The Impact of a Laboratory Error on a Patient’s Well Being: A Case Report on Overdiagnosis and Its Consequent Iatrogenesis
Luís Laranjeira Correia, Joana Ferreira Vieira, Catarina Oliveira Neves, Maria de Freitas Domingues

TL;DR
A lab error led to unnecessary cancer tests for a 77-year-old woman, causing emotional distress and highlighting the risks of overdiagnosis.
Contribution
This case emphasizes the need for cautious test ordering and patient involvement to prevent iatrogenic harm and promote quaternary prevention.
Findings
A laboratory error caused a urinary cytology test instead of a thyroid FNAC, leading to unwarranted cancer suspicion.
The patient experienced anxiety and disrupted family life due to unnecessary invasive tests and follow-ups.
The case underscores the importance of evidence-based test prescribing to avoid overdiagnosis and preserve healthcare resources.
Abstract
Overdiagnosis, resulting from excessive use of diagnostic tests, can lead to unnecessary treatments and negatively impact patients' quality of life. This case highlights the importance of prescribing tests based on the best scientific evidence to avoid emotional and financial harm to patients while promoting quaternary prevention. A 77-year-old woman, undergoing surveillance for a thyroid nodule, mistakenly underwent a urinary cytology test, which revealed a suspicious finding. Due to this incidental result, the Family Physician referred her to a Urology consultation to rule out urothelial cancer. The subsequent investigations included renal and pelvic CT scans, urethrocystoscopy, and repeated urinary cytology, all of which yielded negative results for malignancy. Throughout this process, the patient experienced anxiety, sadness, and loss of appetite, which also affected her family…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
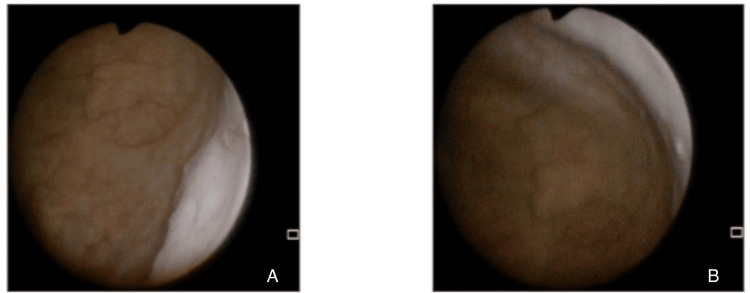 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare cost, quality, practices · Health Systems, Economic Evaluations, Quality of Life · Clinical Reasoning and Diagnostic Skills
Introduction
Diagnostic tests are valuable tools for determining the correct diagnosis based on a patient’s clinical history and symptoms, facilitating medical decision-making. However, overdiagnosis refers to the detection of an alteration or disease that would not have caused any complaints or harm in the future. Apart from the waste of healthcare resources, overdiagnosis can harm patients by leading to overtreatment with associated risks, anxiety, depressive states related to the diagnosis, labeling, or financial burden. This case report illustrates the impact of diagnostic suspicion on the quality of life of an asymptomatic patient who underwent an unintended clinical test. It aims to emphasize the importance of prescribing diagnostic tests based on the best available scientific evidence, ensuring not only secondary prevention but also quaternary prevention [1-4].
Case presentation
The patient is a 77-year-old retired cleaning worker, autonomous in daily living activities and cognitively intact. She was classified as having stage VIII in Duvall’s family life cycle, with a functional family Apgar score and Graffar class 3. Her medical history included dyslipidemia, type 2 diabetes mellitus, hypertension, ischemic stroke in 2009, and multinodular euthyroid goiter with a dominant 16 mm nodule on the right lobe. Family history included a son with Graves' disease, a daughter diagnosed with breast cancer at 55 years old, and a maternal aunt with a diagnosis of colorectal cancer at 40 years old. Her medication regimen included acetylsalicylic acid 100 mg daily, atorvastatin 20 mg daily, metformin 500 mg twice daily, and perindopril/indapamide 10 mg/2.5 mg daily. She has no smoking or drug use habits.
