Association between Parkinson's disease and risk of colorectal cancer: A systematic review and meta‐analysis
Meng‐Dan Su, Tian‐Hong Wang, Hao‐Wen Zhang, Ke‐Yu Cao, Fei Liu

TL;DR
This study finds that people with Parkinson's disease have a lower risk of developing colorectal cancer compared to healthy individuals.
Contribution
This is the largest meta-analysis to date on the relationship between Parkinson's disease and colorectal cancer risk.
Findings
Parkinson's disease patients had a 26% lower risk of colorectal cancer compared to healthy individuals.
The reduced risk was more pronounced in Asian countries compared to Western countries.
The protective effect was stronger for colon cancer than for rectal cancer.
Abstract
This study aims to investigate the relationship between Parkinson's disease (PD) and colorectal cancer (CRC) risk by a systematic review and meta‐analysis. Using Embase, Pubmed, and Cochrane Library databases, 21 articles reporting clinical data of 1,635,873 PD patients and 10,388,842 healthy individuals were finally included. Based on the results of pooled analysis, we found that PD patients exhibited a decreased risk of CRC (relative risk (RR) = 0.74; 95% confidence interval (CI), 0.68–0.80). In contrast to case‐control (RR = 0.80; 95% CI, 0.64–1) and cohort studies (RR = 0.72; 95% CI, 0.66–0.79), the combined risk of PD patients with CRC in Asian nations (RR = 0.67; 95% CI, 0.58–0.78) was lower than that in Western countries (RR = 0.76; 95% CI, 0.70–0.82). In comparison to rectal cancer (RR = 0.82; 95% CI, 0.69–0.97), PD patients exhibited a lower combined risk of colon cancer (RR =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
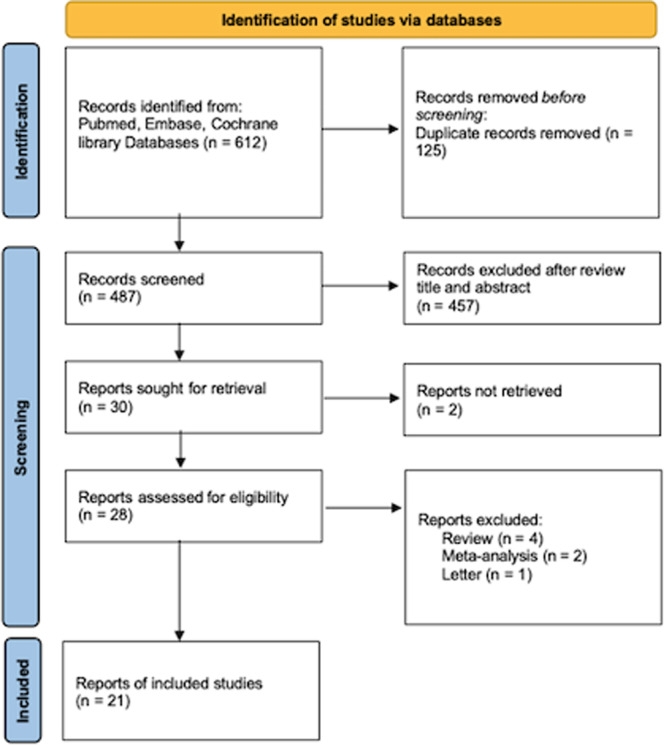 FIGURE 1
FIGURE 1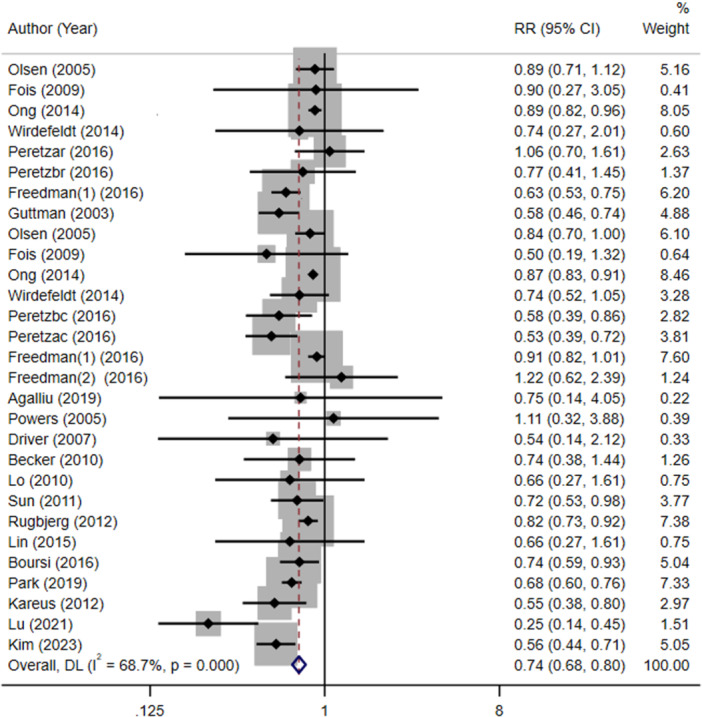 FIGURE 2
FIGURE 2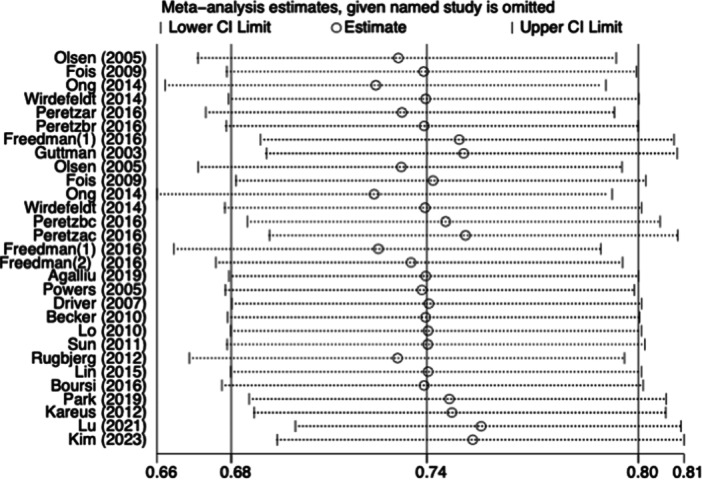 FIGURE 3
FIGURE 3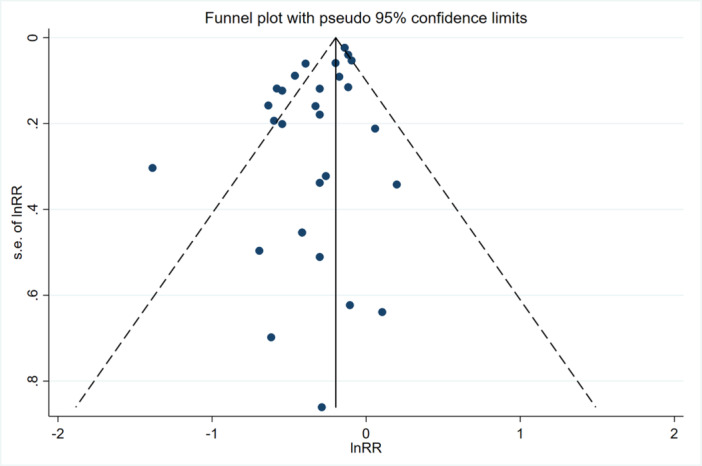 FIGURE 4
FIGURE 4| Author | Year | Country | Study design |
|
| Age |
| Location | Follow‐up |
|---|---|---|---|---|---|---|---|---|---|
| Powers | 2005 | USA | Case‐control | 217 | 100.00% | Median: 69 | 298 | Colorectal | NR |
| Driver | 2007 | USA | Cohort | 487 | NR | Median: 72.2 | 487 | Colorectal | 5.9‐year |
| Becker | 2010 | UK | Cohort | 2993 | 63.30% | NR | 3003 | Colorectal | NR |
| Lo | 2010 | USA | Cohort | 692 | NR | NR | 761 | Colorectal | NR |
