Refractory Primary Duodenal Plasmacytoma Displaying t(11;14): A Report of a Rare Case
Nora El Maachi, Marlene Ochmann, Claire Belchet

TL;DR
This paper reports a rare case of a duodenal plasmacytoma with t(11;14) that was resistant to initial treatment and required a different therapy.
Contribution
The first reported case of duodenal extramedullary plasmacytoma with t(11;14) and its treatment response.
Findings
The patient was diagnosed with duodenal plasmacytoma using fibroscopy and immunohistochemistry.
The tumor displayed t(11;14), a genetic abnormality not previously reported in this location.
Initial radiotherapy failed, but daratumumab-based treatment showed some response.
Abstract
Extramedullary plasmacytoma (EMP) involving the digestive tract is a very rare entity that represents only a very small fraction of multiple myeloma (MM) cases. We describe an unusual case of a 71-year-old man with EMP involving the duodenum who initially presented to the emergency room with melena. The final diagnosis was duodenal plasmacytoma with t(11;14), and the diagnosis was reached by fibroscopy with biopsy and immunohistochemistry (IHC). The patient received local radiotherapy and showed failure three months after treatment. Then, he was administered daratumumab-based treatment associated with Revlimid and dexamethasone (DRD). To our knowledge, this is the first report showing duodenal involvement by EMP with t(11;14).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
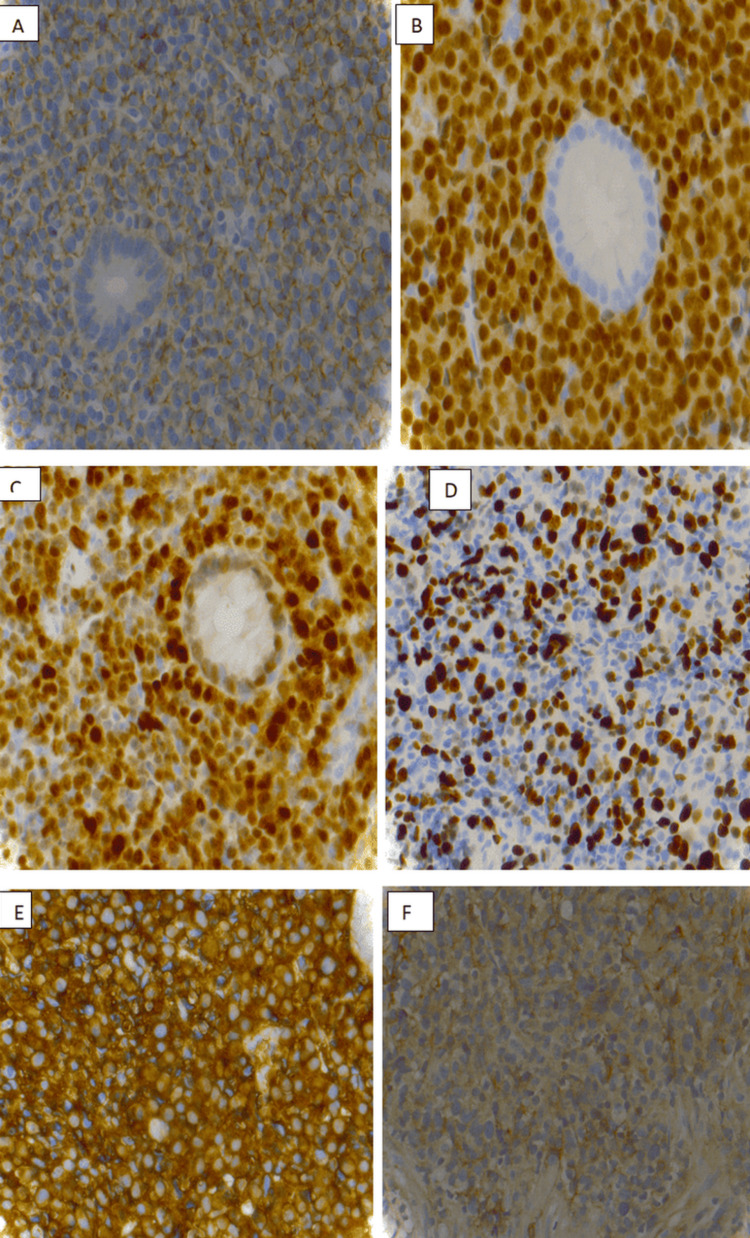 Figure 1
Figure 1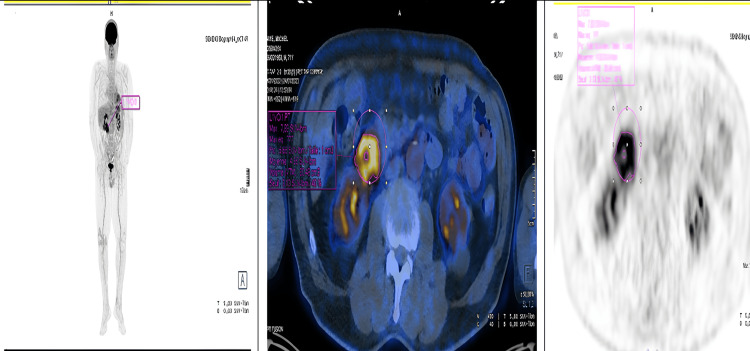 Figure 2
Figure 2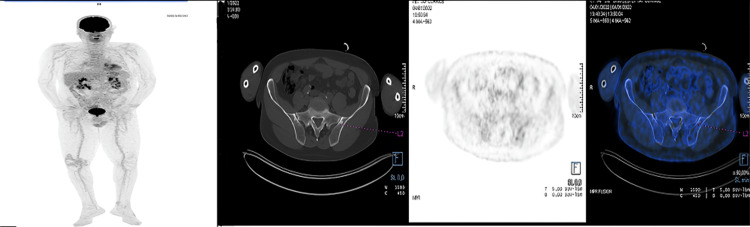 Figure 3
Figure 3| Routine laboratory tests | Values |
| Lactate dehydrogenase | 135 (U/L) |
| Beta-2 microglobulin | 3 mg/L |
| Calcium | 8.5 mg/dL |
| Renal function | eGFR: 90 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Peptidase Inhibition and Analysis · Cancer Mechanisms and Therapy
Introduction
