Feasibility analysis and efficacy evaluation of computed tomography–guided microwave ablation combined with radioactive 125I particles in the treatment of lung nodules
Yu‑Qing Shan, Fan‑Xia Lin, Li Wang, Hai‑Yu Wang

TL;DR
This study shows that combining microwave ablation with radioactive particle implantation for lung nodules is safe and effective without increasing complications.
Contribution
The study demonstrates the feasibility and safety of combining MWA with 125I seed implantation for treating lung nodules.
Findings
Both groups had 100% local control at 3 and 6 months.
Complication rates were similar between the experimental and control groups.
The experimental group had a slightly higher effective rate at 6 months.
Abstract
Lung cancer is one of the leading causes of mortality worldwide and it requires early detection and treatment. Microwave ablation (MWA), a minimally invasive technique, is effective in early stages of lung cancer, but may cause complications when applied near sensitive structures. Such cases require the use of 125I seed implantation. Our study retrospectively analyzed 58 lung nodule patients treated with MWA in combina- tion with simultaneous or delayed radioactive particle implantation to evaluate the impact of implant radiation therapy on patient outcomes and complicaton rates. The aim of this study was to evaluate the feasibility of MWA combined with 125I seed implantation for treating ipsilateral single pulmonary nodules. This retrospective study included 58 patients who underwent computed tomography (CT)-guided percutaneous pulmonary biopsy of ipsilateral single nodules combined…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
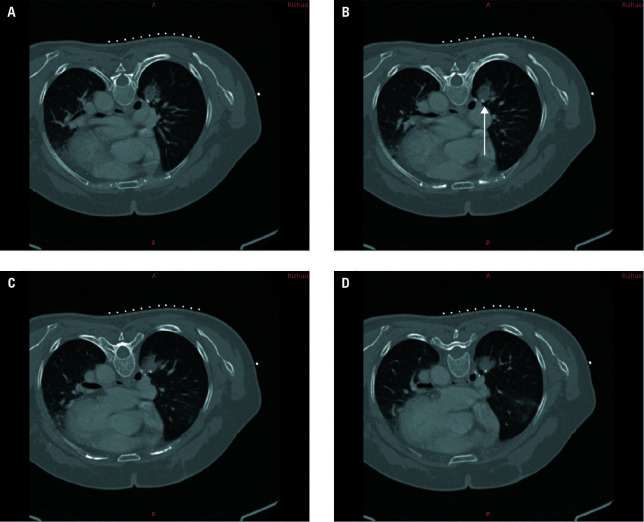 FIGURE 1
FIGURE 1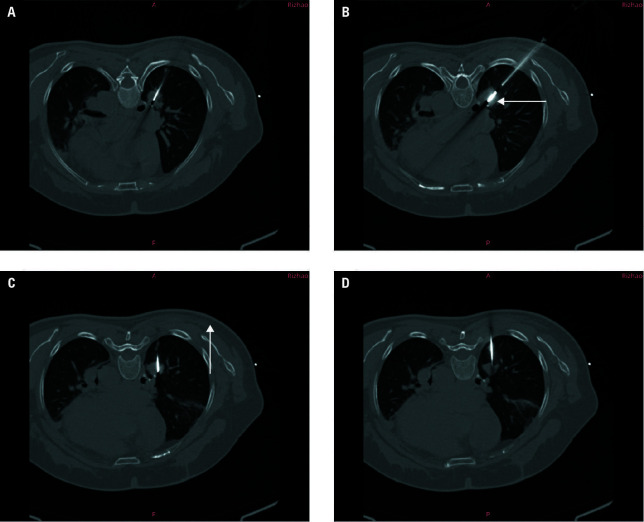 FIGURE 2
FIGURE 2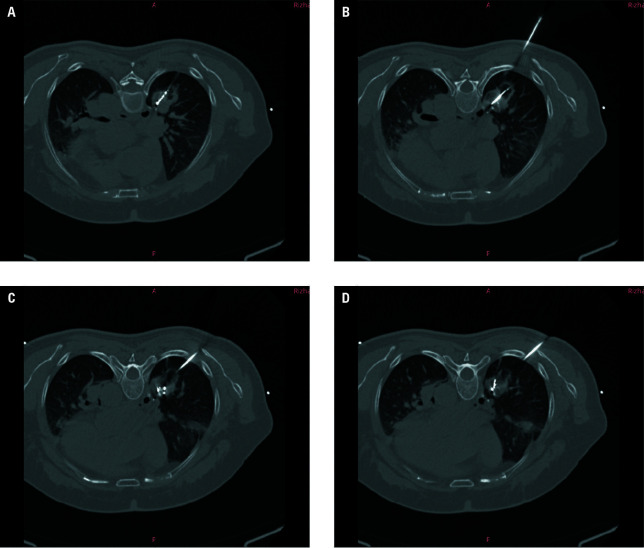 FIGURE 3
FIGURE 3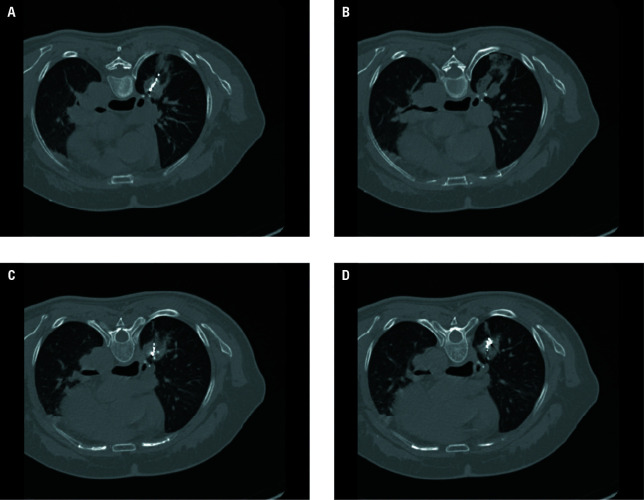 FIGURE 4
FIGURE 4| Parameter |
Control group (n = 30) |
Experimental group (n = 28) |
| |
|---|---|---|---|---|
| Age, y, mean (SD) |
66.33 (6.42) |
64.39 (7.17) |
0.89 | |
| Sex | Men |
18 (60) |
19 (67.9) |
0.53 |
| Women |
2 (40) |
9 (32.1) | ||
| BMI, kg/m2, mean (SD) |
23.80 (3.1) |
23.99 (2.82) |
0.62 | |
| Smoker |
8 (26.7) |
9 (32.1) |
0.19 | |
| Pathological type | Squamous cell carcinoma |
21 (70) |
9 (30) |
0.46 |
| Adenocarcinoma |
17 (60.7) |
