Impact of Maternal Hyperglycemic and Hypertensive Disorders on Perinatal Outcomes Across the COVID-19 Pandemic
Lixia Zhang, Yun Shen, Ronald Horswell, Jessica Lin, San Chu, S. Amanda Dumas, Gang Hu

TL;DR
This study found that maternal hyperglycemic and hypertensive disorders during pregnancy are linked to higher risks of adverse outcomes for mothers and newborns, even during the COVID-19 pandemic.
Contribution
The study reveals consistent associations between maternal metabolic disorders and adverse perinatal outcomes across different pandemic phases.
Findings
Maternal diabetes and hypertension were linked to higher risks of preterm birth and neonatal complications during the pandemic.
The associations between maternal disorders and adverse outcomes remained consistent before and during the pandemic.
Controlling blood sugar and blood pressure is critical to reducing perinatal risks regardless of pandemic conditions.
Abstract
This study aimed to evaluate the joint associations of maternal hyperglycemic and hypertensive disorders with adverse pregnancy outcomes across the coronavirus disease 2019 (COVID-19) pandemic. This retrospective study included 110,447 Louisiana Medicaid pregnant women with first-time delivery from January 1, 2016, to December 31, 2021. Associations between hyperglycemic as well as hypertensive disorders and adverse pregnancy outcomes in pregnancy during prepandemic, early pandemic, and late pandemic were assessed by binary logistic regression. The odds ratios of above adverse pregnancy outcomes were significantly higher during the early and late COVID-19 pandemic than those before the pandemic. Maternal gestational diabetes mellitus and diabetes before pregnancy were associated with higher risks of preterm birth, primary cesarean section, large for gestational age (LGA), macrosomia,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
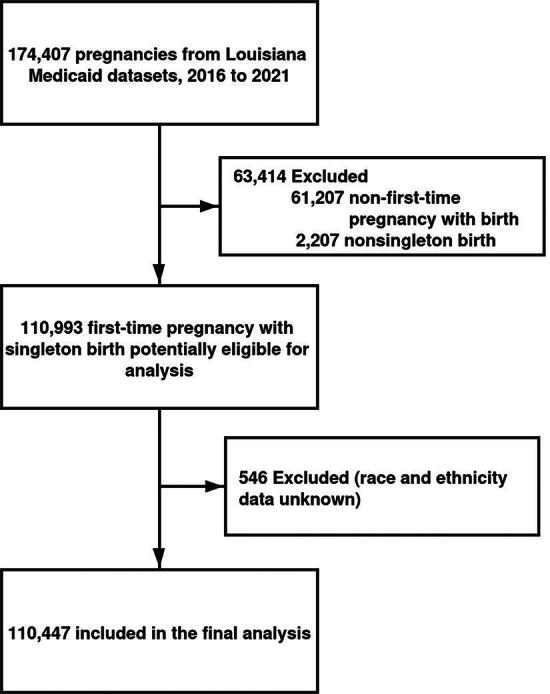 FIG. 1
FIG. 1| Variables | Total | COVID-19 pandemic | |||
|---|---|---|---|---|---|
|
|
|
| |||
| No. of participants | 110,447 | 82,266 | 16,305 | 11,876 | |
| Age, mean (SD), years | 26.2 (6.04) | 26.3 (5.97) | 25.9 (6.25) | 25.7 (6.19) | <0.001 |
| Race and ethnicity, | <0.001 | ||||
| White | 48,385 (43.8) | 37,074 (45.1) | 6,481 (39.7) | 4,830 (40.7) | |
| Black | 44,255 (40.1) | 32,858 (39.9) | 6,705 (41.1) | 4,692 (39.5) | |
| Other | 17,807 (16.1) | 12,334 (15.0) | 3,119 (19.1) | 2,354 (19.8) | |
| Diabetes during pregnancy, | <0.001 | ||||
| Normal glucose | 100,180 (90.7) | 74,934 (91.1) | 14,537 (89.2) | 10,709 (90.2) | |
| Gestational diabetes mellitus | 7,357 (6.66) | 5,191 (6.31) | 1,338 (8.21) | 828 (6.97) | |
| Diabetes before pregnancy | 2,910 (2.63) | 2,141 (2.60) | 430 (2.64) | 339 (2.85) | |
