Association between inflammatory biomarkers and the cognitive response to a multidomain intervention: secondary longitudinal analyses from the MAPT study
Emmanuel Gonzalez-Bautista, Maria Soto, Gabor Abellan van Kan, Julien Delrieu

TL;DR
This study found that higher levels of certain inflammatory biomarkers are linked to worse cognitive outcomes in older adults receiving a multidomain intervention for Alzheimer's prevention.
Contribution
The study identifies specific inflammatory biomarkers associated with cognitive response to a multidomain Alzheimer's intervention.
Findings
Higher GDF15 and TNFR1 levels were linked to worse cognitive function over two years.
Higher IL6 and CRP levels reduced the likelihood of being a 'good responder' to the intervention.
Inflammation levels predicted cognitive outcomes in participants receiving the multidomain intervention.
Abstract
The aim of this study is to evaluate the association of systemic inflammation measured by plasma biomarkers with the change in cognitive function among participants from the Multidomain Alzheimer Preventive Trial (MAPT) exposed to the multidomain intervention (MI). Secondary analysis of the MAPT longitudinal data. MAPT is a randomized, placebo-controlled trial with 3 interventional groups (omega-3 only, MI only, omega-3 plus MI) and a control group. We tested the association of the change in cognitive function with inflammatory biomarkers (tumoral necrosis factor receptor-1 (TNFR1), monocyte chemoattractant protein-1 (MCP1), Growth Differentiation Factor-15 (GDF15), Interleukin-6 (IL6) and C reactive protein (CRP)) using mixed-effects models. A subgroup analysis was performed in those exposed to the MI. The response to the MI was defined as the change in the composite cognitive score…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
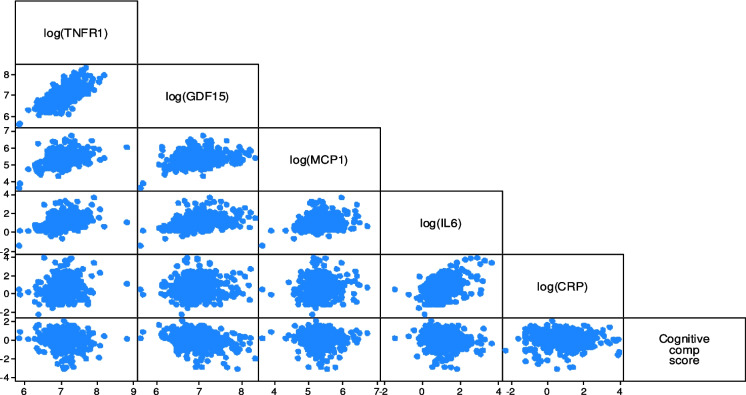 Figure 1
Figure 1- —Université Toulouse III - Paul Sabatier
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Dementia and Cognitive Impairment Research · Neuroinflammation and Neurodegeneration Mechanisms
Background
Multidomain interventions (MI) are strategies aimed at improving older people’s function or delaying its decline, and they involve at least two of the following: cognitive training, physical exercise, nutrition, or psychosocial components [1]. MI targeted to enhance cognitive capacity and slow cognitive decline has produced mixed results. A recent Cochrane review concluded that some features are repeatedly found in trials with positive results. (A) Endpoint measurement: there is a high certainty of evidence (GRADE) that MI provides a small but significative benefit against cognitive decline when measured with a neuropsychological test battery and compared to usual care/placebo (mean difference of a z-score = 0.03 SD higher in the MI group than in placebo or usual care) [2]. (B) Inclusion of cognitive training: it is associated with a positive effect, yet its impact on day-to-day functioning is arguable because participants might be just training on responding to the tests without any clinical relevance.