| Sun | 2011 | Taiwan, China | Cohort | 4957 | 51.70% | Mean: 51.7 | 19,828 | Colorectal | NR |
| Rugbjerg | 2012 | Denmark | Cohort | 20,343 | 52.70% | Mean: 72.7 | 32,360 | Colorectal | NR |
| Lin | 2015 | Taiwan, China | Cohort | 62,023 | 62.60% | Mean: 66 | 124,046 | Colorectal | NR |
| Boursi | 2016 | UK | Case‐control | 22,093 | 55.10% | Median: 72 | 85,833 | Colorectal | 7‐year |
| Park | 2019 | Korea | Cohort | 52,009 | 41.00% | Mean: 71 | 260,045 | Colorectal | NR |
| Kareus | 2012 | USA | Cohort | 2998 | NR | NR | NR | Colorectal | NR |
| Lu | 2021 | German | Cohort | 328,645 | NR | NR | NR | Colorectal | NR |
| Kim | 2023 | Korea | Cohort | 8381 | 46.73% | NR | 33,524 | Colorectal | NR |
| Olsen | 2005 | Denmark | Cohort | 14,088 | NR | Mean: 72.8 | NR | Colon +rectum | 10‐year |
| Fois | 2009 | UK | Cohort | 4355 | NR | NR | 574,860 | Colon +rectum | 3.4‐year |
| Ong | 2014 | UK | Cohort | 219,194 | 57.00% | NR | 9,015,614 | Colon +rectum | NR |
| Wirdefeldt | 2014 | Sweden | Cohort | 11,786 | 60.50% | Mean: 62.5 | 58,930 | Colon +rectum | 1‐year |
| Peretz | 2016 | Israel | Cohort | 7125 | 54.00% | Mean: 71.2 | NR | Colon +rectum | 10‐year |
| Freedman(1) | 2016 | USA | Case‐control | 836,947 | 54.80% | Mean: 74 | 142,869 | Colon +rectum | 5‐year |
| Guttman | 2003 | Canada | Cohort | 15,304 | NR | NR | 30,608 | Colon | NR |
| Freedman(2) | 2016 | Asia | Case‐control | 20,267 | 58.50% | NR | 5558 | Colon | NR |
| Agalliu | 2019 | USA | Cohort | 969 | 61.90% | 67.8 | 218 | Colon | NR |
| Selection (0–4) Comparability (0–2) Outcome (0–3) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | REC | SNEC | AE | DO | SC | AF | AO | FU | AFU | Total | ||
| Powers | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Driver | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Becker | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Lo | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Sun | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Rugbjerg | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Lin | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |||
| Boursi | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Park | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |||