11 (39.3) | ||
| TNM staging | Phase III |
26 (86.7) |
4 (13.3) |
0.26 |
| Phase IV |
21 (75) |
7 (25) |
| Complications |
Control group (n = 30) |
Experimental group (n = 28) |
|
|---|---|---|---|
| Pneumothorax |
5 (16.67) |
4 (14.28) |
0.8 |
| Pleural effusion |
3 (10) |
2 (7.14) |
0.7 |
| Hemoptysis |
4 (13.33) |
3 (10.71) |
0.76 |
| Duration of hospitalization, d, mean (SD) |
7.97 (0.93) |
4.54 (1.29) |
0.03 |
| Follow-up time point |
Control group (n = 30) |
Experimental group (n = 28) | |
|---|---|---|---|
| One month | |||
| CR |
16 (53.3) |
17 (60.7) | 0.61 |
| PR |
8 (26.7) |
6 (21.4) | |
| SD |
6 (20) |
5 (17.9) | |
| PD |
0 |
0 | |
| Three months | 0.67 | ||
| CR |
25 (83.3) |
23 (82.1) | |
| PR |
5 (16.7) |
5 (17.9) | |
| SD |
0 |
0 | |
| PD |
0 |
0 | |
| Six months |
0.84 | ||
| CR |
28 (93.3) |
27 (96.4) | |
| PR |
2 (6.7) |
1 (3.6) | |
| SD |
0 |
0 | |
| PD |
0 |
0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Gyrotron and Vacuum Electronics Research · Particle accelerators and beam dynamics
INTRODUCTION
Despite lung cancer ranking second in incidence globally, it remains one of the leading causes of mortality, which is why ear‑ ly detection, diagnosis, and treatment are cru‑ cial in treating it.1 Local thermal ablation, a precise and minimally invasive technique, has been increasingly employed in the treatment of early lung cancer with the annual number of treated cases rapidly rising.2^,^3 This technique boasts min‑ imal trauma, clear efficacy, high safety, strong re‑ producibility, and broad applicability across dif‑ ferent patient populations. However, microwave ablation (MWA) of nodules adjacent to the pleu‑ ra and pericardium may lead to complications, such as vagal nerve reactions and massive bleed‑ ing. This therapy achieves ultrahigh radiation dos‑ es within the tumor target area, while the dose around the target rapidly diminishes resulting in minimal exposure of normal tissues and sur‑ rounding organs.4 Therefore, ^125^I seed implanta‑ tion has gained widespread recognition as an ef‑ fective treatment for lung nodules. In this study, we retrospectively analyzed the occurrence of postoperative complications and short‑term ef‑ ficacy at 1‑, 3‑, and 6‑month follow‑ups in 58 pa‑ tients with lung nodules who underwent MWA therapy either simultaneously or selectively com‑ bined with particle implantation therapy.
