Prevalence and risk factors of portal vein thrombosis following hepatectomy: a systematic review and meta‑analysis
Yang Qun, Feng Meiying, Yao Weiming, He Dan

TL;DR
This study finds that 9% of patients develop portal vein thrombosis after liver surgery, with cirrhosis and certain surgical factors increasing the risk.
Contribution
The study provides a meta-analysis of risk factors for portal vein thrombosis after hepatectomy, identifying key clinical predictors.
Findings
The pooled prevalence of portal vein thrombosis after hepatectomy is 9%.
Liver cirrhosis, portal vein resection, and right-sided hepatectomy are significant risk factors for PVT.
Prospective studies and larger sample sizes are associated with lower PVT prevalence rates.
Abstract
The prevalence and risk factors of portal vein thrombosis (PVT) are largely unclear, with an increasing number of studies reporting inconsistent results. The current study aimed to evaluate the prevalence and risk factors of PVT following hepatectomy through a systematic review and meta‑analysis. A comprehensive literature search was conducted across multiple databases (PubMed, Embase, and the Cochrane Library) to identify relevant studies. Prospective and retrospective studies reporting on PVT following hepatectomy were included. The Newcastle‑Ottawa Scale (NOS) was used to assess study quality, and the random effects model was used to analyze the prevalence and risk factors. A total of 15 studies involving 5145 patients were included in the current meta‑analysis. The pooled prevalence of PVT following hepatectomy was 9% (95% CI, 7%–12%) with substantial heterogeneity (I2 = 93.1%).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
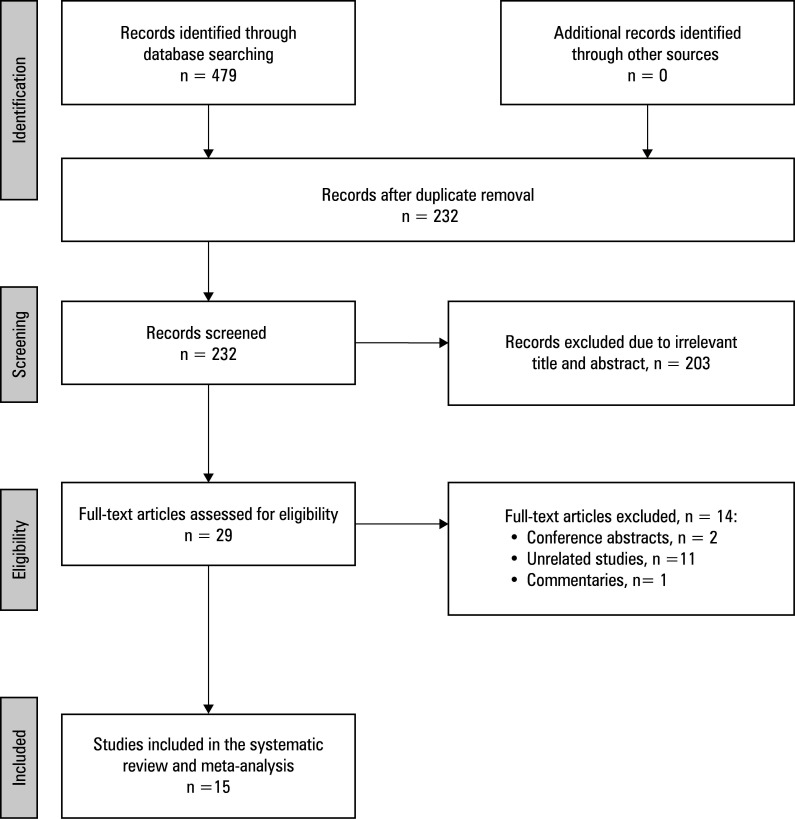 FIGURE 1
FIGURE 1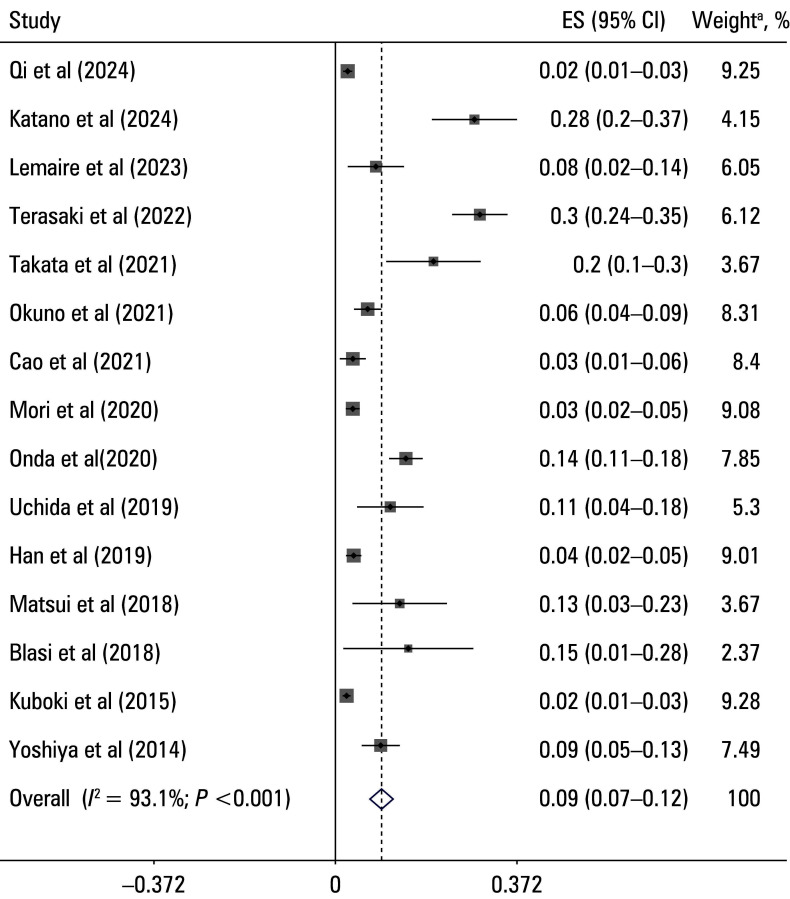 FIGURE 2
FIGURE 2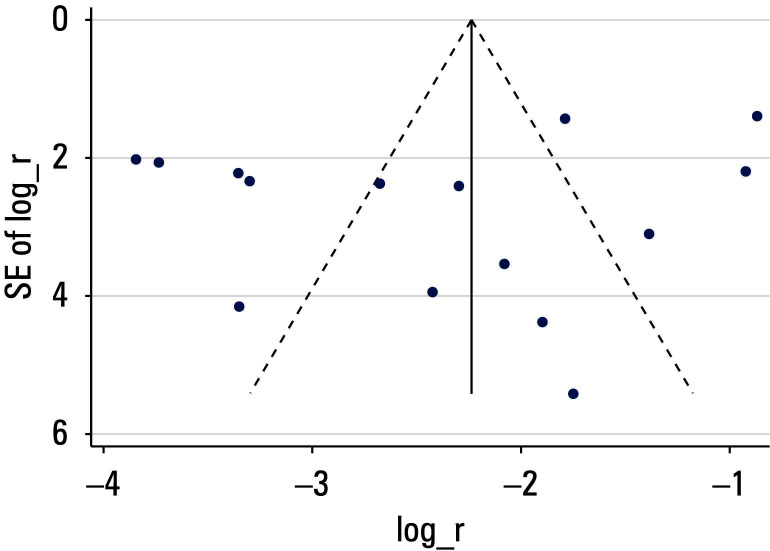 FIGURE 3
FIGURE 3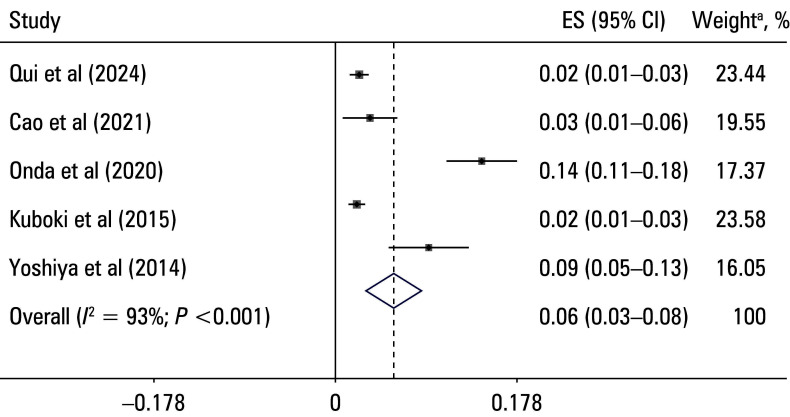 FIGURE 4
FIGURE 4| Study | Design | Country | Enrollment period | Age, y (SD or Range) | Sample size, n | Diagnosis | PVT detection method | Type of hepatectomy | Centers involved |
|---|---|---|---|---|---|---|---|---|---|
| Qi et al | Retrospective | China | 2018–2023 | 58 (11.6) | 1029 | NA | NA | Major (right/left) | Single-center |