| Kareus | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Lu | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Kim | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Olsen | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Fois | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Ong | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | |||
| Wirdefeldt | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Peretz | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Freedman(1) | 1 | 1 | 1 | 1 | 1 | 5 | ||||||
| Guttman | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||
| Freedman(2) | 1 | 1 | 1 | 1 | 1 | 5 | ||||||
| Agalliu | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | ||||
| Number of studies | RR | LCI | UCI |
|
|
| |
|---|---|---|---|---|---|---|---|
| Overall | 21 | 0.74 | 0.68 | 0.80 | <0.001 | 68.70% | <0.001 |
| Country | |||||||
| Asia countries | 5 | 0.67 | 0.58 | 0.78 | <0.001 | 28.10% | 0.234 |
| Western countries | 16 | 0.76 | 0.70 | 0.82 | <0.001 | 64.20% | <0.001 |
| Study design | |||||||
| Case‐control | 4 | 0.80 | 0.64 | 1 | 0.048 | 73.40% | 0.005 |
| Cohort | 17 | 0.72 | 0.66 | 0.79 | <0.001 | 69.10% | <0.001 |
| Location | |||||||
| Colon | 9 | 0.76 | 0.67 | 0.86 | <0.001 | 67.40% | 0.001 |
| Rectal | 6 | 0.82 | 0.69 | 0.97 | 0.021 | 57.70% | 0.028 |
| Colorectal | 12 | 0.67 | 0.57 | 0.76 | <0.001 | 56.10% | 0.009 |
| Year of publication | |||||||
| Before 2010 | 5 | 0.76 | 0.66 | 0.88 | <0.001 | 13.90% | 0.318 |
| After 2010 | 16 | 0.74 | 0.68 | 0.80 | <0.001 | 75.90% | <0.001 |
- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParkinson's Disease Mechanisms and Treatments · Ginkgo biloba and Cashew Applications · Nuclear Receptors and Signaling
INTRODUCTION
1
Parkinson's disease (PD) is a recognizable clinical syndrome with a variety of causes and clinical manifestations.1 PD has placed a substantial burden on society as it affected 6.1 million people worldwide in 2016, up from 2.5 million in 1990.2 According to the study, 1.37% of over 60 years old had PD, suggesting that approximately 3.62 million people in China may have PD.3 PD may be difficult to detect in its earliest stages, as reflected by the long delay (average 10 years) between the first symptom and the diagnosis. Tremor at rest, muscle rigidity, akinesia (or bradykinesia), and postural instability, abbreviated as TRAP, are the four cardinal symptoms of PD.4 Classic symptoms of parkinsonism include freezing (motor blocks) and a flexed posture, with PD being the most common kind. Non‐motor symptoms include issues with perception, sleep patterns, and neurobehavioral and cognitive abnormalities.4 Therefore, PD significantly impacts the quality of life for older patients.