However, there is scarce information on how to target people with high chances of displaying a good response to MI preventing Alzheimer’s disease (AD) and cognitive decline trials. Older age, family history of AD, and mild cognitive impairment have been pointed out as features of participants at higher risk than the overall population, and thus, hypothetically having higher chances of being impacted by interventions [1, 3, 4]. Other studies have also included AD low-grade inflammation-related risk factors (e.g., cardiovascular risk factors like high blood pressure and HbA1c levels) among the inclusion criteria [1, 5]. Factors scores have been developed like the Cardiovascular Risk Factors, Aging and Dementia (CAIDE) [6] and Dementia Assessment Sheet for Community-based Integrated Care System 21-items (DASC-21), which include variables like age, level of education and hypertension, hypercholesterolemia, and obesity. MI studies have also found sub-group effects, for instance, in people with severe white matter hyperintensities [7]. Likewise, responses have been found among ApoE4 carriers [8].
Inflammatory cytokines are linked to cognition through a dual mechanism, wherein systemic cytokines signal the central nervous system (CNS) inflammation, and the systemic consequences of those cytokines ultimately affect cognition [9]. Cognitive manifestations of inflammatory damage appear when chronic excessive exposure to cytokines surpasses the functional cognitive reserve [9]. When activated, proinflammatory microglia can hinder the survival and growth of new cells and impact their integration into existing neural networks [10]. While neuroinflammation is strongly associated with cognitive impairments, there are still gaps in understanding the role of peripheral inflammation. However, peripheral cytokines can communicate with the central nervous system by stimulating vagal afferent nerves or brain vascular endothelial cells to produce proinflammatory cytokines, leading to symptoms such as impaired memory. In particular, systemic inflammation, vascular inflammation, and altered endothelial function may contribute to specific cognitive decline in individuals without dementia. Systemic inflammation, a risk factor for cardiovascular disease, can cross the blood–brain barrier and lead to responses causing neurodegeneration and cognitive impairment [11], for instance, IL-6, a marker of systemic inflammation, has been associated with cognitive decline and changes in brain structure[12].
A recent systematic review with metanalyses found that IL6 is among the most studied cytokines, with higher IL6 concentrations in AD patients compared to controls and in mild cognitive impairment (MCI) subjects compared to controls [9], and similar findings for TNFR-1 levels. Our group recently reported that the MI of Multidomain Alzheimer Preventive Trial (MAPT) positively improved cognition trajectories in participants with positive amyloid status defined by PET [10] or plasma Aβ 42/40 levels. [13] Further implication of inflammatory biomarkers has not been explored. The mechanisms by which multidomain interventions have improved cognitive decline are hypothesized to pass by stimulating cognition, nutrition, and locomotion and reducing risk factors; however, the molecular mechanisms are yet to be explored [1].
Characterizing inflammation levels in non-demented populations exposed to AD-prevention MI could help to select the best target population and increase the efficiency of the MI [14]. Thus, our objective was to evaluate the association of systemic inflammation measured by plasma biomarkers with the change in cognitive function among participants from the Multidomain Alzheimer Preventive Trial (MAPT) exposed to the multidomain intervention (MI).
Methods
Study
This is a secondary analysis of the MAPT study. The detailed methodology of MAPT has been described elsewhere [15, 16]. In summary, MAPT was a randomized controlled trial (RCT) testing the effect of a MI (nutritional counseling, physical exercise, and cognitive stimulation) with and without supplementation of omega-3 polyunsaturated fatty acids (omega-3) versus usual care on the prevention of cognitive decline among community-dwelling adults aged 70 years and older recruited in memory clinics in France. The Ethical Committee (CPP SOOM II) based in Toulouse approved the study (ClinicalTrials.gov identifier: NCT00672685). All participants signed a consent form before the study assessments. One blood sample of 15 ml (10 ml in an EDTA vacutainer and two 2.5 ml in PAXgene RNA tubes) was collected yearly for MAPT biobank. These samples were transferred directly at ambient temperature to the Cellular Biology and Cytology Laboratory at each site. The two PAXgene RNA tubes were frozen at − 20° directly. The EDTA tube was centrifuged then aliquoted; the serum and the pellet were collected in two 5-ml dry tubes, and then frozen at − 20°.