AIM
The aim of this study was to evaluate the feasibility of MWA combined with particle implantation for treating ipsilateral single pulmonary nodules.
MATERIALS AND METHODS
Patients and procedure
A retrospective analysis was conducted on the clinical and follow‑up data of 58 patients with lung nodules who underwent percutaneous lung puncture thermal ablation, either simultaneously or selectively combined with par‑ ticle implantation at the Medical Imaging Centre of Rizhao People’s Hospital between January 2022 and December 2024. Among these patients, 37 were men and 21 were women aged from 28 years to 76 years. All of them had previously un‑ dergone lung biopsy confirming their lung nod‑ ule lesions as malignant. A randomization meth‑ od was used to divide the patients into 2 groups: an MWA combined with particle implantation group (experimental group) which included 28 participants and an MWA selective particle im‑ plantation group (control group) which consist‑ ed of 30 participants.
Inclusion criteria concerned patients meet‑ ing the following conditions: 1) maximum lesion diameter of ≤3 cm; 2) inability to tolerate gen‑ eral anesthesia or surgical intervention; 3) in‑ feasibility of surgical resection due to the lesion location or limited lung function reserve; 4) no possibility of complete resection of multiple le‑ sions; and 5) shrinking or stabilization of the le‑ sion after treatment with other methods, neces‑ sitating ablation or particle therapy to consoli‑ date the therapeutic effect.
Instruments and methods
Chest scanning was performed using a Siemens SOMATOM go.Up series 64‑slice spiral computed tomography (CT) ma‑ chine (Siemens, Erlangen, Germany) with the fol‑ lowing parameters: tube voltage of 120 kV, tube current of 285 mAs, slice thickness of 5 mm, and reconstructed slice thickness of 2 mm. The abla‑ tion equipment utilized was an ECO‑100A micro‑ wave ablation therapeutic device (Nanjing Yigao Microwave System Engineering Co., Ltd., Nanjing, China) operating at a frequency of 2450 MHz with an adjustable output power range of 0 to 50 W. The ECO 18G microwave ablation needle model ECO‑100 AL5 (Nanjing Yigao) had specifications of 1.6 mm × 150 mm. The patient’s position was determined based on the predefined puncture path, and local anesthesia was administered us‑ ing 1% lidocaine at the puncture site.