Interestingly, epidemiological studies revealed that while PD patients have increased chances of suffering from brain cancer and melanoma, they are less likely to suffer from many common types of cancer, such as hematological, gastrointestinal, lung, and genitourinary malignancies.5, 6, 7 The underlying mechanisms remain poorly understood. A study of 62,023 PD patients in China found that PD was linked to an increased risk of malignant brain tumors, gastrointestinal tract cancers, and lung cancers.8 Another study conducted in Korea demonstrated inverse associations between overall cancer incidence and various types of cancer in individuals with PD. The implications of these findings and their underlying mechanisms warrant additional research.9
Colorectal cancer (CRC) is a type of cancer that affects the colon (large intestine) or rectum, and it is the third most frequent cancer around the world. In 2020, it was estimated that there were 1.9 million new cases of CRC and 930,000 fatalities. Europe, New Zealand, and Australia had the highest incidence rates of CRC.10 Interestingly, a study conducted in Korea, which included 260,045 individuals without PD and 52,009 patients diagnosed with PD between 2010 and 2015, found that patients with PD had a decreased risk of CRC.11 Additionally, a recent study that examined populations from 183 countries indicated that nations with high PD mortality had a reduced probability of CRC mortality.12 As of now, however, the phenomena lack a well‐established explanation, and there is still conflicting evidence linking PD to CRC as an additional investigation revealed no connection between CRC and PD.13 Furthermore, epidemiological research on the link between CRC and PD confronts a variety of methodological problems and probable biases, encompassing diagnostic bias, confounding, conflicting hazards, or selective survival. Moreover, recent studies on the connection between CRC and PD have yielded mixed results. Therefore, this work aims to further explore any potential links between PD and the risk of CRC, addressing the existing uncertainties and providing new insights into this area of research.
