Contracted or Vanishing Gallbladder: A Case Report
Karthika PS, Sundeep Selvamuthukumaran, Pola Govardhan Kumar, BV Sreedevi, Ankita Swarnkar

TL;DR
This case report describes a rare condition called a 'vanishing' gallbladder in a 34-year-old man with diabetes, alcohol use, and liver cirrhosis, highlighting the challenges in diagnosis and treatment.
Contribution
The report provides a detailed clinical case of a contracted gallbladder in a young patient with multiple comorbidities, emphasizing the need for multidisciplinary care and adaptive surgical strategies.
Findings
The patient's gallbladder was severely atrophied due to chronic inflammation and fibrosis.
Laparoscopic cholecystectomy was converted to open surgery due to dense adhesions and fibrosis.
Multidisciplinary care was essential for managing the patient's complex medical conditions.
Abstract
A contracted or "vanishing" gallbladder is a condition characterized by severe atrophy or fibrosis of the gallbladder, often resulting from chronic inflammation, recurrent cholecystitis, gallstone disease, or metabolic disorders such as diabetes and chronic alcohol use. The etiopathogenesis involves progressive fibrosis due to persistent biliary obstruction, chronic infection, or impaired blood flow, particularly in patients with liver cirrhosis. While the exact incidence remains unclear, it is more prevalent in individuals with long-standing hepatobiliary diseases or metabolic syndromes. Common symptoms include severe right upper quadrant pain, jaundice, nausea, vomiting, and signs of obstructive jaundice, such as dark urine and pale stools. Diagnostic investigations typically involve ultrasound, contrast-enhanced computed tomography (CECT), magnetic resonance cholangiopancreatography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1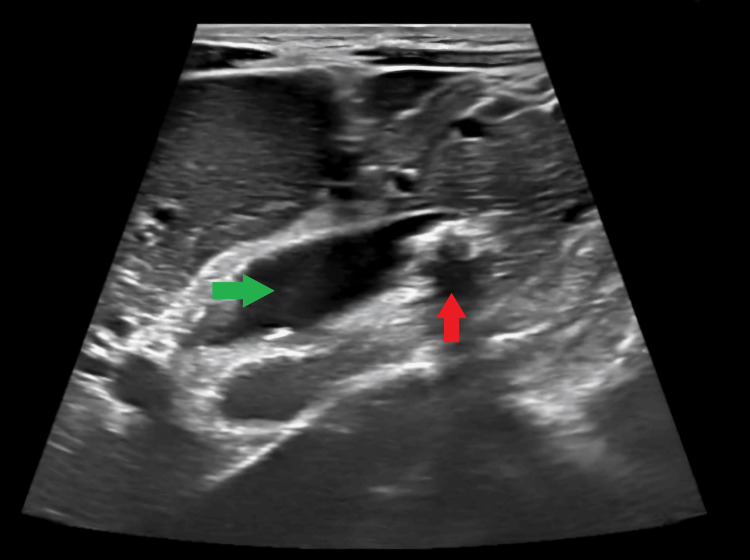 Figure 2
Figure 2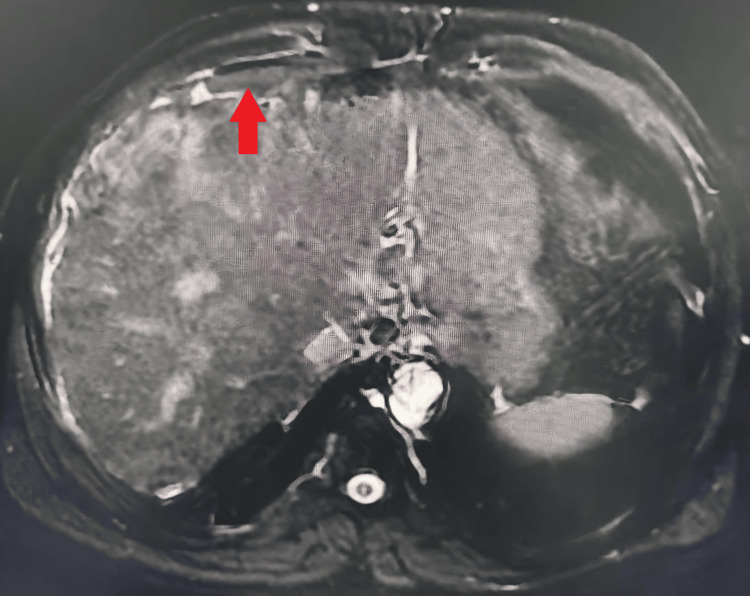 Figure 3