| Katano et al | Retrospective | Japan | 2004–2021 | 68.5 (34–84) | 102 | NA | Contrast-enhanced CT | Hepatectomy and/or splenectomy | Single-center |
| Lemaire | Retrospective | France | 2012–2019 | 68 (48–76) | 86 | Perihilar cholangiocarcinoma | Doppler ultrasound or CT | Major hepatectomy | Single-center |
| Terasaki et al | Retrospective | Japan | 2009–2020 | 70 (35–83) | 247 | NA | Contrast-enhanced CT | Right hepatectomy, including cases with and without PVR | Single-center |
| Takata et al | Retrospective | Japan | 2014–2019 | 73 (38–93) | 65 | Hepatocellular carcinoma | Contrast-enhanced CT | Major or minor hepatectomy | Single-center |
| Okuno et al | Retrospective | Japan | 2015–2018 | 68 (20–87) | 295 | NA | Contrast-enhanced CT | Right-sided hepatectomy | Single-center |
| Cao et al | Retrospective | Japan | 2002–2018 | 68 (32–88) | 177 | Perihilar cholangiocarcinoma | Doppler ultrasound or CT | Major hepatectomy | Single-center |
| Onda et al | Retrospective | Japan | 2009–2019 | 63.6 (13.3) | 398 | Benign or malignant liver disease | Contrast-enhanced CT | Anatomical and partial hepatectomy | Single-center |
| Mori et al | Retrospective | Japan | 2006–2016 | 68.9 (9.9) | 622 | Primary liver cancer | Doppler ultrasound or CT | Laparoscopic and open hepatectomy | Single-center |
| Uchida et al | Retrospective | Japan | 2009–2016 | 72 (37–87) | 81 | Perihilar cholangiocarcinoma | Contrast-enhanced CT | Major hepatectomy with caudate lobectomy | Single-center |
| Han et al | Retrospective | Korea | 2009–2014 | 57.4 (13.1) | 534 | NA | NA | Major and minor hepatectomy | Single-center |
| Matsui et al | Prospective | Japan | 2012–2014 | NA | 81 | NA | Contrast-enhanced CT | Hepatectomy and/or splenectomy | Single-center |
| Blasi et al | Prospective | Spain | 2011–2014 | 64 (54–72) | 27 | Cholangiocarcinoma | NA | Major hepatectomy | Single-center |
| Kuboki et al | Retrospective | Japan | 2000–2013 | NA | 1193 | NA | Doppler ultrasound or CT | Major and minor hepatectomy | Single-center |
| Yoshiya et al | Retrospective | Japan | 2009–2012 | 66.7 (0.8) | 208 | Primary or metastatic liver tumors | Contrast-enhanced CT | Major hepatectomy | Single-center |
|
Study | a |
b |
c |
d |
e |
f |
g |
h |
i |
Score |
Overall quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Qi et al |
1 |