Participants
MAPT inclusion criteria were meeting at least one of (a) spontaneous memory complaint expressed to their physician, (b) limitation in one instrumental activity of daily living (IADL), or (c) slow gait speed (≤ 0.8 m/s). Exclusion criteria comprised (a) participants with a Mini-Mental State Examination (MMSE) score < 24, (b) diagnosis of dementia, (c) limitation for one or more basic activities of daily living (ADLs), and (d) those taking omega-3 supplements at baseline. The selection of participants based on functional status was determined to target people with at least some degree of functional limitation (IADLs), hens with room to make improvements, but not yet touched in their ADLs, as this would be a proxy for care dependency [17].
The MI consisted of 2-h group sessions focusing on three domains (cognitive stimulation, physical activity, and nutrition) and a preventive consultation (at baseline, 12 months, and 24 months) with a physician to optimize management of cardiovascular risk factors and detect functional impairments [18]. Twelve small group sessions of the multidomain intervention were done in the first 2 months of the trial (two sessions per week in the first month, and one session per week in the second). Each session included 60 min of cognitive training (reasoning and memory training), 45 min of advice about and demonstrations of physical activity encouraging participants to increase their physical activity in their daily life to the equivalent of at least 30 min walking per day, 5 days a week, and was provided with a home-based program designed during individual interviews), and 15 min of nutritional advice based on French National guidelines. For the remainder of the 3-year study, participants in the multidomain intervention groups attended a 1-h session each month and two 2-h reinforcement sessions (12 and 24 months).
From the original 1679 participants enrolled in MAPT, we included participants with at least two available cognitive composite score measures and biomarker data (Supplementary Fig. 1). We defined the analytic start of our study by the time of the biomarker sampling (12 months after the MAPT study baseline) and worked with data for the rest of the intervention period. Sociodemographic and clinical data of interest for this study was collected at 12, 24, and 36 months after MAPT started.
Composite cognitive score
The MAPT study used a cognitive composite score resulting from the z scores (using baseline means and standard deviations) of free and cued selective reminding test (FCSRT – free + total) for episodic memory [19], MMSE for orientation [20], Digit Symbol Substitution Subtest (DSST from Wechsler Adult Intelligence Scale-Revised) for attention and executive function [21], and Category Fluency Test for verbal fluency measured yearly within our study period. The MAPT composite score, similar to other indices of this kind, was derived from cohort studies in “normal controls” who progressed to mild cognitive impairment or Alzheimer dementia. Those studies determined that a composite measure sensitive to change in preclinical AD would likely require assessment of 3 key domains: episodic memory, executive function, and orientation [22]. The use of cognitive composite scores is supported by theoretical and empirical validations [23–25], and has been accepted by the FDA as a primary outcome in randomized clinical trials [26].
Change in the cognitive composite score
First, using data from the overall MAPT population, we assessed the association of the change in the cognitive composite score and the plasma biomarkers adjusting for the MAPT allocation group (4 groups) in stepwise models.
Response to the multidomain intervention
Secondly, we worked with the 531 participants randomized to the MI groups (with or without omega-3 supplementation).
We used two alternative definitions of the MI cognitive response: (i) those in the 5th quintile of change in the composite score in 2 years (20% best responders—this group can include people with a mild absolute negative change in the cognitive score) and (ii) participants with a change in cognitive composite score > 0 (only those with an improvement of the cognitive score over time).
Inflammatory biomarkers
Plasma biomarkers selected as surrogates of peripheral inflammation were: IL6 [27, 28], TNFR1, MCP1 [29], GDF15, and CRP [30, 31]. Sample processing is described thoroughly in the supplementary material 1. All biomarker concentrations were measured in pg/mL except for CRP (mg/L) and were log transformed.
Covariates
Models were adjusted for age, sex, education, apoE4 status (carrier versus non-carrier), clinical dementia rating (CDR) global score, MAPT allocation group (MI only or MI plus omega-3 supplementation) and intervention adherence (percentage of sessions attended) at baseline. Plasma Aβ 42/40 ratio was used as a covariate in the sensitivity analyses because it was only available on a subsample (n = 241).