Figure 3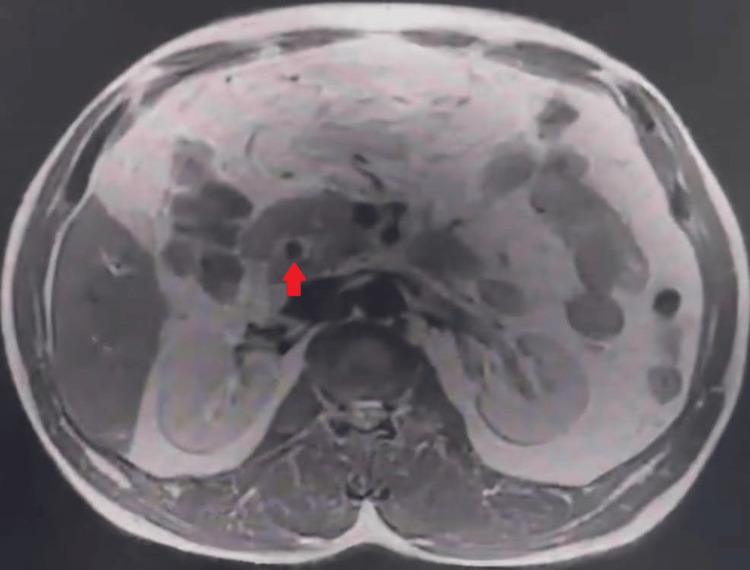 Figure 4
Figure 4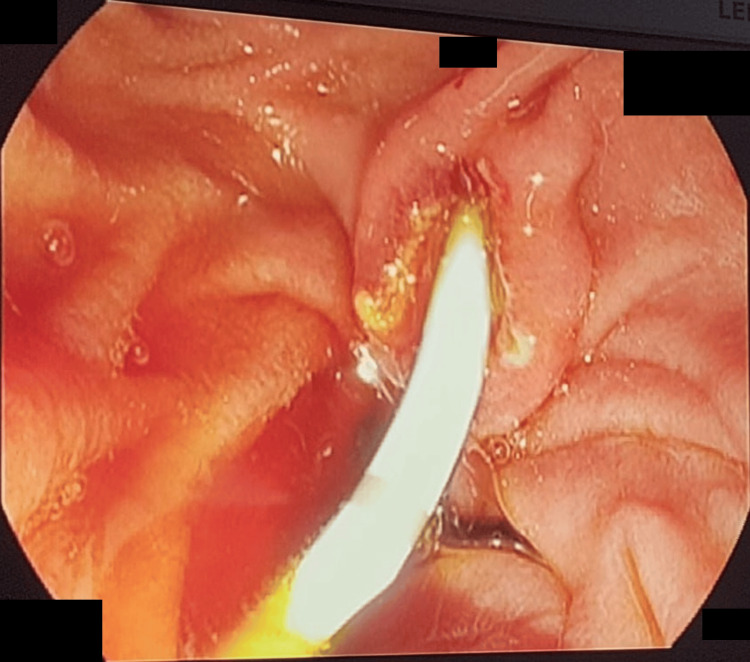 Figure 5
Figure 5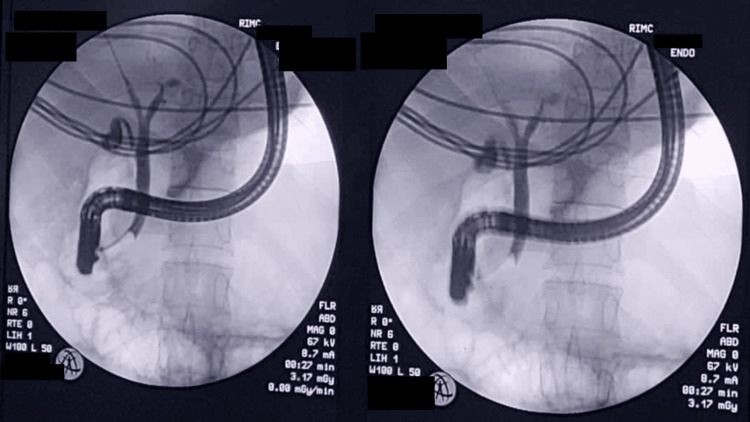 Figure 6
Figure 6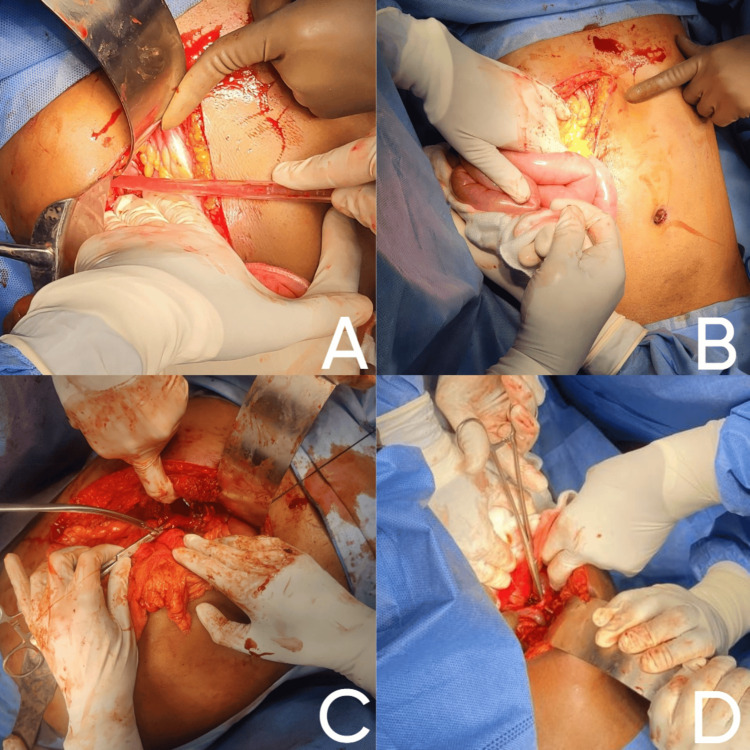 Figure 7
Figure 7 Figure 8
Figure 8 Figure 9
Figure 9 Figure 10
Figure 10| Test | Patient's value | Normal reference range |
| White blood cells (WBC) | 12,000/µL | 4,000-11,000/µL |
| Total bilirubin | 5.2 mg/dL | 0.1-1.2 mg/dL |
| Direct bilirubin | 3.1 mg/dL | 0.0-0.3 mg/dL |
| Alkaline phosphatase (ALP) | 240 U/L | 30-120 U/L |
| Aspartate aminotransferase (AST) | 80 U/L | 10-40 U/L |
| Alanine aminotransferase (ALT) | 60 U/L | 7-56 U/L |
| Amylase | 334 U/L | 30-110 U/L |
| Lipase | 380 U/L | 10-140 U/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Congenital Anomalies and Fetal Surgery · Organ Transplantation Techniques and Outcomes
Introduction
The gallbladder serves a vital function in bile storage and concentration, enabling efficient fat digestion and absorption [1]. Pathological conditions such as acute cholecystitis, choledocholithiasis, and cholangitis frequently require surgical management, with laparoscopic cholecystectomy remaining the preferred approach [2]. However, the contracted or "vanishing gallbladder" - characterized by severe fibrosis and anatomical distortion - presents significant diagnostic and operative challenges [3]. These complex cases typically result from chronic inflammation, metabolic disorders including diabetes mellitus, or advanced liver cirrhosis, all of which contribute to structural and functional gallbladder deterioration [4]. While preoperative imaging modalities like ultrasonography and magnetic resonance cholangiopancreatography (MRCP) are essential for surgical planning, intraoperative findings often necessitate procedural modifications, including conversion to open