1 |
1 |
1 |
1 |
0 |
1 |
1 |
1 |
8 |
High |
|
Katano et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Lemaire et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Terasaki et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Takata et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Okuno et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Cao et al |
1 |
1 |
1 |
1 |
1 |
0 |
1 |
1 |
0 |
7 |
High |
|
Onda et al |
1 |
1 |
1 |
1 |
1 |
0 |
1 |
1 |
1 |
8 |
High |
|
Mori et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Uchida et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Han et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Matsui et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Blasi et al |
1 |
1 |
1 |
1 |
0 |
0 |
1 |
1 |
0 |
6 |
Moderate |
|
Kuboki et al |
1 |
1 |
1 |
1 |
1 |
0 |
1 |
1 |
1 |
8 |
High |
|
Yoshiya et al |
1 |
1 |
1 |
1 |
1 |
0 |
1 |
1 |
0 |
7 |
High |
|
Outcomes |
Number of studies |
OR (95% CI) |
Heterogeneity, |
|---|---|---|---|
|
Pooled results |
15 |
0.09 (0.07–0.12) |
93.1 |
|
Study design | |||
|
Prospective studies |
2 |
0.14 (0.06–0.22) |
0 |
|
Retrospective studies |
13 |
0.09 (0.07–0.11) |
93.9 |
|
Sample size | |||
|
More than 500 |
4 |
0.026 (0.019–0.033) |
29.9 |
|
Less than 500 |
9 |
0.014 (0.09– 0.19) |
90.4 |
|
Study quality (NOS score) | |||
|
High (≥8 points) |
3 |
0.05 (0.02–0.09) |
95.7 |
|
Low / moderate (<8 points) |
12 |
0.11 (0.08–0.15) |
91.6 |
|
Type of surgery | |||
|
Hepatectomy |
13 |
0.08 (0.06–0.1) |
92.9 |
|
Simultaneous splenectomy and hepatectomy |
2 |
0.21 (0.06–0.36) |
81.2 |
|
Study region | |||
|
Asia |
13 |
0.09 (0.07–0.12) |
91.57 |
|
Europe |
2 |
0.09 (0.04–0.14) |
0 |
|
Excluded study |
Estimate |
95% CI |
|---|---|---|
|
Qi et al |
0.105 |
0.075–0.134 |
|
Katano et al |
0.083 |
0.06–0.106 |
|
Lemaire et al |
0.094 |
0.069–0.118 |
|
Terasaki et al |
0.074 |
0.0536–0.093 |
|
Takata et al |
0.088 |
0.0645–0.112 |
|
Okuno et al |
0.096 |
0.0708–0.121 |
|
Cao et al |
0.099 |
0.0736–0.125 |
|
Onda et al |
0.086 |
0.063–0.109 |
|
Mori et al |
0.101 |
0.0742–0.129 |
|
Uchida et al |
0.092 |
0.067–0.116 |
|
Han et al |
0.101 |
0.074–0.127 |
|
Matsui et al |
0.091 |
0.0672–0.116 |
|
Blasi et al |
0.092 |
0.068–0.116 |
|
Kuboki et al |
0.105 |
0.0755–0.134 |
|
Yoshiya et al |