Extramedullary plasmacytoma (EMP) is a rare type of plasma cell neoplasm that arises in soft tissues without the involvement of the bone marrow [1]. Gastrointestinal (GI) tract involvement in EMP is particularly uncommon, accounting for less than 1% of multiple myeloma (MM) cases [2]. EMP is known to be highly sensitive to radiotherapy [1]. Due to its rarity, we present a case involving a 71-year-old man diagnosed with duodenal plasmacytoma carrying the t(11;14) translocation. Initially, the patient was treated with localized radiotherapy, which did not yield a response. Subsequently, he was administered a daratumumab-based treatment associated with Revlimid and dexamethasone (DRD).
Case presentation
A 71-year-old man with a medical history of hypertension, multinodular goiter, chronic bronchitis, polycystic kidney disease, and bilateral orchiepididymitis presented to the emergency room with melena and hematochezia. He did not report any history of bleeding, abdominal operation, or use of antithrombotic agents or nonsteroidal anti-inflammatory drugs (NSAIDs). On physical examination, the patient appeared pale, although hemodynamic status remained stable. Mild tenderness was noted around the epigastric region. Laboratory tests revealed severe normocytic normochromic anemia with a hemoglobin level of 6.4 g/dL. An upper GI endoscopy showed a hemi-circumferential duodenal ulcer (Forrest classification Ib) without Helicobacter pylori infection. No hemostatic intervention was possible. Multiple endoscopic biopsy samples were taken, and histology showed a chorion massively infiltrated by a small lymphoid population, with diffuse architecture and strong plasma cell differentiation without lymphoepithelial lesion. Immunohistochemistry (IHC) was negative for cluster of differentiation 20 (CD20), CD79a, CD5, CD56, CD23, and CD10 and B-cell lymphoma 6 (BCL-6)-negative for B-cell markers. Immunostaining was strongly positive for the plasma cell marker CD138 with monotype immunoglobulin A (IgA) kappa consistent with plasmacytoma, multiple myeloma oncogene-1 (MUM1) (100%), and cyclin D1 (100%) (Figure 1). Anti-CD117 labels scattered mast cells in the chorion. A test for Epstein-Barr virus (EBV) was negative.