In the experimental group, preoperative as‑ sessments were undertaken to establish the pa‑ tient’s positioning, the strategy for nodule man‑ agement, puncture route, and other pertinent variables. After the routine chest CT scan, the skin puncture entry point was defined, the adjacent area was sanitized, and anesthesia was admin‑ istered to several sites using 10 milliliters of 1% lidocaine. Guided by CT imaging, both the abla‑ tion probe and the particle injector were inserted percutaneously into the precise location of the le‑ sion. After verification via another CT scan, mul‑ tiple nodules were targeted for ablation and par‑ ticle seeding. The ablation power was calibrat‑ ed at 40–60 W, with a total ablation time of 4 to 5 minutes, yielding a maximum ablation zone of 3.5 cm by 4 cm. Upon completion of ablation and withdrawal of the probe, CT imaging demonstrat‑ ed elevated density of lung tissue surrounding the lesion, creating a halo of 5 to 10 mm outside the lesion borders. The radiation oncologist for‑ mulated a treatment protocol with a target vol‑ ume dose spanning from 100 to 140 Gy. With CT imaging as a guide, once the implantation nee‑ dle precisely accessed the tumor site, ^125^I particles (Saili, Tianjin, China) with a dose of 0.7 mCi were administered at intervals of 1 to 1.5 cm. A follow‑up chest CT scan was performed to test for any potential complications, such as pneumothorax or hemorrhage.
The preoperative preparation of the control group was identical to that of the experimen‑ tal group. Under CT guidance, the ablation nee‑ dle was percutaneously inserted into the loca‑ tion of the lesion. The ablation parameters utilized were consistent with those employed in the experimental group. Upon cessation of ab‑ lation and subsequent removal of the needle, CT scanning revealed increased density of lung tis‑ sue surrounding the lesion, forming a halo that surpassed the lesion boundaries by 5–10 mm. The ablation range was then evaluated. Particle implantation was conducted either 1 week af‑ ter MWA or once the complications had fully re‑ solved. The preoperative procedure for particle implantation was the same as described above, and the particle specifications and administration methods were analogous to those used in the ex‑ perimental group. After completion, the particle needle was removed. A subsequent chest CT scan was performed to check for any complications, such as pneumothorax or bleeding.
Efficacy and complications
Promptly after the pro‑ cedure, a chest CT scan was performed to evaluate the ablation zone, which was deemed adequate if a ground‑glass opacity with a thickness ranging from 0.5 to 1 cm was visible on the periphery of the nodule.5 Furthermore, a postoperative assess‑ ment of the treatment volume covered by particle radiotherapy was performed to check whether it aligned with the anticipated outcomes. Technical success rates were calculated accordingly.
Complications including pneumothorax, pleural effusion, and hemoptysis, were evaluat‑ ed within 24 hours after surgery in accordance with the guidelines established by the Interna‑ tional Collaborative Group on Tumor Ablation.6 The postoperative complications were assessed using the following criteria: pleural effusion was categorized as minor (<500 ml), moderate (500–1000 ml), or significant (>1000 ml); pneu‑ mothorax was categorized as mild (<20% lung compression), moderate (20%–50% lung com‑ pression), or severe (>50% lung compression); and hemoptysis was categorized as slight (<10 ml), moderate (10–100 ml), or substantial (>100 ml).
Follow‑up
Postoperative follow‑up was con‑ ducted for a period of 6 months to monitor for complications such as needle tract metastasis, pulmonary embolism, bronchopleural fistula, or mortality. The follow‑up included plain and contrast‑enhanced chest CT scans at 1, 3, and 6 months postoperatively. The diameter of the nod‑ ular enhancement area in the arterial phase was measured during these scans. All sample size data were obtained from contrast‑enhanced CT images performed before and after treatment, and the maximum diameter line of the lesion in the same plane was selected for comparison. Data collected 1 month after the surgery were used as baseline for evaluating efficacy at 3 and 6 months postoperatively. The efficacy was assessed using several criteria. Complete response (CR) was defined as a reduction in the ablation target area or the formation of a scar, accompa‑ nied by a ≥50% decrease in the diameter of the im‑ planted particle nodule and no enhancement of the lesion. Partial response (PR) was defined as the formation of honeycomb or cavity structures within the lesion after ablation and particle implantation, with a ≥30% decrease in the diame‑ ter of the enhancement area in the arterial phase. Stable disease (SD) was defined as a decrease in le‑ sion density with either a <30% decrease or <20% increase in the diameter of the enhancement area in the arterial phase. Progressive disease (PD) was defined as a ≥20% increase in the diameter of the enhancement area in the arterial phase or the emergence of new lesions. The overall re‑ sponse rate was calculated as CR + PR / total num‑ ber of cases × 100%, and the local control rate was determined as CR + PR + SD / total number of cas‑ es × 100%.7 Additionally, the total duration of hos‑ pitalization, from the date of surgery to the date of discharge, was calculated.