Statistical analyses
We used means and standard deviations (SD) to describe continuous variables and frequencies and percentages for categorical/binary variables. We explored the distribution of the biomarkers and the cognitive response using scatterplots **(**Fig. 1).Fig. 1. Graphical distribution of the baseline inflammation biomarkers and the cognitive composite score change during the study period. The scatterplots of the bottom line correspond to the unadjusted modeled associations in Table 2, which have the cognitive composite score in the y-axis and the biomarker log levels in the x-axis
We ran linear mixed models with a random intercept at the individual level to estimate the association of the biomarker levels with the change in the cognitive composite score over time: (A) adjusted for sex, age, and MAPT group (using the no-MI group as a reference), (B) adjusted for A + education, CDR score, ApoE4 status, and (C) B + plasma Aβ 42/40 ratio. These models take into account the individual-level variance, which adjusts for the starting cognitive score [32].
Operational definitions of the MI cognitive response
(i) We predicted the individual trajectory of cognitive score over the study period (24 months) using mixed models for the time variable with random intercepts at the participant level and random slope for time (“empty model”). Then, we divided the slope of such trajectories into quantiles, the fifth quintile identifying the 20% best-off responders (steeper slope for composite cognitive score change over time). We coded a binary variable with “good responders (Q5)” = 1 and “other participants (Q1–Q4)” = 0. We ran logit models with this binary variable as the dependent and predictors as in models A, B, and C.
(ii) We used an alternative definition for “good responders”, including only the participants with a change in cognitive composite score > 0 (meaning their cognitive score improved over time) for our study period.
All analyses were evaluated at α = 0.05 and were performed using Stata 18. Stata Corp. 2023. College Station, TX: StataCorp LLC.
Results
We included 1527 participants with at least two cognitive measures. Their mean age was 75.3 (standard deviation, SD = 4.3), and 64% were female. About 1 out of 4 participants (23.3%) were ApoE4 carriers (Table 1). Among those, 1089 had biomarker data available. The cognitive composite score showed a statistically significant monthly decrease of 0.0048 (95% CI − 0.0091; − 0.0005) per each log unit of TNFR1, and a statistically significant monthly decrease of 0.0049 (95% CI − 0.0085; − 0.0013) per each log unit of GDF-15, adjusting for age, sex, MAPT allocation group, education level, CDR score, and ApoE4 status. (Model B Table 2). The association of the cognitive composite score with the other biomarkers was not statistically significant. Adjusting for plasma Ab 42/40 ratio rendered the associations non-significant (n = 382). Table 1. Description of the study populationNot exposed to multidomain intervention expoExposed to multidomain interventionOverallParticipants with a cognitive