(A) Positive immunostaining for the plasma cell marker CD138 (400×). (B) Positive plasma cell marker MUM1 (400×). (C) Positive plasma cell marker cyclin D1 (400×). (D) Plasma cell marker Ki67 (400×). (E) Fine membrane granular positivity for kappa immunoglobulin light chain (400×). (F) Fine membrane granular positivity for lambdaCD138, cluster of differentiation 138; MUM1, multiple myeloma oncogene-1
Fluorescence in situ hybridization (FISH) for multiple myeloma markers revealed a positive result for translocation t(11;14), confirming the presence of translocation CCND1-IGH. Bone marrow aspirate showed 2% poorly differentiated plasma cells. Cytofluorometry was without atypia. Serum protein electrophoresis showed no monoclonal protein.
Serum free light chain analysis showed elevated kappa (34 mg/L) and lambda (20 mg/L) levels, with a mildly increased kappa/lambda ratio. Routine laboratory tests, including serum lactate dehydrogenase (LDH), beta-2 microglobulin, serum calcium, and renal function, were all within normal limits (Table 1).
Positron emission tomography/computed tomography (PET/CT) revealed pathological hypermetabolism corresponding to the tumoral infiltration in the second portion of the duodenum, with a maximum standardized uptake value (SUVmax) of 16.8. Additionally, a hypermetabolic focus was noted in the right prostatic lobe, warranting further evaluation with total prostate-specific antigen (PSA) testing. No other suspicious metabolic abnormalities were identified on whole-body imaging (Figure 2).
PET/CT at diagnosis showed pathological hypermetabolism at the height of the tumoral infiltration of the second duodenum (SUVmax: 16.8)PET/CT, positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value
The patient underwent intensity-modulated radiation therapy (IMRT) with a total dose of 50 Gy, delivered in five fractions over five weeks, beginning in March 2022. As no Helicobacter pylori infection was identified, eradication therapy was not initiated.
Follow-up PET/CT imaging in June 2022 demonstrated a decrease in both the size and metabolic activity of the duodenal lesion, with the SUVmax reduced from 16.8 to 7.2, indicating a partial metabolic response. However, new hypermetabolic bone lesions were observed in the left iliac bone and the distal femur, without evidence of paramedullary extension (Figure 3).
PET/CT three months after radiotherapy revealed a decrease in size and fixation of tumor hypermetabolic infiltration of the duodenum (SUVmax: 7.2 versus 16.8). Partial metabolic response to duodenal injury. The appearance of hypermetabolic bone lesions of the left iliac bone and the lower extremity of the left femur, without paramedullary extensionPET/CT, positron emission tomography/computed tomography; SUVmax, maximum standardized uptake value
A follow-up upper gastrointestinal endoscopy in June revealed an ulcerated lesion with a fibrinous base originating at the genu superius, along with ulcerated and stenotic infiltrative involvement of the duodenal mucosa extending to the second portion (D2). Biopsies confirmed the persistence of the duodenal infiltration by monotypic kappa-restricted plasma cells expressing cyclin D1, consistent with the previously established diagnosis.
Repeat immunofixation electrophoresis for immunoglobulins (IgG, IgA, and IgM) and light chains (kappa and lambda) remained negative for monoclonal protein.
The patient was started on a DRD regimen comprising daratumumab 1800 mg subcutaneously on days 1, 8, and 15; lenalidomide (Revlimid) 25 mg orally on days 1-21; and dexamethasone 20 mg orally on days 1-2 and once weekly. Each treatment cycle was 28 days in duration. By the end of September, the patient had completed three treatment cycles without any reported toxicity. At the time of reporting, the patient remains under treatment, and no posttreatment evaluation data are yet available to assess therapeutic response.