Statistical analysis
Statistical analysis was con‑ ducted using SPSS software, version 26.0 (SPSS Inc., Chicago, Illinois, United States). Quantita‑ tive data that followed a normal distribution were presented as mean (SD), and intergroup com‑ parisons were performed using the independent sample t tests. Comparisons of the patients’ sex, smoking history, complications, and treatment outcomes between the groups were conducted using the χ2 test. A P value of less than 0.05 was considered significant.
Ethics
This study received approval from the lo‑ cal institutional review board (KYSQ014‑2024), and all patients provided written informed con‑ sent to participate in it. The study complies with the ethical guidelines outlined in the Declaration of Helsinki, originally established in 1975 and revised in 2000.
RESULTS
Basic information No significant differences were observed between the 2 groups in terms of sex, age, body mass index, smoking his‑ tory, pathological type, and Tumor, Node, Metastasis classification. Detailed information is presented in TABLE 1.
Complications and hospital stay
All the patients underwent the procedure successfully, achiev‑ ing a technical success rate of 100% (58/58). In the experimental group, 3 patients experienced hemoptysis (3/28; 10.71%), 4 had small pneu‑ mothorax (4/28; 14.28%), and 2 had pleural ef‑ fusion (2/28; 7.14%). In the control group, 4 pa‑ tients experienced hemoptysis (4/30; 13.33%), 5 had small pneumothorax (5/30; 16.67%), and 3 had pleural effusion (3/30; 10%). No differenc‑ es were observed between the 2 groups in the in‑ cidence of pneumothorax, pleural effusion, or he‑ moptysis. However, there was a notable discrep‑ ancy in the duration of hospital stay which was 4.54 (1.29) days for the experimental group and 7.97 (0.93) days for the control group (P = 0.03). Detailed information is shown in TABLE 2.
Efficacy The technical success rate was 100% in both groups. At the 3‑month postoperative follow‑up, the total effective rate was 70% (21/30) and the local control rate was 100% (30/30) in the control group, compared with 75% (21/28) and 100% (28/28), respectively, in the experi‑ mental group. No differences were observed be‑ tween the groups in terms of the total effective rate and local control rate (Z = –0.422; P = 0.67). Similarly, at the 6‑month postoperative follow‑up, the total effective rate in the control group was 80% (24/30) and the local control rate was 100% (30/30), versus 82.1% (23/28) and 100% (28/28), respectively, in the experimental group. Again, no differences were noted between the groups in the total effective rate and local control rate (Z = –0.206; P = 0.84). Detailed data are presented in FIGURE 3. Imaging data of a patient who un‑ derwent simultaneous MWA and particle implan‑ tation are presented in 1^,^2^,^3^,^4
DISCUSSION
With the growing prevalence of low‑dose computed tomography (LDCT) and ad‑ vancements in artificial intelligence, the detection rate of lung nodules has surged, demonstrating a tendency toward multiple occurrences among younger individuals.8 An LDCT scanning scheme is used to reduce patient radiation exposure.9 Tho‑ racoscopic wedge resection or segmentectomy can accomplish complete removal of the lesion while enabling pathological biopsy, achieving a diagnos‑ tic accuracy rate of 100%. Consequently, numer‑ ous scholars advocate for the benefits of resec‑ tion surgery.10 However, for nodules located near the lung hilum or in other challenging locations, surgical resection may cause significant trauma, resulting in substantial loss of lung tissue and compromised lung function. Postoperative com‑ plications can also harm patients, as early surgi‑ cal intervention does not substantially improve the overall patient survival rate.11^,^12