0.093 |
0.068–0.118 |
| Risk factor | Number of studies | Pooled OR (95% CI) | Heterogeneity, I2, % |
|---|---|---|---|
| Liver cirrhosis | 2 | 5.177 (1.853–14.47) | 0 |
| Operative time | 4 | 1.001 (0.995–1.007) | 29.78 |
| Blood loss | 2 | 1.003 (0.902–1.115) | 0 |
| Portal vein resection | 2 | 5.07 (2.204–11.661) | 30.93 |
| Right-sided hepatectomy | 3 | 6.259 (1.8–21.761) | 61.69 |
| Pringle maneuver use | 2 | 1.65 (0.759–3.589) | 75.28 |
| Postoperative PV angle | 2 | 15.63 (3.22–75.88) | 0 |
| Remnant PV diameter | 2 | 4.6 (0.39–54.73) | 83.49 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Hepatocellular Carcinoma Treatment and Prognosis · Liver Disease Diagnosis and Treatment
INTRODUCTION
Portal vein thrombosis (PVT) is a significant yet often underrecognized complication of hepatectomy, with substantial clinical implications for patient outcomes.1^,^2 Hepatectomy is a cornerstone treatment for various liver conditions, including hepatocellular carcinoma and metastatic liver tumors.3 Despite the proven efficacy of hepatectomy in treating these conditions, potential complications, such as PVT, pose serious challenges.4^,^5 PVT can lead to compromised liver function, impaired regeneration, prolonged hospital stay, and increased postoperative mortality.1 Thus, there is a critical need for a deeper understanding of its prevalence and risk factors to guide clinical practice and improve patient care.
The reported incidence of PVT after hepatectomy varies considerably. This variation is largely attributed to differences in patient characteristics, surgical techniques, and study methodologies. Specific subgroups of patients, such as those undergoing extended hepatectomy or those with underlying liver cirrhosis, are at a particularly high risk of developing PVT.4^,^6^,^7 For instance, individuals with liver cirrhosis experience altered portal hemodynamics and hypercoagulability, which significantly increase their susceptibility to PVT.8^,^9 These factors complicate perioperative management and underscore the need for a comprehensive evaluation of the PVT incidence and its determinants.10 A standardized approach to assessing and reporting PVT incidence could contribute to a clearer understanding of this complication across different patient populations.