| Hypertensive disorders of pregnancy, | <0.001 | ||||
| No | 84,808 (76.8) | 65,237 (79.3) | 12,283 (75.3) | 8,798 (74.1) | |
| Yes | 25,639 (23.2) | 17,029 (20.7) | 4,022 (24.7) | 3,078 (25.9) | |
| Preterm birth, | 0.03 | ||||
| No | 102,104 (92.4) | 75,959 (92.3) | 15,150 (92.9) | 10,995 (92.6) | |
| Yes | 8,343 (7.55) | 6,307 (7.67) | 1,155 (7.08) | 881 (7.42) | |
| Primary cesarean section, | <0.001 | ||||
| No | 100,049 (90.6) | 74,777 (90.9) | 14,668 (90.0) | 10,604 (89.3) | |
| Yes | 10,398 (9.41) | 7,489 (9.10) | 1,637 (10.0) | 1,272 (10.7) | |
| Low birth weight, | <0.001 | ||||
| No | 103,144 (93.4) | 76,985 (93.6) | 15,121 (92.7) | 11,038 (92.9) | |
| Yes | 7,303 (6.61) | 5,281 (6.42) | 1,184 (7.26) | 838 (7.06) | |
| Small for gestational age, | <0.001 | ||||
| No | 105,061 (95.1) | 78,893 (95.9) | 15,112 (92.7) | 11,056 (93.1) | |
| Yes | 5,386 (4.88) | 3,373 (4.10) | 1,193 (7.32) | 820 (6.90) | |
| Large for gestational age, | <0.001 | ||||
| No | 107,008 (96.9) | 79,837 (97.0) | 15,686 (96.2) | 11,485 (96.7) | |
| Yes | 3,439 (3.11) | 2,429 (2.95) | 619 (3.80) | 391 (3.29) | |
| Macrosomia, | <0.001 | ||||
| No | 106,853 (96.7) | 79,719 (96.9) | 15,665 (96.1) | 11,469 (96.6) | |
| Yes | 3,594 (3.25) | 2,547 (3.10) | 640 (3.93) | 407 (3.43) | |
| Neonatal hypoglycemia, | <0.001 | ||||
| No | 102,880 (93.1) | 77,101 (93.7) | 14,905 (91.4) | 10,874 (91.6) | |
| Yes | 7,567 (6.85) | 5,165 (6.28) | 1,400 (8.59) | 1,002 (8.44) | |
| Neonatal jaundice, | <0.001 | ||||
| No | 67,032 (60.7) | 50,212 (61.0) | 9,562 (58.6) | 7,258 (61.1) | |
| Yes | 43,415 (39.3) | 32,054 (39.0) | 6,743 (41.4) | 4,618 (38.9) | |
| Neonatal respiratory distress syndrome, | <0.001 | ||||
| No | 98,473 (89.2) | 73,732 (89.6) | 14,326 (87.9) | 10,415 (87.7) | |
| Yes | 11,974 (10.8) | 8,534 (10.4) | 1,979 (12.1) | 1,461 (12.3) | |
| Outcomes | Total | Odds ratios (95% confidence intervals) | ||||
|---|---|---|---|---|---|---|
| Preterm birth ( | 1.00 | 1.18 (1.08–1.28) | 1.68 (1.50–1.88) | <0.001 | 0.07 | |
| Prepandemic | 1.00 | 1.00 | 1.25 (1.13–1.38) | 1.72 (1.51–1.96) | <0.001 | |
| Early pandemic | 0.92 (0.86–0.98) | 0.92 (0.86–0.99) | 1.08 (0.88–1.32) | 1.41 (1.04–1.93) | 0.005 | |
| Late pandemic | 0.97 (0.90–1.04) | 1.00 (0.92–1.08) | 0.80 (0.60–1.07) | 1.58 (1.13–2.22) | 0.27 | |
| | 0.07 | 0.35 | 0.003 | 0.40 | ||
| Primary cesarean section ( | 1.00 | 1.36 (1.26–1.46) | 2.26 (2.05–2.49) | <0.001 | 0.83 | |
| Prepandemic | 1.00 | 1.00 | 1.36 (1.25–1.49) | 2.24 (2.00–2.51) | <0.001 | |
| Early pandemic | 1.11 (1.05–1.17) | 1.10 (1.04–1.17) | 1.40 (1.19–1.65) | 2.69 (2.13–3.39) | <0.001 | |
| Late pandemic | 1.19 (1.12–1.27) | 1.19 (1.11–1.27) | 1.69 (1.38–2.05) | 2.56 (1.96–3.34) | <0.001 | |
| | <0.001 | <0.001 | 0.08 | 0.19 | ||
| