Periportal Paraganglioma: A Rare Cause of Obstructive Jaundice and Gastroesophageal Varices
Irhoboudu D. Atogwe, Lefika Bathobakae, Fnu Deepali, Maria Lagarde Mussa, Olubunmi Shoyele

TL;DR
A rare case of periportal paraganglioma causing jaundice and varices is reported, emphasizing the need to consider this tumor in biliary tract mass diagnoses.
Contribution
The novelty lies in presenting a rare case of nonfunctioning periportal paraganglioma with obstructive jaundice and varices.
Findings
The tumor was nonfunctioning and showed no metastatic disease.
The patient was managed with portal vein stenting after failed laparoscopic resection.
The case underscores the diagnostic challenge of paragangliomas mimicking biliary tract malignancies.
Abstract
Paragangliomas are rare neuroendocrine tumors arising from extra-adrenal chromaffin cells. Biliary tropism is exceptionally rare and can mimic primary biliary tract malignancies, thus presenting a diagnostic challenge. We describe a rare case of periportal paraganglioma presenting with obstructive jaundice and gastric and duodenal varices. Similar to other reported primary hepatic paragangliomas, this tumor was nonfunctioning, and there was no evidence of metastatic disease. The patient underwent portal vein stenting to relieve portal hypertension after failed laparoscopic resection because of high vascularity. He continues to follow-up with our clinic for serial blood tests and imaging and remains asymptomatic. This case highlights the importance of considering paraganglioma in the differential diagnosis of biliary tract masses.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
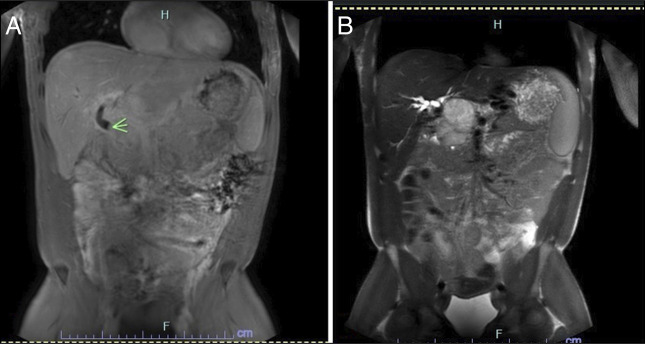 Figure 1
Figure 1 Figure 2
Figure 2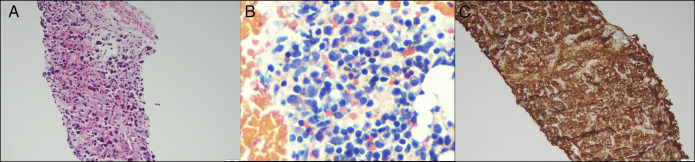 Figure 3
Figure 3| Laboratory parameter | On initial evaluation | After biliary duct stenting | Reference range |
| Alanine transferase | 128 | 37 | 5–40 unit/L |
| Aspartate transferase | 65 | 28 | 9–48 unit/L |
| Alkaline phosphatase | 158 | 91 | 44–121 unit/L |
| Total bilirubin | 1.1 | 0.9 | 0.0–0.3 mg/dL |
| Gamma glutamyl transferase | 221 | — | 8–54 unit/L |
| Platelet count | 137 | — | 150–400 K/uL |
| Total protein | 7.2 | — | 6–8.5 mg/dL |
| International normalized ratio | 1 | — | 0.851–1.14 |
| Serum creatinine | 1.01 | — | 0.5–1.5 mg/dL |
| Albumin | 5.4 | — | 3.4–4.8 g/dL |
| Author(s) | Year | Patient | Clinical presentation | Location | Treatment | Outcome |
| Caceres et al. | 2001 | 28/F | Abdominal pain | Common bile duct | Open cholecystectomy and Roux-en-Y hepaticojejunostomy | Cured with no evidence of tumor recurrence |
| Hitanant et al. | 1984 | 59/M | Obstructive jaundice | Common hepatic duct | Open surgical exploration | Cured with no evidence of tumor recurrence |
| Sarma et al. | 1980 | 37/M | Obstructive jaundice | Hepatic ducts | Exploratory laparotomy | Cured |
| Our case | 2025 | 29/M | Obstructive jaundice | Porta hepatis | Biliary stenting, portal vein stenting after failed resection. Active observation | Currently asymptomatic |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Hormonal Regulation and Hypertension · Pituitary Gland Disorders and Treatments
INTRODUCTION
Paragangliomas are rare neuroendocrine tumors that arise from extra-adrenal paraganglionic tissue.^1–3^ These tumors can be found in various locations throughout the body, most commonly in the head, neck, abdomen, urinary bladder, and para-aortic region.^4^ Biliary paragangliomas are very rare, and only a handful of cases have been reported to date.^5–8^We present an exceptionally rare case of periportal paraganglioma in a 29-year-old man with a history of ankylosing spondylitis. The patient presented with obstructive jaundice and was found to have a nonsecretory extrahepatic paraganglioma on imaging, which was confirmed by core needle biopsy. It is crucial to differentiate biliary tumors from extrahepatic nonfunctioning paragangliomas due to significant differences in their clinical management, prognosis, and genetic implications.