Several risk factors for PVT following hepatectomy have been proposed, with liver cirrhosis consistently emerging as a major predictor due to its impact on hepatic vasculature and the overall coagulation profile.11 Patients with cirrhosis may develop a hypercoagulable state caused by imbalanced pro‑ and anticoagulant factors, as well as endothelial dysfunction, all of which increase the risk of thrombosis.12^,^13 Apart from liver cirrhosis, intraoperative factors, such as blood transfusion, prolonged operative time, and specific surgical techniques (eg, portal vein resection [PVR]) have been linked to an increased PVT risk.4^,^5^,^14 Blood transfusions may contribute to a proinflammatory and hypercoagulable state, thereby exacerbating the risk of PVT. The invasive nature of PVR, which often involves extensive vascular manipulations, is associated with endothelial damage, a key factor predisposing patients to thrombus formation.14^,^15^,^16 Prolonged use of the Pringle maneuver, during which blood flow to the liver is temporarily occluded, can also exacerbate ischemia‑reperfusion injury, further increasing the likelihood of PVT.17^,^18 Understanding these risk factors is crucial for informing perioperative decision‑making and improving patient outcomes. Mitigating the risk of PVT requires targeted perioperative interventions.1 Perioperative anticoagulation is an important consideration for high‑risk patients, such as those with liver cirrhosis or those undergoing extensive vascular procedures.19^,^20 However, anticoagulation in these patients must be carefully balanced against the concurrent risk of bleeding.20^,^21 Proactive identification of modifiable risk factors and tailoring perioperative care to individual patient needs are essential for minimizing the incidence of PVT, reducing postoperative morbidity, and improving overall outcomes.
AIM
The objective of this systematic review and meta‑analysis was to estimate the pooled prevalence of PVT following hepatectomy and to identify key risk factors validated through multivariable or adjusted analyses. By consolidating the available evidence, we aimed to provide actionable insights into the prevention and management of PVT, ultimately contributing to improved clinical outcomes of patients undergoing hepatectomy.
MATERIALS AND METHODS
Study design This systematic review and meta‑analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta‑Analyses guidelines.22 The primary objective was to estimate the prevalence of PVT following hepatectomy and to identify the risk factors for its occurrence.
Search strategy
A comprehensive literature search was performed across multiple databases (PubMed, Embase, and the Cochrane Library) to identify relevant studies published since the database inception until August 7, 2024, without language restrictions. The search strategy used a combination of Medical Subject Headings terms and relevant key words, such as portal vein thrombosis, hepatectomy, liver surgery, prevalence, and risk factors, and their variants. Reference lists of the retrieved articles were manually screened to identify any additional studies that met the inclusion criteria.
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: 1) reported quantitative data on the prevalence of PVT or included a multivariable or adjusted analysis of risk factors associated with PVT following hepatectomy; 2) involved adult patients undergoing hepatectomy for any indication; 3) were original research articles, including observational studies (eg, cohort, cross‑sectional, and case‑control studies).
Studies were excluded if they were case reports, letters, conference abstracts, reviews, or animal studies, or if they lacked sufficient data on PVT prevalence or associated risk factors.
Data extraction and management
Two independent reviewers (FM and YW) extracted data using a standardized data extraction form. The extracted data included study characteristics (author, year of publication, country), patient demographics (age, sex, presence of liver cirrhosis), surgical details (type of hepatectomy, PVR, Pringle maneuver duration), and outcomes (prevalence of PVT, identified risk factors, and effect estimates). Any disagreements between the reviewers were resolved through discussion or by consulting a third reviewer (HD). The EndNote soft‑ ware (Clarivate, Philadelphia, Pennsylvania, United States) was used for reference management.
PRISMA flow diagram of the study selection process
Quality assessment
The quality of the included papers was assessed using the Newcastle‑Ottawa Scale (NOS) for observational studies.23 The NOS evaluates study quality across 3 domains: selection of study groups, comparability of groups, and assessment of outcomes.23 Each study was as‑ signed a score of up to 9 points, with higher scores indicating better quality. We assigned scores of 0 to 3, 4 to 6, and 7 to 9 for low, moderate, and high quality of studies, respectively.
Statistical analysis
This meta‑analysis was performed to evaluate the pooled prevalence (primary outcome) and risk factors (secondary outcomes) of PVT following hepatectomy. Event rates and their corresponding 95% CIs were extracted or calculated from the included studies for prevalence estimation. To stabilize variance and normalize the distribution, log‑transformed prevalence rates and SEs were used. The pooled prevalence was calculated using the DerSimonian–Laird random effects model to account for the expected heterogeneity across studies. Heterogeneity was assessed using the Cochrane Q test and quantified by the I^2^ statistic, with I^2^ greater than 50% indicating substantial heterogeneity.24 Subgroup analyses were conducted based on study design, sample size, study quality, type of surgery, and geographic region to explore potential sources of heterogeneity. The leave‑one‑out sensitivity analyses were performed by sequentially excluding individual studies to evaluate the robustness of the overall results. We also performed sensitivity analyses through excluding low‑quality studies (based on the risk of bias assessment) to evaluate their impact on the overall pooled effect estimate. For the risk factors, odds ratios (ORs) with their 95% CIs were extracted, and log‑transformed ORs and SEs were computed for each study. The random effects model was used for all meta‑analyses due to the substantial heterogeneity observed among the included studies. Publication bias was evaluated using funnel plots and the Egger or Begg regression test, with a P value below 0.05 indicating significant publication bias.25 If a bias was detected, the trim‑and‑fill method was applied to adjust the pooled effect size.26 All statistical analyses were performed using the Stata software, version 12.0 (StataCorp, College Station, Texas, United States).