cholecystectomy [5]. This case report examines a 34-year-old male with multiple comorbidities, emphasizing the critical role of comprehensive clinical evaluation, advanced imaging interpretation, and multidisciplinary collaboration in managing contracted gallbladder pathology. The discussion highlights the importance of surgical adaptability and meticulous postoperative care to minimize complications such as bile duct injury or hemorrhage while simultaneously addressing underlying systemic conditions including cirrhosis and metabolic dysfunction.
Case presentation
A 34-year-old male, presented to the emergency department with a one-week history of severe right upper quadrant pain described as sharp and radiating to the back. He reported worsening abdominal distension noted by both himself and family members, along with visible jaundice characterized by yellowing of the sclera that prompted his hospital visit. Additional symptoms included high-colored urine indicative of bilirubin excretion and pale stools suggestive of obstructive jaundice. The patient reported two episodes of fever two weeks prior to presentation. Notably, there was no associated nausea, vomiting, melena, hematemesis, hematochezia, constipation, or diarrhea.
The patient's past medical history was significant for multiple comorbidities including type 2 diabetes mellitus diagnosed 10 years prior with suboptimal glycemic control, systemic hypertension managed with antihypertensive medications, and a history of acute calculus cholelithiasis treated conservatively in 2018. His cardiovascular history included coronary artery disease status post angioplasty in 2018 with ongoing antiplatelet therapy. Other notable conditions included dyslipidemia, chronic hepatitis B infection (HBsAg positive), and a 20-year history of chronic alcohol use. No significant family history of liver or gallbladder disease was reported.