METHODS
2
Meta‐analysis was implemented by applying Preferred Reporting Items for Systematic Reviews and Meta‐Analyses guidelines.14
Search strategy and selection
2.1
By searching EMBASE, PubMed, and Cochrane Library with the terms “Parkinson's disease,” “colon cancer,” “rectal cancer,” and “colorectal cancer,” relevant studies published in English up to January 2024 were retrieved. Additionally, we manually reviewed the bibliographies of all relevant articles to ensure no significant studies were missed. The databases were independently searched by two researchers, each oblivious to the other's findings to minimize bias. In the event of a disagreement, the results were reviewed and resolved by a third researcher to reach a consensus. The detailed search strategy for Pubmed database was as follows: (“parkinson disease”[MeSH Terms] OR (“parkinson”[All Fields] AND “disease”[All Fields]) OR “parkinson disease”[All Fields] OR “parkinson s disease”[All Fields]) AND (“colonic neoplasms”[MeSH Terms] OR (“colonic”[All Fields] AND “neoplasms”[All Fields]) OR “colonic neoplasms”[All Fields] OR (“colon”[All Fields] AND “cancer”[All Fields]) OR “colon cancer”[All Fields] OR (“rectal neoplasms”[MeSH Terms] OR (“rectal”[All Fields] AND “neoplasms”[All Fields]) OR “rectal neoplasms”[All Fields] OR (“rectal”[All Fields] AND “cancer”[All Fields]) OR “rectal cancer”[All Fields]) OR (“colorectal neoplasms”[MeSH Terms] OR (“colorectal”[All Fields] AND “neoplasms”[All Fields]) OR “colorectal neoplasms”[All Fields] OR (“colorectal”[All Fields] AND “cancer”[All Fields]) OR “colorectal cancer”[All Fields])).
Eligibility criteria
2.2
The inclusion criteria for this study centered on the relationship between the risk of CRC and PD. Studies that reported relative risk (RR), odds ratio (OR), or hazard ratio (HR) data were included, encompassing various study designs such as cohort studies, case‐control studies, and randomized controlled trials. Exclusion criteria encompassed studies with insufficient data to investigate these ratios, as well as meta‐analyses, reviews, letters, editorials, and case reports. Additionally, duplicate studies were excluded from the analysis.
Data extraction and quality assessment
2.3
Two authors independently collected the following data from the qualified research studies: author, year, nation, research design, number of control groups and cases, sex, age, follow‐up, tumor location, as well as outcomes. The quality of the included studies was evaluated according to the Newcastle‐Ottawa scale (NOS).15 The scale ranges from zero to nine stars: studies with scores higher than or equal to five are considered methodologically sound. It was performed independently by two researchers to reduce bias and risk. In cases where discrepancies arose, a third reviewer was consulted to resolve the differences.
Statistical analysis
2.4
The association between CRC risk and PD was assessed utilizing pooled RR and matching 95% confidence intervals (CIs) based on selnRR and lnRR. Heterogeneity between the studies was evaluated through the I ^2^ statistical approach and Q‐test to determine variation not solely caused by chance. I ^2^ ≥ 75%, 50% < I ^2^ ≤ 75%, 25% < I ^2^ ≤ 50%, and I ^2^ ≤ 25% indicated considerable, substantial, moderate, and slight heterogeneity, respectively. Subgroup analyses were performed based on countries, study design, year of publication, and tumor location. Sensitivity analysis was conducted on each research individually to ensure the stability of the results. A publication bias assessment was carried out utilizing Begg's test and funnel plots. A statistically significant result was defined as p < 0.05, and STATA version 16.0 was exploited for all statistical analyses.
RESULTS
3
Basic characteristics
3.1
Based on the search strategies, a total of 612 literatures were retrieved. After an initial review of the abstracts and titles, 28 papers were selected for further assessment. Of these, 21 articles5, 8, 9, 11, 12, 13, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30 were included in the final analysis, which provided relevant data on the relationship between PD and CRC. These studies involved a total of 1,635,873 PD patients and 10,388,842 healthy individuals. The flow chart of the study selection process is presented in Figure 1. Of the included studies, 16 studies were conducted in Western countries and 5 studies were from Asian countries. Furthermore, 17 studies were cohort studies, and four studies were case‐control studies. Seven studies were published in 2010 or earlier, and 14 studies were published after 2010. There has been evidence from nine studies linking PD to the risk of colon cancer, six studies linking PD to the risk of rectal cancer, and 12 studies linking PD to the risk of CRC (studies including colon cancer and rectal cancer, but did not analyze it separately). The detailed information of basic characteristics is shown in Table 1.