Thermal ablation has continuously pro‑ gressed in tumor therapy, playing a pivotal role in the treatment of patients with advanced lung cancer or metastatic lung tumors with no surgi‑ cal indications.13 MWA typically utilizes 2 fre‑ quencies: 915 MHz and 2450 MHz. Under the in‑ fluence of microwave electromagnetic fields, po‑ lar molecules, such as water and protein mole‑ cules in tumor tissue, undergo extremely rapid vibrations, causing mutual collisions and fric‑ tion. This leads to a rapid increase in tempera‑ ture up to 60–150 °C, resulting in cellular coagu‑ lation necrosis. The microwave energy is focused within a specific area by an antenna, enabling ef‑ fective radiation to the target area. Notably, mi‑ crowave thermal radiation exhibits a higher con‑ vection coefficient and a lesser heat deposition effect in the lungs.14 Literature reports suggest that the complete ablation rate of tumors located in the outer one‑third of the lung is remarkably higher than that of tumors in the middle and inner one‑third.15
This is attributed to the proxim‑ ity of the middle and inner parts of the lungs to the heart, large blood vessels, and main airways. In consideration of these factors, it is worth ex‑ ploring whether the use of combined methods can enhance efficacy of the procedure. Studies have found that ^125^I particle irradiation activates the p38MAPK/MDM2/p53 signaling pathway, promoting apoptosis in non‑small cell lung cancer (NSCLC) cells.16 Relevant guidelines indicate that when the tumor diameter exceeds 5 cm or its location may impact the ablation effect, com‑ bined treatment with alternative methods can be considered.17 ^125^I seed implantation, a form of in‑ ternal radiation therapy, has proved effective in the treatment of prostate cancer,18 brain tumors,19 and recurrent cervical cancer.20 As a form of local brachytherapy, after being introduced and contin‑ uously refined by Wang et al,21 Jiang et al,22 and Qu et al,23 combined with various auxiliary guid‑ ance techniques, this treatment approach is now extensively employed in the clinical management of solid malignant tumors in various locations. Yu et al24 reported that ^125^I seed implantation ex‑ hibited superior effectiveness in treating stage III recurrent NSCLC patients, with a prolonged me‑ dian survival time and no severe complications. In our research, the average length of hospital stay in the experimental group was shorter than that in the control group, although no significant dif‑ ference in efficacy and treatment efficiency was observed between the 2 groups. This indicates that the use of ^125^I seed implantation for close‑range radiotherapy in conjunction with MWA for pulmonary nodules may shorten patients’ hospi‑ talization and potentially reduce their economic burden to a certain extent.
A–D – imaging data of a 64-year-old woman who underwent surgery on the lower lobe of her right lung. The arrow (B) indicates the shadow of the surgical stapler after the operation. The local soft tissue mass was confirmed by biopsy to be a local tumor recurrence.
A–D – chest computed tomography performed during microwave ablation (MWA) combined with particle implantation showing insertion of the the MWA needle (B, arrow) and the particle implantation needle (C, arrow) into the target location, according to the preoperative plan
A–D – chest computed tomography performed during microwave ablation combined with particle implantation to assess the microwave ablation range, radioactive particle placement, and occurrence of complications
A–D – chest computed tomography performed 10 minutes after microwave ablation combined with particle implantation, showing a satisfactory ablation area, uniform particle implantation distribution, and minimal bleeding from the needle tract
Primary complications associated with MWA and particle implantation include pneumothorax, hemorrhage, and pleural effusion. These compli‑ cations are influenced by factors such as the le‑ sion’s location, size, depth, and elasticity, as well as the compliance of the lung tissue.25 Here, lon‑ ger localization time was identified as a risk factor significantly associated with the odds of pneumothorax and lung hemorrhage, whereas positional change was specifically associated with the risk of pneumothorax.26 When MWA targets pulmonary nodules situated in the proximity to the pleura, pericardium, and lung hilum, it may lead to se‑ vere complications such as pleural fistulas, nerve injuries, and substantial bleeding, potentially im‑ pairing patients’ quality of life and even posing life‑threatening risks. Consequently, this study aimed to address high‑risk pulmonary nodules by integrating MWA with particle implantation, in order to achieve complete remission.