Ethical approval
This study did not require approval of a bioethics committee.
RESULTS
Study selection A comprehensive literature search yielded 479 records. After removal of duplicates, the remaining 232 records were screened based on the title and abstract, leading to the exclusion of 203 articles. Subsequently, 29 full‑text articles were assessed for eligibility, and 14 were excluded for the following rea‑ sons: conference abstracts (n = 2), unrelated studies (n = 11), and commentaries (n = 1). Ultimately, 15 studies met the inclusion criteria and were included in the systematic review and meta‑analysis4^,^5^,^14^,^17^,^18^,^27^,^28^,^29^,^30^,^31^,^32^,^33^,^34^,^35^,^36 FIGURE 1 .
Characteristics of the included studies
General characteristics of the included studies are summarized in TABLE 1. The studies were conducted across 5 countries, with a majority having been carried out in Japan (n = 11). The remaining 4 studies were conducted in China, Korea, France, and Spain. Sample sizes ranged from 27 to 1193 patients, with study enrollment periods spanning from 2000 to 2023. Most of the included studies were retrospective (n = 13), while 2 were prospective.27, 31 The primary methods of PVT detection were contrast‑enhanced computed tomography and Doppler ultrasound.
The quality of the included studies was assessed using the NOS criteria TABLE 2. Overall quality scores ranged from 6 to 8, with 5 studies rated to be of high quality,5^,^17^,^28^,^30^,^36 and the remaining ones rated to be of moderate quality.4^,^14^,^18^,^27^,^29^,^31^,^32^,^33^,^34^,^35 Most studies demonstrated good representative‑ ness of the cohort and appropriate selection of controls; however, limitations in controlling for confounders and the adequacy of follow‑up were noted, potentially affecting the robustness of the findings.
Pooled prevalence of portal vein thrombosis
The overall pooled prevalence of PVT following hepatectomy was 9% (95% CI, 7%–12%), as depicted in FIGURE 2. Substantial heterogeneity was observed among the included studies (I2 = 93.1%). The prevalence estimates in individual studies ranged from 2% to 30%, reflecting considerable variability in the reported rates of PVT.
To explore potential sources of heterogeneity, subgroup analyses were conducted based on study design, sample size, study quality, type of surgery, and study region TABLE 3. The pooled prevalence of PVT was higher in the prospective studies (OR, 0.14; 95% CI, 0.06–0.22), as compared with the retrospective ones (OR, 0.09; 95% CI, 0.07–0.11). Notably, no heterogeneity was observed among the prospective studies (I^2^ = 0%), whereas substantial heterogeneity was noted among the retrospective ones (I^2^ = 93.9%). The studies with a sample sizes greater than 500 reported a lower prevalence of PVT (OR, 0.026; 95% CI, 0.019–0.033; I^2^ = 29.9%) than those with smaller sample sizes (OR, 0.014; 95% CI, 0.09–0.19; I^2^ = 90.4%). The studies with NOS scores of 8 or more demonstrated a lower prevalence of PVT (OR, 0.05; 95% CI, 0.02–0.09), as compared with those with lower scores (OR, 0.11; 95% CI, 0.08–0.15), with high heterogeneity observed in both subgroups, particularly in the high‑quality group (I^2^ = 95.7%). The prevalence of PVT was also higher in the patients undergoing simultaneous splenectomy and hepatectomy (OR, 0.21; 95% CI, 0.06–0.36; I^2^ = 81.2%), as compared with those undergoing hepatectomy alone (OR, 0.08; 95% CI, 0.06–0.1). The studies conducted in Asia reported a pooled PVT prevalence of 9% (95% CI, 7%–12%; I^2^ = 91.57%), while the European studies reported a similar prevalence (OR, 0.09; 95% CI, 0.04–0.14) but with no heterogeneity (I^2^ = 0%).
