine, the eye has been found to have altered metabolism in ocular tissues [51]. Studies have shown that the retina produces taurine, and CSAD is present in all retinal layers [52]. The salt and pepper retinopathy in cystinosis eyes is one of the first clinical manifestations to appear [1] and is not universally responsive to systemic cysteamine [53]. This retinopathy may be the result of taurine deficiency.
Cystinosis patients have been managed with cysteamine and small molecule replacement but cysteamine's deficiencies, as described above, are a major hindrance to their quality of life. Taurine is benign and may possess the ability to correct these deficiencies. As noted, addition of taurine to the diet of taurine deficient mice raised the taurine content in solid organs to normal in two to four months, supporting the idea that oral taurine will reach the kidneys and other solid organs in cystinotic patients. Since taurine corrects many of the phenotypic abnormalities found in other conditions which occur in cystinosis it appears reasonable to determine its validity via preliminary in vitro and animal studies and a well-controlled clinical trial.
CRediT authorship contribution statement
Jess G. Thoene: Writing – review & editing, Writing – original draft, Conceptualization.
Declaration of Generative AI and AI-assisted technologies in the writing process
During the preparation of this work the author(s) used [Chat GPT04] in order to produce the figure. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Declaration of competing interest
I received no financial support for this work.
I am the inventor of a patent owned by the University of Michigan covering this use of taurine.
I did not use AI in the preparation of this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gahl WA, Thoene J G. Cystinosis: a disorder of, lysosomal membrane transport. In: Valle DL, Antonarakis Ballabio A, Beaudet AL, Mitchell GA. Online Metabolic and Molecular Bases of Inherited Disease S, https://ommbid.mhmedical.com.
- 2Thoene J.Oshima R.Crawhall J.Olson D.Schneider J.Cystinosis: intracellular cystine depletion by aminothiols in vitro and in vivo J. Clin. Invest.58197618018993220510.1172/JCI 108448 PMC 333169 · doi ↗ · pubmed ↗
- 3Gahl W.A.Reed G.F.Thoene J.G.Schulman J.D.Rizzo W.B.Jonas A.J.Denman D.W.Schlesselman J.J.Corden B.J.Schneider J.A.Cysteamine therapy for children with nephropathic cystinosis N. Engl. J. Med.31616198797197710.1056/NEJM 198704163161602 Apr 16. (PMID: 3550461)3550461 · doi ↗ · pubmed ↗
- 4Pisoni R.L.Thoene J.G.Christensen H.N.Detection and characterization of carriermediated cationic amino acid transport in lysosomes of normal and cystinotic human fibroblasts. Role in therapeutic cystine removal?J Biol Chem 2608198547918 Apr 25. PMID: 39215383921538 · pubmed ↗
- 5Cherqui S.Courtoy P.J.The renal Fanconi syndrome in cystinosis: pathogenic insights and therapeutic perspectives Nat Rev Nephrol 1322017 Feb 11513110.1038/nrneph.2016.182Epub 2016 Dec 19. PMID: 27990015; PMCID: PMC 565749027990015 PMC 5657490 · doi ↗ · pubmed ↗
- 6Gahl W.A.Balog J.Z.Kleta R.Nephropathic cystinosis in adults: natural history and effects of oral cysteamine therapy Ann. Intern. Med.1474200724225010.7326/0003-4819-147-4-200708210-00006 Aug 21. (PMID: 17709758)17709758 · doi ↗ · pubmed ↗
- 7Panwar V.Singh A.Bhatt M.Tonk R.K.Azizov S.Raza A.S.Sengupta S.Kumar D.Garg M.Multifaceted role of m TOR (mammalian target of rapamycin) signaling pathway in human health and disease Signal Transduct. Target. Ther.81202337510.1038/s 41392-023-01608-z Oct 2. (PMID: 37779156; PMCID: PMC 10543444)37779156 PMC 10543444 · doi ↗ · pubmed ↗
- 8Kim Y.C.Guan K.L.m TOR: a pharmacologic target for autophagy regulation J Clin Invest 12512015 Jan 253210.1172/JCI 73939 Epub 2015 Jan 2. PMID: 25654547; PMCID: PMC 438226525654547 PMC 4382265 · doi ↗ · pubmed ↗