change in Q1-Q4Participants with a cognitive change in Q5 “good responders”N842 (55.1%)548 (35.9%)137 (9.0%)1527 (100.0%)Age75.4 (4.514)75.5 (4.309)73.9 (3.796)75.3 (4.400)SexFemale548 (65.1%)338 (61.7%)92 (67.2%)978 (64.0%)Male294 (34.9%)210 (38.3%)45 (32.8%)549 (36.0%)Cognitive composite score0.137 (0.771)0.103 (0.761)0.314 (0.750)0.141 (0.767)CDR0372 (53.4%)255 (47.4%)80 (58.8%)707 (51.6%)0.5321 (46.1%)282 (52.4%)55 (40.4%)658 (48.0%)14 (0.6%)1 (0.2%)1 (0.7%)6 (0.4%)Education < 12 years459 (56.4%)314 (57.8%)66 (48.5%)839 (56.2%) ≥ 12 years355 (43.6%)229 (42.2%)70 (51.5%)654 (43.8%)ApoE4 carrierNo506 (77.6%)351 (75.6%)92 (76.0%)949 (76.7%)Yes146 (22.4%)113 (24.4%)29 (24.0%)288 (23.3%)BMI26.3 (3.9)26.4 (4.2)25.7 (3.8)26.3 (4.0)MMSE (/40)28.0 (1.9)28.1 (1.8)28.2 (1.7)28.0 (1.9)FrailtyRobust316 (51.0%)256 (53.2%)74 (62.2%)646 (53.0%)Pre_frail281 (45.3%)211 (43.9%)44 (37.0%)536 (43.9%)Frail23 (3.7%)14 (2.9%)1 (0.8%)38 (3.1%)Inflammatory biomarkersTNFR11222.5 (415.6)1253.5 (486.6)1117.7(337.7)1223.7 (439.1)GDF151120.7 (510.1)1164.7 (532.7)992.8 (384.0)1124.5 (509.6)MCP1221.6 (86.4)223.1 (87.7)220.1 (84.8)222.1 (86.7)IL64.3 (17.0)3.5 (3.2)3.5 (4.5)3.9 (12.3)CRP [mg/L]0.45 (1.7)0.32 (1.4)0.16 (0.8)0.37 (1.5)BMI body mass index, MVPA moderate-to-vigorous intensity physical activity, MET metabolic equivalent task, ApoE4 Apolipoprotein E4, IL6 Interleukin-6, TNFR1 tumoral necrosis factor receptor-1, MCP1 monocyte chemoattractant protein-1, GDF15 Growth Differentiation Factor-15, CRP C reactive protein^^Unit [pg/mL]Table 2. Mixed effect models for the change in cognitive composite score (continuous variable) in the overall MAPT populationModel AModel BModel CAge, sex and MAPT groupA + education, CDR, ApoE4B + plasma Ab 42/40 ratioCoeffpCI95%lbCI95%ubCoeffpCI95%lbCI95%ubCoeffpCI95%lbCI95%ubn*1089968382TNFR1 − 0.00450.033 − 0.0086** − 0.0004**** − 0.00480.0280 − 0.0091**** − 0.0005**** − 0.00670.0930 − 0.01450.0011GDF15 − 0.00490.005 − 0.0083**** − 0.0015**** − 0.00490.0070 − 0.0085**** − 0.0013**** − 0.00560.1070 − 0.01240.0012MCP1 − 0.00050.789 − 0.00430.0033 − 0.00070.7160 − 0.00480.0033 − 0.00100.8070 − 0.00890.0069IL60.00050.657 − 0.00160.00250.00030.7650 − 0.00180.0025 − 0.00260.2140 − 0.00670.0015CRP0.00020.927 − 0.00480.00530.00190.5290 − 0.00390.00770.00310.5100 − **0.00620.0124Coeff. = the estimated change in the cognitive composite score by per month, by each increase in one unit of the log transformed biomarkerApoE4 Apolipoprotein E4, IL6 Interleukin-6, TNFR1 tumoral necrosis factor receptor-1, MCP1 monocyte chemoattractant protein-1, GDF15 Growth Differentiation Factor-15, CRP C reactive proteinStatistically significant results are marked in bold
MAPT participants exposed to the MI
Among MAPT participants exposed to the MI (with or without omega-3 supplementation), “good responders” were younger and had better CDR scores than their counterparts at baseline (Table 1). They had an estimated mean change in the composite score of 0.051 (SD 0.062) over 2 years of intervention, compared to − 0.136 (SD = 0.111) for the not-good responders.