Due to the stability of her thyroid condition, she was discharged from the General Surgery outpatient clinic, with a recommendation for follow-up by the Family Physician, including annual ultrasound evaluations and fine-needle aspiration cytology (FNAC) if there was dimensional growth of the nodule. During a follow-up visit, the patient was asymptomatic, and a thyroid ultrasound was requested as per protocol. The report indicated a 2 mm increase in the dominant nodule, leading to an FNAC request via a non-cervicovaginal exfoliative cytology test, specifying that the sample was for a thyroid nodule biopsy.
The patient later returned with the results of a mistakenly performed urinary cytology, which identified atypical urothelial cells (Paris classification). Despite the absence of urinary symptoms, due to this incidental finding, the Family Physician ordered a renal and pelvic CT scan and referred her to a Urology consultation to rule out urothelial malignancy. The imaging study showed no abnormalities in the urinary system. In the outpatient Urology consultation, the patient underwent urethrocystoscopy, which showed no alterations (Figure 1), and a repeat urinary cytology, which was negative for high-grade urothelial carcinoma (Paris classification). Consequently, she was discharged from the hospital consultation.
Endoscopic views obtained during urethrocystoscopyA: Lateral bladder wall with a uniformly smooth urothelium, a faint arborising vascular network, and no focal mucosal irregularities or suspicious lesions; B: Trigone and bladder-neck region with intact urothelium, adequate luminal distension, and no macroscopic evidence of inflammation, hyperplasia, or neoplastic growth
At a subsequent follow-up visit, the patient reported experiencing increased anxiety, sadness, and health-related concerns during the three-month period in which the suspicion of urothelial pathology loomed over her. She also described a decrease in appetite. Additionally, she mentioned that her family was significantly worried, especially her husband and children. However, after receiving the positive outcome, she noticed a gradual improvement in her emotional state and appetite. A physical examination revealed a weight loss of 4 kg since the initial evaluation.
Discussion
The test requested by the Family Physician was a non-cervicovaginal exfoliative cytology. This type of test can refer to FNAC, exfoliative cytology, cytology of secretions, cytology of respiratory tract washes and brushings, or cytology of fluids (urine, ascitic fluid, or pleural fluid). Therefore, additional information is required to specify the intended test.
In this case, despite the correct specification in the diagnostic request, a laboratory error led to the performance of urinary cytology instead of FNAC. After undergoing an unintended diagnostic test, the patient was left with a suspicion of cancer despite having no personal or family history supporting such a diagnosis. The suspicion and subsequent excessive testing caused the patient and her family significant anxiety and distress. She underwent invasive tests with potential iatrogenic risks and misspent valuable healthcare resources in a National Health Service facing sustainability challenges [1].
Conclusions
This case illustrates the impact of overdiagnosis, particularly in asymptomatic individuals, highlighting the importance of investing in quaternary prevention. To prevent excessive medical intervention and its consequent iatrogenesis, healthcare professionals should prioritize the judicious and economically rational prescription of diagnostic and therapeutic tests. Additionally, clear communication between the prescribing physician and the laboratory is essential, along with patient empowerment in seeking appropriate healthcare and understanding the benefits and drawbacks of diagnostic and therapeutic procedures. Furthermore, the role of the Family Physician is crucial in understanding patients' thoughts, expectations, emotions, and fears concerning diagnostic and therapeutic procedures. Physicians must be attentive to how patients perceive their health status and the impact it may have on their social and family lives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Overdiagnosis in primary care: framing the problem and finding solutions BMJ Kale MS Korenstein D 0362201810.1136/bmj.k 2820 PMC 688986230108054 · doi ↗ · pubmed ↗
- 2From primary prevention to quaternary prevention (Article in Portuguese)Rev Port Saude Publica Almeida LM 16232005 https://www.docsity.com/pt/docs/da-prevencao-primordial-a-prevencao-quaternaria/9402707/
- 3Quaternary prevention against medical excesses (Article in Portuguese)Rev Port Med Geral Fam Melo M 289293232007 https://rpmgf.pt/ojs/index.php/rpmgf/article/view/10361
- 4Communication in a Clinical Context (Text in Portuguese) Nunes JM Lisboa Health Care 2010 https://www.mgfamiliar.net/wp-content/uploads/livrocomunic.pdf