On physical examination, the patient appeared icteric with stable vital signs (blood pressure (BP) of 130/85 mmHg, heart rate (HR) of 85 beats per minute (bpm)) but exhibited tachypnea (30 breaths/min). Abdominal examination revealed mild distension with a positive Murphy's sign. Palpation demonstrated tenderness in the right hypochondrium with guarding but no rigidity. Percussion detected minimal ascites with shifting dullness, and bowel sounds were present though diminished in intensity.
Initial laboratory investigations showed mild leukocytosis suggesting infection, while liver function tests revealed elevated total bilirubin with direct bilirubin predominance, alkaline phosphatase, and mildly elevated aspartate aminotransferase (AST) and alanine aminotransferase (ALT). Pancreatic enzymes were notably elevated, raising concern for pancreatitis or biliary obstruction (Table 1).
Imaging studies began with an erect abdominal X-ray which showed no signs of obstruction (Figure 1).
Erect abdominal X-ray showing no signs of obstruction
Abdominal ultrasound demonstrated early liver parenchymal disease, a 2 × 2 cm calculus at the distal common bile duct (CBD) causing proximal bile duct dilatation, a contracted gallbladder, and mild ascites (Figure 2).
Ultrasound of abdomen showing calculus at the distal common bile duct causing proximal bile duct dilatation. The green arrow shows the common bile duct, and the red arrow shows the calculi
MRCP further characterized the liver cirrhosis with nodularity and irregular contours, along with a dilated CBD containing multiple stones and a contracted gallbladder complicating potential laparoscopic access (Figures 3-4).
Magnetic resonance cholangiopancreatography (MRCP). The red arrow shows nodularity and irregular contours of liver surface
Magnetic resonance cholangiopancreatography (MRCP). The red arrow shows choledocholithiasis (gallstones within the common bile duct)
Subsequent endoscopic retrograde cholangiopancreatography (ERCP) confirmed CBD dilation with sludge but no large obstructing stones, leading to successful biliary sphincterotomy with sludge extraction and biliary stenting (Figures 5-6).
Endoscopic retrograde cholangiopancreatography (ERCP) showing common bile duct dilation with sludge but no large obstructing stones, leading to successful biliary sphincterotomy with sludge extraction
Endoscopic retrograde cholangiopancreatography (ERCP) showing biliary stenting (common bile duct plastic stenting)
The patient's initial management included intravenous fluids, broad-spectrum antibiotics for cholangitis, and opioid analgesics for pain control. Surgical intervention with attempted laparoscopic cholecystectomy was complicated by severe fibrosis and dense adhesions obscuring the gallbladder and dilated bowel loops, necessitating conversion to an open procedure. Intraoperative findings included significant scarring from previous inflammation and multiple black stones in the gallbladder bed. Only the gallbladder fundus was visualized, and the intrahepatic gallbladder was contracted. Gallbladder stones were retrieved. The anterior wall of the gallbladder was excised and sutured. Subtotal cholecystectomy was done (Figure 7).
Intraoperative imagesA) The right subcostal Kocher's incision was made. The abdomen opened in layers. The liver is retracted using a Deaver retractor.B) Dilated bowel loops; adhesions covering gallbladder fossa.C) Adhesiolysis, only the gallbladder fundus could be visualized.D) Contracted intrahepatic gallbladder fundus opened.
An intercostal drain (ICD) was placed and the abdomen was subsequently closed in layers (Figure 8).
Postoperative on-table image with intercostal drain (ICD) drain
The postoperative period was uneventful. The patient was started on appropriate intravenous fluids, antibiotics, analgesics, and other supportive measures. Ryle's tube (RT) was inserted. The patient gradually resumed oral intake, with successful recovery, and was discharged. The patient was on regular follow-up (Figures 9-10).