For each log unit increase in GDF-15, the cognitive composite score decreased significantly 0.0053 (95% CI − 0.0105; − 0.0002) points monthly, adjusting for age, sex, education, CDR score, ApoE status, MAPT allocation group, and adherence to the MI (Table 3 Model B). No other significant associations were found for models A and B. Among participants with available data for plasma Ab 42/40 ratio (n = 187), a significant decrease in the cognitive composite score was found for each log unit increase in TNFR1 (− 0.0157, 95% CI − 0.0279; − 0.0034) and also for GDF-15 (− 0.0116, 95% CI − 0.0215; − 0.0016) (Table 3 Model C). Table 3. Mixed effect models for the change in cognitive composite score (continuous variable) in participants exposed to the MIModel AModel BModel CAge and sexA + education, CDR, ApoE4, MAPT group and adherenceB + plasma Aβ 42/40 ratioCoeffpCI95%lbCI95%ubCoeffpCI95%lbCI95%ubCoeffpCI95%lbCI95%ubn531478187TNFR1 − 0.00430.180 − 0.01050.0020 − 0.00600.068 − 0.01240.0004** − 0.01570.012 − 0.0279**** − 0.0034GDF15 − 0.00390.121 − 0.00890.0010 − 0.00530.042 − 0.0105**** − 0.0002**** − 0.01160.022 − 0.0215**** − 0.0016**MCP10.00080.772 − 0.00460.00630.00040.883 − 0.00530.0062 − 0.00500.417 − 0.01720.0071IL60.00180.249 − 0.00130.00480.00150.362 − 0.00170.0047 − 0.00480.174 − 0.01170.0021CRP0.00090.359 − 0.00100.00280.00080.430 − 0.00120.0028 − 0.00070.679 − 0.00420.0027Coeff. = the estimated change in the cognitive composite score by per month, by each increase in one unit of the log transformed biomarkerApoE4 Apolipoprotein E4, IL6 Interleukin-6, TNFR1 tumoral necrosis factor receptor-1, MCP1 monocyte chemoattractant protein-1, GDF15 Growth Differentiation Factor-15, CRP C reactive proteinStatistically significant results are marked in bold
Odds of being in the good responder group (logit models)
Higher plasma levels of GDF15 and TNFR1 were significantly associated with lower chances of being in the cognitive “good responder” group when adjusting for age and sex. However, this association remained significant only for TNFR1 after adjusting for education, CDR baseline status, ApoE4, MAPT group, and adherence. For each log increase in TNFR1, the odds of being in the “good responder” group lowered by 59% (OR = 0.41, 95% CI 0.18; 0.94) (Table 4). In other words, for each increase in one log unit of the TNFR1, the odds of being in the “good responder” group decreased by 34% compared to those in the non-good responders’ group. Table 4. Logit models for the odds of being in the “good responders” group compared to being in the “other participants”Model AModel BModel CAge and sexA + education, CDR, ApoE4, MAPT group and adherenceB + plasma Aβ 42/40 ratioORpCI95%lbCI95%ubORpCI95%lbCI95%ubORpCI95%lbCI95%ubn531478187TNFR10.440.0310.200.930.410.0360.180.940.360.3120.052.61GDF150.490.0330.260.940.550.1100.271.140.730.7340.114.62MCP11.100.7670.592.031.120.7490.572.211.050.9480.244.55IL60.950.7720.671.351.010.9780.681.490.220.0180.060.78CRP0.970.7980.791.200.980.8610.771.240.480.0090.280.84OR = the odds ratio of being in the “good responders” group compared to being among the “no good responders” per each increase in one unit of the log transformed biomarkerApoE Apolipoprotein E, IL6 Interleukin-6, TNFR1 tumoral necrosis factor receptor-1, MCP1 monocyte chemoattractant protein-1, GDF15 Growth Differentiation Factor-15, CRP C reactive protein
Similar results were found with the second definition of good responders (absolute positive change in the composite score over time). In the model adjusted for age, sex, education, CDR, ApoE4, MAPT group, and adherence (n = 478), the possibility of being a good responder was OR = 0.41, 95% CI 0.18 for each unit increase in the log transformed TNFR1 (Supplementary Table S1).
Participants with higher IL6 or CRP levels showed significantly lower odds of being in the “good responder” group (Model C Table 4). For each log increase in IL6 levels, the odds of being in the “good responder” group decreased by 78% (OR = 0.22, p = 0.018, 95% CI 0.06; 0.78), likewise, those odds decreased by 52% for each log increase in CRP (OR = 0.48, p = 0.009, 95% CI 0.28; 0.84). No association was found for MCP1.
Discussion
The levels of inflammatory plasma biomarkers (TNFR1 and GDF15) were inversely and significantly associated with the change in cognitive function within 2 years of the second cognitive measure in MAPT participants. Among those exposed to the MI, this association was independent from the participants’ level of plasma Aβ 42/40 ratio and ApoE4 status. Moreover, participants who showed a good response to the MI (i.e., the 20% best-off of change in cognitive function), registered low peripheral inflammation biomarkers (TNFR1, GDF15, IL6, and CRP) within 2 years of the second cognitive measure, independently from their Aβ 42/40 ratio levels and ApoE4 status. When adjusting for plasma amyloid levels, higher IL6 and CRP plasma levels were significantly associated with lower odds of being in the “good responder” group.