CASE REPORT
A 29-year-old man with a history of ankylosing spondylitis treated with etanercept was referred to the gastroenterology clinic for elevated liver enzymes. The patient was started on etanercept therapy approximately 1 year before presentation and denied any side effects. During his visit, he denied headache, acute dysphagia, palpitations, diaphoresis, abdominal pain, pruritus, diarrhea, melena, recent weight loss, dark urine, or gross hematuria. The patient was a lifetime nonsmoker and denied the use of alcohol and illicit substances. Physical examination was notable for bilateral paraspinal tenderness, and vital signs were within the normal ranges. His most recent blood test results were significant for elevated levels of hepatic transaminases, alkaline phosphatase, and gamma glutamyl transferase (Table 1). Serological tests for ingestions, viral hepatitis, autoimmune disorders, and metabolic and genetic syndromes were unremarkable. Tumor markers and plasma metanephrine and normetanephrine levels were also normal.
An abdominal ultrasound (US) revealed several mass-like lesions throughout the right hepatic lobe, exerting a mass effect on the porta hepatis. A follow-up magnetic resonance imaging of the abdomen confirmed an external mass likely lymphoproliferative in origin, exerting pressure on the midcommon bile duct, with intrahepatic and extrahepatic biliary ductal dilatation (Figure 1). Compression of the hepatic vasculature led to the development of upper abdominal varices and collaterals in the porta hepatis. Notably, no morphological indications of cirrhosis or intraparenchymal liver lesions were observed.
Magnetic resonance imaging of the abdomen images showing abrupt cutoff of the midcommon bile duct due to the periportal mass (green arrow).
An endoscopic US showed an 11 mm dilation of the common hepatic duct and a mass that was not amenable to biopsy due to increased vascularity. Subsequent endoscopic retrograde cholangiopancreatography demonstrated a 10 mm stenotic area in the main bile duct likely due to extrinsic compression by the porta hepatis mass (Figure 2). Brush cytology samples ruled out malignancy and a 10 Fr by 7 cm plastic biliary stent with a single external flap, and a single internal flap was inserted into the common bile duct to ensure patency. Liver enzyme levels normalized after stent placement. Esophagogastroduodenoscopy revealed small gastroesophageal and duodenal varices that did not require endoscopic intervention.
Endoscopic retrograde cholangiopancreatography image showing a filling defect (blue arrow) with common bile duct dilatation (yellow arrow).
Given the complexity of the case and a high index of suspicion for a lymphoma, oncology service was consulted for comanagement. The diagnostic workup for lymphoma and other hematological disorders was normal. Scrotal US was negative for focal lesions, and staging computed tomography of the chest, abdomen, and pelvis was negative for metastatic disease. Although the positron emission tomography scan showed multiple areas of variable uptake, the radiologist concluded that they were artifacts given the recent use of contrast medium.