Flow chart of selection studies and specific reasons for exclusion. [Color figure can be viewed at wileyonlinelibrary.com]
Quality assessment
3.2
Two studies received a score of 5, nine studies received a score of 6, seven studies received a score of 7, and three studies received an 8 when the quality of the included studies was evaluated using the NOS (Table 2).
Relationship between PD and risk of CRC
3.3
The pooled RRs of CRC in people with and without PD are displayed in Table 3. When all 21 studies were included, we discovered that PD patients had a significantly decreased risk of CRC (RR = 0.74; 95% CI, 0.68–0.80) (Figure 2).
The meta‐analysis forest plot of the association between PD and CRC. Abbreviations: CRC, colorectal cancer; PD, Parkinson's disease; RR, relative risk. [Color figure can be viewed at wileyonlinelibrary.com]
Subgroup analysis
3.4
Even after the studies were stratified by country, tumor location, and research design, there was still an inverse relationship between CRC risk and PD. The combined risk of PD patients with CRC in Asian nations (RR = 0.67; 95% CI, 0.58–0.78) was lower than that in Western countries (RR = 0.76; 95% CI, 0.70–0.82) (Table 3), according to assessments that were country‐specific. A consistent lower cancer risk was seen in subset analyses of both research types, with a total RR of 0.80 for case‐control studies (RR = 0.80; 95% CI, 0.64–1) and 0.72 for cohort studies (RR = 0.72; 95% CI, 0.66–0.79) (Table 3). As for the tumor location, in comparison to rectal cancer (RR = 0.82; 95% CI, 0.69–0.97), PD patients exhibited a lower combined risk of colon cancer (RR = 0.76; 95% CI, 0.67–0.86) (Table 3). Although the combined risk of PD patients in studies published before 2010 (RR = 0.76; 95% CI, 0.66–0.88) was only slightly higher than that of those in studies published after 2010 (RR = 0.74; 95% CI, 0.68–0.80), they all indicated that PD patients had a significantly decreased risk of CRC. All of these subgroup analyses revealed that the significant inverse association between PD and the risk of CRC was not undermined by many factors, including country, study design, tumor location, and publication time of the study.
Sensitivity analysis and publication bias
3.5
Sensitivity analysis revealed no significant variation between studies when the pooled RR and 95% CI were recalculated after omitting each study in turn (Figure 3). Additionally, there was no remarkable publication bias for the risks of CRC based on Begg's test (p = 0.91) and inspection of the funnel plot (Figure 4), suggesting that our findings were robust.
The sensitivity analysis of the association between PD and CRC. Abbreviations: CI, confidence interval; CRC, colorectal cancer; PD, Parkinson's disease.