The impact of MI on global cognition has been inconclusive so far [33]. Meta-analyses indicate that multidomain interventions have small but significant effects on reducing dementia risk and improving cognitive composite scores, although effects on global cognition remain inconclusive [34]. Large RCTs have found negative primary outcome results, but some significant findings when looking at participants with higher dementia risk [7, 18].
To our knowledge, this is the first study to identify peripheral inflammation associated with a good MI response in nondemented older adults with memory complaints.
Previous works have identified a positive response to MI among ApoE4 carriers and positive amyloid participants [13, 35]. These two biomarkers are related to the AD pathophysiology. They thus might indicate the impact of MI as secondary prevention in people who are at risk for developing AD or at an early symptomatic stage of the disease. However, according to our results, we think that MI might also exert an effect on cognitive function in non-AD patients with memory complaint afflicted by other cognitive deteriorations related to aging and inflammation. In other words, by selecting participants with low inflammatory markers, clinical trials, and population-based interventions could open their scope to the primary prevention of cognitive decline for both AD and non-AD patients without systemic inflammation. As can be seen in Supplementary Figure S2, plasma levels of GDF15, IL6, and CRP are consistently low in “good responders”, regardless of their amyloid status.
The association between systemic inflammation and cognitive decline has been studied during the last two decades. This link has been found in middle-aged [36] and older subjects [37]. In AD pathogenesis, inflammation has been suggested to play a role in amyloid brain deposition [38]. Put another way, finding low inflammatory levels in people with memory complaints might be a marker of good cognitive reserve [9] or a “fertile field” to receive an MI. A complex cross-talk between the immune and neurological systems involves cytokines as modulators of the neuronal and glial cell function in neuronal regeneration or neurodegeneration [39].
Our study has strengths. We have used data from a clinical trial, which allows for a thorough measurement of the clinical outcome after a standardized exposure and adjusting by adherence to the intervention. Additionally, we were able to control for the effect of previously explored variables related to the outcome, like ApoE4 and amyloid status. This allowed us to bridge further the knowledge gap on factors associated with a MI. Our study had limitations; for instance, we could not describe the trajectory of the inflammatory biomarkers along the intervention because they were measured only once. The biomarker sampling did not coincide with the beginning of the MAPT study but 12 months after, which impeded us from including the complete intervention period (initially 3 years). However, had the biomarker level lowered due to the intervention during the first 12 months, this effect would have reinforced the association we found (lower biomarker levels linked to higher cognitive response). Also, our sample size was affected, given that plasma Aβ 42/40 ratio was only measured in a small subsample of participants.
This study does not allow for detailed evaluation of each intervention individually; particularly, given that the MAPT study was designed as a 1:1:1:1 randomized controlled trial. Furthermore, given that the omega-3 supplementation without MI has not shown a positive effect in older adults’ cognition trajectories, we focused our research question on the response to the MI.
Perspectives
In future studies, we foresee the instrumentation of a biochemical profiling of patients who are candidates for a MI. Using a panel of plasma biomarkers can be an innovative step forward to personalized prevention of cognitive decline. Additionally, AD and neurodegeneration blood biomarkers [40], including inflammation, could be helpful to reach a more efficient population in cognitive decline prevention trials.