An interventional radiologist performed computed tomography-guided core biopsies of the periportal mass, and the histopathology was consistent with an extrahepatic paraganglioma (Figure 3). The neoplastic cells were strongly positive for synaptophysin, chromogranin, and GATA-3 (Figure 3). The cells were negative for CK7, TTF-1, CD45, CDX-2, CAM5.2, cytokeratin AEL/AE3, arginase, and CK20. S100 immunostaining was noncontributory, and the Ki-67 proliferative index was low. The patient was started on doxazosin and propranolol for catecholamine blockage and was referred to surgical oncology 2 weeks later for resection. Laparoscopic resection was aborted because of the high vascularity of the lesion, and portal vein stenting was pursued as a temporizing measure. Radiation therapy with cytoreductive resection was floated as an alternative treatment during the tumor board meeting. Although viable tumors located in other anatomic locations, there is a paucity of data relating to the safety and efficacy of external beam radiation therapy in extrahepatic paragangliomas. The patient continues to follow-up at our clinic with serial blood tests to monitor disease progression. He was also referred to the genetics clinic for counseling and possible testing. If the patient becomes symptomatic or the gastric and duodenal varices resolve, radiation therapy or a more radical resection may be considered.
Histological and immunophenotypic profile of a periportal paraganglioma. Hematoxylin-eosin stains of the periportal mass (panel A, 20×). Note the epithelioid cells with eosinophilic cytoplasm, focal nuclear pleomorphisms, and nuclear hyperchromasia. Core needle biopsy reveals nests (zellballen pattern) of uniform round to oval cells with finely granular eosinophilic cytoplasm and centrally located nuclei with salt-and-pepper chromatin (panel B, 20×). The tumor cells are surrounded by delicate fibrovascular stroma. Immunohistochemical stains of the tumor cells are positive for chromogranin A (panel C, 20×) and synaptophysin, supporting neuroendocrine differentiation.
DISCUSSION
Paragangliomas can be sporadic or familial, with a significant proportion linked to genetic mutations, particularly in succinate dehydrogenase genes.^2,3,8^ Most of these tumors are diagnosed incidentally on imaging during investigations for unrelated complaints. However, about a third of the patients may present with signs of catecholamine excess, such as hypertension, palpitations, chest pain, excess sweating, myocardial infarction, anxiety, and headache.^3,4^ Obstructive jaundice is an extremely rare manifestation of paragangliomas and has only been observed in a few cases (Table 2).^5–8^ This unique presentation can pose a diagnostic challenge and predispose patients to significant perioperative morbidity and mortality.
We describe an exceedingly rare case of extrahepatic paraganglioma presenting as obstructive jaundice and gastroesophageal varices. The patient first presented to our clinic with elevated liver enzymes and was found to have a periportal lesion with a mass effect on imaging. A biliary paraganglioma was confirmed on histopathology, but there was no evidence of metastatic disease or catecholamine excess. In symptomatic patients, the biochemical diagnosis of paragangliomas and pheochromocytomas begins with the detection of catecholamine metabolites (metanephrine and normetanephrine) in urine or serum plasma.^3,4^ Other markers include serum chromogranin A and methoxytyramine, which can be detected in metastatic disease.^3^ Although imaging plays a role in the diagnosis of paragangliomas, histopathology remains the gold standard for diagnosis.^3,4^
Surgical resection is the mainstay of treatment for localized and resectable tumors.^2,3^ The National Comprehensive Cancer Network (NCCN) guidelines recommend preoperative treatment with alpha-adrenergic blockage and fluid therapy to avoid hypertensive crises, malignant arrhythmias, and cardiovascular collapse during surgery.^2–4^ A laparoscopic approach is preferred when feasible to minimize perioperative morbidity. For metastatic or unresectable paragangliomas, other treatment options may include external radiation therapy with cytoreductive resection, immunotherapy, chemotherapy, and active observation.^2,9^
The management of biliary tract paragangliomas poses significant clinical challenges due to their rarity, vascularity, and proximity to critical hepatobiliary structures. In our case, the patient was started on medical therapy to prevent a catecholamine surge and subsequent hypertensive crisis. Endoscopic stenting was performed to relieve biliary obstruction, given the tumor's location encasing the common bile duct. After failed laparoscopic resection, the patient underwent endovascular vein stenting to treat the portal hypertension and varices. The patient is scheduled to follow-up with our service every 3 months for blood pressure monitoring and tumor marker checks as per the NCCN guidelines. For resectable tumors (paraganglioma/pheochromocytoma), the NCCN recommends follow-up within 12 weeks to 12 months of the surgery, then every 6 to 12 months for the first 3 years, and then annually for up to 10 years.^2^ After 10 years, follow-up and imaging are recommended when there is concern for cancer recurrence or metastases.