The meta‐analysis funnel plot of the association between PD and CRC. Abbreviations: CRC, colorectal cancer; PD, Parkinson's disease. [Color figure can be viewed at wileyonlinelibrary.com]
DISCUSSION
4
PD, a neurodegenerative disorder, and cancer, characterized by uncontrolled cellular proliferation, can be viewed as contrasting biological processes. However, the question arises as to whether there is a close clinical association. Epidemiological evidence demonstrates inconsistent associations between PD and CRC. For instance, one study included 8381 PD patients showed inverse associations between CRC in patients with PD.9 Another study, which utilized national cause‐specific death data from 183 countries extracted from the Global Health Observatory database, indicated a negative association between PD and CRC.12 Furthermore, a meta‐analysis investigating the association between PD and cancer revealed that individuals with PD exhibited decreased susceptibility to colon, rectal, colorectal, and lung cancers while experiencing heightened risks of brain cancer and melanoma.31 However, a third study utilizing Epidemiology, Surveillance, and End Results‐Medicare linked data (1992–2005) of persons over 65 years, which included 743,779 cancer patients with PD as well as a non‐cancer group (n = 419,432) in prospective cohort analyses, showed no correlation between CRC risk and PD.18 Thus, it was necessary to comprehensively analyze the complex associations between the two conditions in a large population. So far, our study was the largest meta‐analysis to assess the relationship between CRC and PD. Although inconsistent results existed in some research studies, the investigation including 21 studies involving 1,635,873 PD patients and 10,388,842 healthy individuals indicated that PD is a protective factor against CRC. Besides, we carried out subgroup analysis using stratified variables such as tumor location, research design, research region, and publication time of the study, which all support a negative association between PD and the risk of CRC. Based on the above results, we can conclude that PD patients might have a lower risk of CRC.
Several mechanisms contribute to the pathogenesis of PD and some kinds of neoplasms, including mitochondrial dysfunction, oxidative stress, DNA damage, abnormalities in mitosis‐stimulating signals, inflammatory factors, and anomalies in cell cycle activation. Additionally, certain biochemical substances, such as α‐synuclein, a marker for PD, may potentially stimulate malignant cells.32 Several studies suggest a potential association between dopamine receptors (DR) and susceptibility to malignancies. DR polymorphisms have been linked to an increased risk of non‐small‐cell lung cancer and gastric cancer, while heightened expression of dopamine D2 receptors (DR2) has been observed in various cancer types such as gastric cancer, neuroendocrine tumors, glioma, and breast cancer.33 One study reported several genes that link the association between cancer and PD. Approximately half of the cases of PD with early onset are caused by mutations in the Parkin gene, which was already thought to be a tumor suppressor gene due to its location on the long arm of chromosome 6, a section of which has long been recognized to be changed or deleted in a variety of human malignancies. Furthermore, parkinsonism‐associated deglycase (PARK7), and leucine‐rich repeat kinase 2 (LRRK2) play a vital role in the link between the two diseases.34 Additionally, Chen and his colleagues reported that PD patients had decreased probabilities of developing colon cancer, owing to the regulation of autophagy flux by the PD‐associated gene ATPase cation transporting 13A2 (ATP13A2).35 Additionally, one research found that dysbiosis and changed colonic microbiota in PD patients may be the mechanism behind the association between CRC and PD.36 Previous research has presented that the fecal microbiota and colonic mucosa from patients with PD differ from those of healthy people.37 Other mechanisms of the pathogenesis of PD and neoplasms, such as oxidative stress, mitochondrial dysfunction, inflammatory factors, DNA damage, and abnormal mitosis‐stimulating signals also play critical roles, which still need further investigation.
The strengths of this meta‐analysis and systematic review include that it utilizes the largest clinical data to assess the correlation between CRC risk and PD. In recent years, an increasing number of studies have explored this correlation; this work provides a comprehensive summary, stratified by year of publication. Although previous research presented conflicting views on the connection between CRC risk and PD, this review, with the largest sample size available, indicated that PD is associated with a lower risk of CRC.
However, there are limitations to this study. The included investigations were predominantly retrospective, introducing potential bias. While efforts were made to match the most significant confounding variables, and multivariate analyses were conducted to obtain reliable estimates of HR, OR, and RR, some factors may still not have been accounted for. Additionally, the funnel plot analysis revealed that a substantial number of studies fell outside the CIs, particularly at the top of the funnel. This suggests that the inclusion of a larger number of studies may compromise the unbiased conclusion due to increased variability in estimated effect sizes. This variability could be attributed to differences in patient enrollment criteria, such as age, race, sex, and individual patient variation. What is more, the etiology of CRC and PD, as well as the underlying mechanisms behind the inverse association between these two diseases, are complex and warrant further investigation.