Conclusion
“Good responders” to the MAPT MI showed lower GDF15 and TNFR1 baseline blood levels than their counterparts. MAPT participants who increased their cognitive score after 2 years of intervention had lower IL6 and CRP baseline levels, regardless of their Aβ 42/40 and ApoE4 status. More research is needed to describe the trajectories of inflammation along the MI. Also, further trials should explore if inflammation-lowering interventions like physical activity, diet, or anti-inflammatory drugs should be implemented before or concomitantly with cognitive stimulation in MI. Using inflammatory biomarkers as a selection criterion for AD primary preventive trials might lead to a more efficient enrolling process for the research and real-world clinical contexts.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1(DOCX 17.1 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hafdi M, Hoevenaar-Blom MP, Richard E. Multi-domain interventions for the prevention of dementia and cognitive decline. The Cochrane Database Syst Rev. 2021;11:CD 013572. 10.1002/14651858.CD 013572.pub 2.10.1002/14651858.CD 013572.pub 2PMC 857476834748207 · doi ↗ · pubmed ↗
- 2Kumagai R, Osaki T, Oki Y, Murata S, Uchida K, Encho H, Ono R, Kowa H. The Japan-multimodal intervention trial for prevention of dementia PRIME Tamba (J-MINT PRIME Tamba): study protocol of a randomised controlled multi-domain intervention trial. Arch Gerontol Geriatr. 2023;104:104803. 10.1016/j.archger.2022.104803.10.1016/j.archger.2022.10480336088747 · doi ↗ · pubmed ↗
- 3Chi GC, Fitzpatrick AL, Sharma M, Jenny NS, Lopez OL, De Kosky ST. Inflammatory biomarkers predict domain-specific cognitive decline in older adults., The Journals of Gerontology. Series A, Biol Sci Med Sci. 2017;72:796–803. 10.1093/gerona/glw 155.10.1093/gerona/glw 155PMC 586184527522059 · doi ↗ · pubmed ↗
- 4Delrieu J, Vellas B, Guyonnet S, Cantet C, Ovod V, Li Y, Bollinger J, Bateman R, Andrieu S, Carrié I, Brigitte L, Faisant C, Lala F, Villars H, Combrouze E, Badufle C, Zueras A, Morin C, Van Kan GA, Dupuy C, Rolland Y, Caillaud C, Ousset P-J, Willis S, Belleville S, Gilbert B, Fontaine F, Dartigues J-F, Marcet I, Delva F, Foubert A, Cerda S, Marie-Noëlle-Cuffi CC, Rouaud O, Manckoundia P, Quipourt V, Marilier S, Franon E, Bories L, Pader M-L, Basset M-F, Lapoujade B, Faure V, Tong MLY, Malick-Lo · doi ↗ · pubmed ↗
- 5Vermunt L, Muniz-Terrera G, Ter Meulen L, Veal C, Blennow K, Campbell A, Carrié I, Delrieu J, Fauria K, Rodríguez GH, Ingala S, Jenkins N, Molinuevo JL, Ousset P-J, Porteous D, Prins ND, Solomon A, Tom BD, Zetterberg H, Zwan M, Ritchie CW, Scheltens P, Luscan G, Brookes AJ, Visser PJ. Prescreening for European prevention of Alzheimer dementia (EPAD) trial-ready cohort: impact of AD risk factors and recruitment settings. Alzheimer’s Res Ther. 2020;12:8. 10.1186/s 13195-019-0576-y.10.1186/s 13195-01 · doi ↗ · pubmed ↗
- 6Villalobos Dintrans P, González Bautista E. Functional dependency in Mexico: measurement issues and policy challenges. Int J Health Pol Manag. 2020. 10.34172/ijhpm.2020.248.10.34172/ijhpm.2020.248PMC 980816333589566 · doi ↗ · pubmed ↗
- 7Hendrix SB, Soininen H, van Hees AMJ, Ellison N, Visser PJ, Solomon A, Attali A, Blennow K, Kivipelto M, Hartmann T. Alzheimer’s disease composite score: a post-hoc analysis using data from the Lipi Di Diet trial in prodromal Alzheimer’s disease. J Prev Alzheimer’s Disease. 2019;6:232–236. 10.14283/jpad.2019.33.10.14283/jpad.2019.3331686094 · doi ↗ · pubmed ↗
- 8Sims JR, Zimmer JA, Evans CD, Lu M, Ardayfio P, Sparks J, Wessels AM, Shcherbinin S, Wang H, Monkul Nery ES, Collins EC, Solomon P, Salloway S, Apostolova LG, Hansson O, Ritchie C, Brooks DA, Mintun M, Skovronsky DM. Donanemab in early symptomatic alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330:512–527. 10.1001/jama.2023.13239.10.1001/jama.2023.13239 PMC 1035293137459141 · doi ↗ · pubmed ↗