Forest plot of the prevalence of portal vein thrombosis following hepatectomy
Sensitivity analysis and publication bias
A leave one‑out sensitivity analysis was performed to evaluate the robustness of the pooled prevalence estimate TABLE 4. The results indicated that no single study significantly influenced the overall estimate, which remained stable at approximately 9% to 12%, suggesting robustness of the findings. We also performed sensitivity analyses involving exclusion of lower‑quality studies to evaluate their impact on the overall pooled effect, and the result showed that the pooled prevalence of PVT following hepatectomy was 6% (95% CI, 3%–8%) in the included studies of high quality FIGURE 3. To assess the potential publication bias, a funnel plot was constructed FIGURE 4. Visual inspection suggested some potential asymmetry, but statistical analysis (Egger test: P = 0.62) indicated no significant evidence of a publication bias.
Risk factors for portal vein thrombosis
The pooled ORs for various risk factors associated with PVT are presented in TABLE 5. Liver cirrhosis was significantly associated with an increased risk of PVT (OR, 5.18; 95% CI, 1.85–14.47; I^2^ = 0%). The patients undergoing PVR also had an elevated risk of PVT (OR, 5.07; 95% CI, 2.2–11.66; I^2^ = 30.93%). Right‑sided hepatectomy was significantly associated with a higher risk of PVT (OR, 6.26; 95% CI, 1.8–21.76; I^2^ = 61.69%). Moreover, a wider post‑ operative portal vein angle was strongly associated with an increased PVT risk (OR, 15.63; 95% CI, 3.22–75.88; I^2^ = 0%).
Other factors, such as operative time (OR, 1.001; 95% CI, 0.995–1.007; I^2^ = 29.78%), blood loss (OR, 1.003; 95% CI, 0.902–1.115; I^2^ = 0%), Pringle maneuver use (OR, 1.65; 95% CI, 0.76–3.59; I^2^ = 75.28%), and remnant portal vein diameter (OR, 4.6; 95% CI, 0.39–54.73; I^2^ = 83.49%) did not show significant associations with the PVT risk.
DISCUSSION
This meta‑analysis provides a comprehensive evaluation of the prevalence and risk factors of PVT following hepatectomy. We showed that despite relatively low prevalence (9%), PVT is a significant postoperative complication with substantial implications for patient outcomes. The most critical risk factors identified were liver cirrhosis, PVR, right‑sided hepatectomy, and widened postoperative portal vein angle. These findings emphasize the need for careful patient selection, perioperative planning, and close post‑ operative monitoring in high‑risk populations.
The pooled prevalence of PVT following hepatectomy was estimated at 9%, with substantial heterogeneity. The variation in prevalence, ranging from 2% to 30%, may reflect differences in study design, surgical expertise, and patient characteristics, highlighting the need for standardized diagnostic criteria and protocols. Our finding that liver cirrhosis significantly increased PVT risk, which is consistent with earlier reports, underscores the association between hypercoagulable state and cirrhosis mediated by portal hypertension, impaired liver function, and endothelial dysfunction.37^,^38 Similarly, the high risk associated with PVR is in line with prior studies indicating that extensive vascular manipulation elevates the thrombotic risk due to endothelial injury.15^,^16 These results emphasize the importance of vigilant postoperative management in these high‑risk groups. The identified risk factors for PVT, including liver cirrhosis, PVR, right‑sided hepatectomy, and widened postoperative portal vein angle, reflect the clinically relevant underlying biological mechanisms. Cirrhosis contributes to hypercoagulable state, highlighting the need for enhanced monitoring and potential low‑dose anticoagulation to prevent PVT, despite the inherent bleeding risk.20^,^39^,^40 The increased PVT risk with PVR and right‑sided hepatectomy likely results from vascular disruption and altered portal flow dynamics. Minimizing endothelial injury and maintaining optimal venous flow are essential strategies to reduce the PVT risk.1 The strong association between a widened portal vein angle and PVT suggests that anatomical alterations may lead to venous stasis, necessitating surgical approaches that preserve optimal portal vein alignment. These findings support tailored perioperative interventions, such as anticoagulation and careful monitoring in high‑risk patients. Further studies should focus on optimizing surgical techniques and evaluating prophylactic measures to reduce the incidence of PVT and improve patient outcomes.
This meta‑analysis has several strengths, including a large pooled sample size, robust statistical methodologies, and a comprehensive assessment of both patient‑related and procedural risk factors for PVT. These strengths enhance the generalizability of our findings and provide valuable insights for both clinicians and researchers seeking to mitigate the PVT risk after hepatectomy.