In summary, biliary paragangliomas are extremely rare neuroendocrine tumors that can present with obstructive jaundice. Although infrequent, these tumors may be considered in the differential diagnosis of biliary lesions as prompt recognition and intervention are crucial.
DISCLOSURES
Author contributions: ID Atogwe conceptualized the idea of this case report. L. Bathobakae and F. Deepali assisted with literature search and drafting of the manuscript. ML Mussa and O. Shoyele edited, fact-checked, and proofread the final version of this case report. O. Shoyele prepared the pathology slides and interpretations. L. Bathobakae is the article guarantor.
Financial disclosure: None to report.
Previous presentation: This case was presented as an abstract at the American College of Gastroenterology (ACG) Annual Scientific Meeting, 2024 in Philadelphia, Pennsylvania. Atogwe, Irhoboudu D. MD,*; Mussa, Maria Lagarde MD, Barrett, Lisa DO, Echikunwoke, Blanche MBBS, Shoyele, Olubunmi MD. S2454 - A rare case of extrahepatic paraganglioma presenting with biliary obstruction in a 29-year-old man. The American Journal of Gastroenterology 119(10S): S1739, October 2024. DOI: 10.14309/01.ajg.0001039184.55876.80
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Atogwe ID Mussa ML Barrett L Echikunwoke B Shoyele O. S 2454 A rare case of extrahepatic paraganglioma presenting with biliary obstruction in a 29-year-old man. Am J Gastroenterol. 2024;119(10S):S 1739.
- 2Shah MH Goldner WS Benson AB Neuroendocrine and adrenal tumors, version 2.2021. JNCCN J Natl Compr Cancer Netw. 2021;19(7):839–67.10.6004/jnccn.2021.003234340212 · doi ↗ · pubmed ↗
- 3Granberg D Juhlin CC Falhammar H. Metastatic pheochromocytomas and abdominal paragangliomas. J Clin Endocrinol Metab. 2021;106(5):E 1937–52.33462603 10.1210/clinem/dgaa 982PMC 8063253 · doi ↗ · pubmed ↗
- 4Lenders JWM Kerstens MN Amar L Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: A position statement and consensus of the Working Group on Endocrine Hypertension of the European Society of hypertension. J Hypertens. 2020;38(8):1443–56.32412940 10.1097/HJH.0000000000002438 PMC 7486815 · doi ↗ · pubmed ↗
- 5Sarma DP Rodriguez FH Hoffmann EO. Paraganglioma of the hepatic duct. South Med J. 1980;73(12):1677–8.7444569 10.1097/00007611-198012000-00050 · doi ↗ · pubmed ↗
- 6Hitanant S Sriumpai S Na-songkla S Pichyangkula C Sindhavananda K Viranuvatti V. Paraganglioma of the common hepatic duct. Am J Gastroenterol. 1984;79(6):485–8.6731425 · pubmed ↗
- 7Caceres M Mosquera LF Shih J O'Leary P. Paraganglioma of the bile duct. South Med J. 2001;94(5):515–8.11372805 · pubmed ↗
- 8Zimmermann A. Paraganglioma of the hepatobiliary tract. In: Tumors and Tumor-Like Lesions of the Hepatobiliary Tract. Springer International Publishing: Cham, Switzerland, 2016, pp 1–11.