The results demonstrated that the technical success rate for CT‑guided MWA, combined with either simultaneous or delayed particle implan‑ tation, in treating pulmonary nodules was 100%. The treatment efficacy for nodules, assessed at 3‑and 6‑month follow‑up, exceeded 70%, fully aligning with clinical expectations. No differenc‑ es were observed between the 2 groups in terms of the incidence of pleural effusion, hemoptysis, and pneumothorax, as well as the overall effective rate of nodule control. These findings suggest that both methods are comparably effective and safe. However, patients undergoing MWA combined with simultaneous particle implantation had a shorter total hospital stay compared with those treated with MWA combined with delayed particle implantation.
CONCLUSIONS
This study shows that MWA in combination with particle implantation offers high safety and a reduced incidence of complications. By ensuring surgical efficacy without augmenting complication rates, this approach can shorten patients’ hospitalization, alleviate their economic burden, and enhance their over‑ all medical experience. It can be successfully used to treat lung nodules with minimal trauma, pre‑ cise short‑term effectiveness, and limited harm. However, the study is limited to cases of multiple lung nodules located in the same lung lobe, insuf‑ ficient samples, and a relatively short follow‑up period. Consequently, long‑term clinical efficacy assessment requires additional follow‑up, which may inherently introduce occasional inaccuracies.
Further research grounded in extensive clinical big data is required to establish whether this com‑ bined therapy can supersede surgery as the pri‑ mary
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global cancer statistics 2020: GLOBO- CAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer Clin 71 Sung H. Ferlay J. Siegel R.L. 2021209249209-24910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Image-guided percutaneous microwave ablation of early-stage non-small cell lung cancer Asia Pac J Clin Oncol 16 Ni Y. Xu H. Ye X. 2020320325320-3253296919210.1111/ajco.13419 · doi ↗ · pubmed ↗
- 3Alternatives to surgery for early-stage non-small cell lung cancer: thermal ablation Clin Chest Med 41 Quirk M.T. Lee S. Murali N. 2020197210197-2103240235610.1016/j.ccm.2020.02.002 · doi ↗ · pubmed ↗
- 4Palliative endobronchial brachythera- py for non-small cell lung cancer Cochrane Database Syst Rev 12 Reveiz L. Rueda Cardona A.F. 201200428410.1002/14651858.CD 004284.pub 3PMC 1184851123235606 · doi ↗ · pubmed ↗
- 5Loss of cellular viability in ar- eas of ground-glass opacity on computed tomography images immediate- ly after pulmonary radiofrequency ablation in rabbits Jpn J Radiol 30 Kuroki M. Nakada H. Yamashita A. 2012323330323-3302230229510.1007/s 11604-012-0054-y · doi ↗ · pubmed ↗
- 6CTCAE v 3.0: development of a comprehensive grading system for the adverse effects of cancer treatment Semin Radiat Oncol 13 Trotti A. Colevas A.D. Setser A. 2003176181176-1811290300710.1016/S 1053-4296(03)00031-6 · doi ↗ · pubmed ↗
- 7Significance of different response evaluation criteria in predicting progression-free survival of lung cancer with certain imaging characteristics Thorac Cancer 7 Yang D. Woodard G. Zhou C. 2016535542535-5422776677710.1111/1759-7714.12363 PMC 5130210 · doi ↗ · pubmed ↗
- 8Safely and effectively carry out percutaneous biopsy and ablation of small pulmonary nodules Chin J Interv Imaging Ther 18 Xiao Y.Y. Wei Y.T. 2021232-3