Funnel plot for assessing publication bias
Forest plot of the prevalence of portal vein thrombosis following hepatectomy after removing lower‑quality studies
However, certain limitations must be acknowledged. Firstly, we observed substantial heterogeneity across the included studies. Heterogeneity is a common challenge in systematic reviews, particularly when studies vary in clinical settings, patient populations, and diagnostic criteria. To explore potential sources of heterogeneity, we conducted subgroup analyses based on various factors. However, we were unable to identify any single factor that fully accounted for the observed heterogeneity. Also, the leave‑one‑out sensitivity analysis showed that omitting any individual study did not significantly affect the overall pooled effect. Understandably, these analyses suggest that heterogeneity is likely multifactorial and cannot be easily resolved through subgroup or sensitivity analyses alone. Consistently, sensitivity analyses involving exclusion of lower‑quality studies did not substantially alter the effect estimate. Consequently, despite the inherent variability among studies, the consistency of our findings across multiple analyses supports the robustness and reliability of the overall pooled effect estimate. Additionally, while a publication bias was not detected through statistical testing, it is hard to completely rule it out since the funnel plot seems to be asymmetrical. Finally, the predominance of retrospective and moderate‑quality studies also introduces potential biases, such as selection bias, which may affect the validity of our findings.
Future research should prioritize prospective, multicenter studies with standardized definitions and diagnostic criteria for PVT. This would enhance comparability of the data and provide a more accurate estimate of PVT prevalence. Moreover, clinical trials are needed to evaluate the efficacy and safety of prophylactic anticoagulation in high‑risk populations, such as patients with liver cirrhosis or those undergoing extensive vascular resection. The role of postoperative anatomical changes, particularly portal vein angle, in PVT development also warrants further investigation. Understanding the impact of surgical modifications on vascular dynamics may offer new strategies to prevent thrombosis. Finally, the relationship between intraoperative factors (eg, blood transfusion) and PVT remains an area for further study, particularly in the context of optimizing transfusion protocols to balance the risks of bleeding and thrombosis.
CONCLUSIONS
PVT remains a significant complication following hepatectomy, particularly in the patients with liver cirrhosis, those undergoing PVR, and those with notable postoperative anatomical changes. Identifying these risk factors allows for targeted perioperative interventions that may reduce the incidence of PVT and improve overall patient outcomes. Future research should aim to validate these findings through well‑designed prospective studies and to explore preventive measures, including individualized anticoagulation strategies, to further enhance postoperative care for high‑risk patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Portal vein thrombosis: di‐ agnosis, management, and endpoints for future clinical studies Lancet Gas‐ troenterol Hepatol 9 Elkrief L. Hernandez‐Gea V. Senzolo M. 2024859883859-88310.1016/S 2468-1253(24)00155-938996577 · doi ↗ · pubmed ↗
- 2Imaging in clinical decision‐making for portal vein thrombosis Nat Rev Gastroenterol Hepatol 11 Berzigotti A. García‐Criado A. Darnell A. García‐Pagán J.C. 2014308316308-3162441939510.1038/nrgastro.2013.258 · doi ↗ · pubmed ↗
- 3Guidelines for the diagnosis and treatment of hepatocellular carcinoma (HCC) in adults Gut 52 Suppl 3 Ryder S.D. 2003181-81269214810.1136/gut.52.suppl_3.iii 1PMC 1867754 · doi ↗ · pubmed ↗
- 4Predictors of portal vein thrombo‐ sis after simultaneous hepatectomy and splenectomy: a single‐center retro‐ spective study Asian J Surg 47 Katano K. Nakanuma S. Araki T. 2024513751425137-51423905415410.1016/j.asjsur.2024.07.131 · doi ↗ · pubmed ↗
- 5Analysis of related influencing factors of por‐ tal vein thrombosis after hepatectomy J Laparoendosc Adv Surg Tech A 34 Qi S. Tao J. Wu X. 2024246250246-2503825255710.1089/lap.2023.0455 · doi ↗ · pubmed ↗
- 6Metabolic dysfunction‐associated steatotic liver disease related cirrhosis and incidence of portal vein thrombosis Eur J Gastroenterol Hepatol 36 Amjad W. Jiang Z.G. Lai M. 2024103810451038-10453882995010.1097/MEG.0000000000002800 · doi ↗ · pubmed ↗
- 7Platelet activation is upregulated in cir‐ rhotic patients with portal vein thrombosis Thromb Haemost 124 Zhao F. Ding J. Cui J. 2024739752739-7523782750710.1055/a-2190-8705 · doi ↗ · pubmed ↗
- 8Clinical characteristics and predictors of benign portal vein thrombosis in patients with liver cirrho‐ sis: a retrospective single‐center study Medicine (Baltimore 103 Arabpour E. Hatami B. Pasharavavesh L. 20243982310.1097/MD.0000000000039823 PMC 1141942339312324 · doi ↗ · pubmed ↗