Tenth postoperative day follow-up imaging prior to suture removal
Thirtieth postoperative day follow-up imaging after suture removal
Discussion
The contracted gallbladder is a condition characterized by reduced size and function, which may result from chronic inflammation, repeated episodes of cholecystitis, or gallstone disease [6], with patients exhibiting chronic liver disease and portal hypertension being particularly susceptible to gallbladder atrophy due to impaired blood flow and biliary drainage [7]. The etiology is complex and multifactorial, involving chronic cholecystitis leading to fibrosis and scarring [8], nutritional factors like chronic alcohol use (as seen in this case) causing liver dysfunction and reduced motility [9], and metabolic conditions such as diabetes impacting gallbladder function and morphology [10]. While laparoscopic cholecystectomy is generally preferred for its advantages of lower morbidity, faster recovery, and reduced postoperative pain [11], cases with contracted gallbladders or significant inflammation often require conversion to open procedures due to challenges in visualization and access [12], with intraoperative decision-making being crucial to mitigate risks of bile duct injury, hemorrhage, or incomplete gallbladder removal, where surgical experience and adaptability significantly influence outcomes [13].
This case underscores the necessity of a multidisciplinary approach involving gastroenterologists, surgeons, and internists for optimal preoperative assessment, liver function monitoring, and timely management of complications like cholangitis or pancreatitis [14]. Postoperative recovery requires vigilant monitoring for potential complications, including surgical site infections (necessitating antibiotics), bile leaks (requiring drainage or reintervention), and intra-abdominal hemorrhage (potentially needing reoperation), particularly in patients with comorbidities like liver disease, with this patient being discharged after one week with instructions for liver function monitoring, infection surveillance, and lifestyle modifications, including dietary changes and alcohol cessation. Differential diagnosis must carefully consider acute cholecystitis (gallbladder inflammation from stone obstruction, supported by history and imaging), choledocholithiasis (CBD stones causing obstructive jaundice, evident on imaging), cholangitis (bile duct infection confirmed by clinical and laboratory findings), obstructive jaundice (secondary to biliary obstruction), and liver cirrhosis (with nodularity on imaging), as accurate differentiation is essential for appropriate treatment given the frequent symptom overlap that can complicate clinical assessment. This comprehensive understanding of contracted gallbladder pathology, from etiology through postoperative management, highlights the importance of thorough evaluation, adaptive treatment strategies, and multidisciplinary collaboration in optimizing patient outcomes.
Conclusions
This case highlights the complexities associated with diagnosing and managing a contracted gallbladder in the context of multiple comorbidities. A tailored approach, including thorough investigations and consideration of the patient's overall health status, is essential for optimal outcomes. The necessity for a multidisciplinary team is paramount in navigating the challenges presented by such complex cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dietary considerations in cholecystectomy: investigating the impact of various dietary factors on symptoms and outcomes Cureus Dahmiwal T Zade A Tote D Reddy S Sudabattula K 016202410.7759/cureus.61183 PMC 1120031438933619 · doi ↗ · pubmed ↗
- 2Physiology, gallbladder Stat Pearls [Internet] Jones MW Small K Kashyap S Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 482488/29494095 · pubmed ↗
- 3Contracted gallbladder: a finding in hepatic dysfunction Radiology Ferin P Lerner RM 7697701541985 https://pubmed.ncbi.nlm.nih.gov/3881796/388179610.1148/radiology.154.3.3881796 · doi ↗ · pubmed ↗
- 4Gallstones in patients with liver cirrhosis: incidence, etiology, clinical and therapeutical aspects World J Gastroenterol Acalovschi M 72777285202014 https://pubmed.ncbi.nlm.nih.gov/24966598/2496659810.3748/wjg.v 20.i 23.7277 PMC 4064073 · doi ↗ · pubmed ↗
- 5Assessment of predictors of difficult laparoscopic cholecystectomy by clinico-radiological parameters at a tertiary hospital in eastern India Cureus Toppo S Gaurav K Kumar K 016202410.7759/cureus.72512 PMC 1159963339606514 · doi ↗ · pubmed ↗
- 6Beware of the shrunken gallbladder - case report of intraoperatively diagnosed gallbladder agenesis Int J Surg Case Rep Anderson K Roland AL Miller MP Foretia DA 107588982022 https://pubmed.ncbi.nlm.nih.gov/36058154/3605815410.1016/j.ijscr.2022.107588 PMC 9482971 · doi ↗ · pubmed ↗
- 7Portal hypertension among patients with chronic liver disease admitted to the Department of Internal Medicine of a tertiary care centre JNMA J Nepal Med Assoc Khadka S Aryal A Karki S 779781612023 https://pubmed.ncbi.nlm.nih.gov/38289778/3828977810.31729/jnma.8294 PMC 10579770 · doi ↗ · pubmed ↗
- 8Risk factors for cholelithiasis Gastroenterol Nurs Pak M Lindseth G 297309392016 https://pubmed.ncbi.nlm.nih.gov/27467059/2746705910.1097/SGA.0000000000000235 PMC 8802735 · doi ↗ · pubmed ↗