Building upon the current study, future research could focus on the underlying mechanism of decreased risk of CRC in PD patients. Emerging research supports the existence of shared genetic pathways between PD and cancer, offering potential insights for novel approaches to tumor management. Furthermore, advancing understanding of the etiopathogenesis of PD and cancer has the potential to facilitate the creation of innovative diagnostic techniques with practical implications. Elucidating the potential mechanisms underlying these pathologies and their interrelated dependencies may serve as a foundation for the development of precise therapeutic interventions for both disease conditions.
CONCLUSION
5
According to our results, patients with PD had a lower risk of CRC; however, the underlying mechanisms are still unclear and require further research to be fully understood.
AUTHOR CONTRIBUTION
Meng‐Dan Su and Fei Liu conceptualized the study; Meng‐Dan Su, Hao‐Wen Zhang, Ke‐Yu Cao, Tian‐Hong Wang, and Fei Liu developed the methodology; Meng‐Dan Su and Hao‐Wen Zhang managed the software; Meng‐Dan Su, Hao‐Wen Zhang, and Tian‐Hong Wang conducted the statistical analysis and revised the manuscript; Meng‐Dan Su, Hao‐Wen Zhang, and Fei Liu reviewed the manuscript. All the authors have read and approved the final version of the manuscript.
CONFLICT OF INTEREST STATEMENT
Fei Liu, who is also an editorial member of Ibrain, is excluded from editorial decision‐making related to the acceptance and publication of this article. Editorial decision‐making was handled independently by the editors‐in‐chief to minimize bias. Other authors declare no conflicts of interest.
ETHICS STATEMENT
Not applicable since all analyses were based on previously published research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bloem BR , Okun MS , Klein C . Parkinson's disease. Lancet. 2021;397(10291):2284‐2303. 10.1016/s 0140-6736(21)00218-x 33848468 · doi ↗ · pubmed ↗
- 2Dorsey ER , Elbaz A , Nichols E , et al. Global, regional, and national burden of Parkinson's disease, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):939‐953. 10.1016/s 1474-4422(18)30295-3 30287051 PMC 6191528 · doi ↗ · pubmed ↗
- 3Qi S , Yin P , Wang L , et al. Prevalence of Parkinson's disease: a community‐based study in China. Mov Disorders. 2021;36(12):2940‐2944. 10.1002/mds.28762 34390510 · doi ↗ · pubmed ↗
- 4Jankovic J . Parkinson's disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79(4):368‐376. 10.1136/jnnp.2007.131045 18344392 · doi ↗ · pubmed ↗
- 5Ong EL , Goldacre R , Goldacre M . Differential risks of cancer types in people with Parkinson's disease: a national record‐linkage study. Eur J Cancer. 2014;50(14):2456‐2462. 10.1016/j.ejca.2014.06.018 25065294 · doi ↗ · pubmed ↗
- 6Hang Z , Lei T , Zeng Z , Cai S , Bi W , Du H . Composition of intestinal flora affects the risk relationship between Alzheimer's disease/Parkinson's disease and cancer. Biomed Pharmacother = Biomed Pharmacother. 2022;145:112343. 10.1016/j.biopha.2021.112343 34864312 · doi ↗ · pubmed ↗
- 7Leong YQ , Lee SWH , Ng KY . Cancer risk in Parkinson disease: an updated systematic review and meta‐analysis. Eur J Neurol. 2021;28(12):4219‐4237. 10.1111/ene.15069 34403556 · doi ↗ · pubmed ↗
- 8Lin PY , Chang SN , Hsiao TH , Huang BT , Lin CH , Yang PC . Association between Parkinson disease and risk of cancer in Taiwan. JAMA Oncol. 2015;1(5):633‐640. 10.1001/jamaoncol.2015.1752 26181771 · doi ↗ · pubmed ↗