Discussion
Multiple myeloma (MM) with extramedullary plasmacytoma (EMP) is a rare clinical entity, accounting for approximately 3%-5% of all plasmacytomas [1,3]. EMP involving the gastrointestinal (GI) tract is particularly uncommon. Among reported cases, the small intestine is the most frequently affected site, followed by the stomach, colon, and esophagus [4].
Due to its rarity, there are currently no consensus guidelines for the management of intra-abdominal EMP [5]. Treatment strategies are typically guided by institutional protocols or individual clinician experience. Reported approaches include surgical resection, radiotherapy, systemic chemotherapy, or a combination of these modalities [6]. Optimal patient outcomes are best achieved through multidisciplinary team discussions involving surgery, hematology, oncology, pathology, and radiology.
To our knowledge, this is the first reported case of a duodenal plasmacytoma with a t(11;14) translocation. EMP is generally considered highly radiosensitive. Various radiotherapy protocols have been described, such as targeted radiotherapy delivering 40-50 Gy over four weeks, which was the approach used in our case [6,7]. However, our patient demonstrated a refractory response to radiotherapy, necessitating systemic treatment with a chemotherapy regimen.
This case also underscores the importance of a thorough diagnostic workup upon the identification of EMP. This should include serum and urine protein electrophoresis with immunofixation, free light chain analysis, bone marrow biopsy, and the radiographic evaluation of the axial skeleton to assess for systemic involvement and inform treatment planning.
Future directions
Further research is warranted to better understand the biological behavior of extramedullary plasmacytomas with t(11;14), as well as to evaluate the efficacy and safety of targeted therapies such as BCL-2 inhibitors in this context.
Conclusions
Gastrointestinal involvement in EMP remains extremely rare. Given the potential sensitivity of t(11;14)-positive plasma cell neoplasms to BCL-2 inhibition, agents such as venetoclax may represent promising alternatives, particularly in refractory cases. Clinicians should consider the early integration of molecular diagnostics into treatment planning to identify high-risk features and guide individualized therapy.
Collaboration between international specialist centers is essential. Establishing registries and collecting standardized clinical data will improve future treatment strategies and improve outcomes for those with EMP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Refractory primary extramedullary plasmacytoma in kidney: a case report J Int Med Res Niu W Zhang L Wu Y Li K Sun L Ji H Zhang B 30006052110637134920213493950910.1177/03000605211063713 PMC 8829794 · doi ↗ · pubmed ↗
- 2Duodenal ulcer with massive gastrointestinal hemorrhage as an initial manifestation in multiple myeloma with extramedullary disease: a case report Medicina (Kaunas) Chiu HT Chen PH Yen H 1345820223505644210.3390/medicina 58010134 PMC 8780751 · doi ↗ · pubmed ↗
- 3Secondary extramedullary plasmacytoma of the duodenum: an unusual endoscopic presentation Gastroenterology Res Gravina AG Federico A Sica A 110111620132778523910.4021/gr 547w PMC 5051155 · doi ↗ · pubmed ↗
- 4Gastrointestinal manifestations of extramedullary plasmacytoma: a narrative review and illustrative case reports Ann R Coll Surg Engl Glasbey JC Arshad F Almond LM Vydianath B Desai A Gourevitch D Ford SJ 37137610020182969219410.1308/rcsann.2018.0015 PMC 5956591 · doi ↗ · pubmed ↗
- 5Extramedullary plasmacytoma in the presence of multiple myeloma: clinical correlates and prognostic relevance Onco Targets Ther Chen HF Wu TQ Li ZY 329334520122315268810.2147/OTT.S 35348 PMC 3496411 · doi ↗ · pubmed ↗
- 6Extramedullary plasmacytoma of the small intestine and mesentery: a rare case report Int J Surg Case Rep Patel T Lincango E Mc Intosh M Shockley M San Miguel F 11096712820253996551910.1016/j.ijscr.2025.110967 PMC 11875793 · doi ↗ · pubmed ↗
- 7Management of extramedullary plasmacytoma: role of radiotherapy and prognostic factor analysis in 55 patients Chin J Cancer Res Wen G Wang W Zhang Y Niu S Li Q Li Y 4384462920172914246310.21147/j.issn.1000-9604.2017.05.08PMC 5677129 · doi ↗ · pubmed ↗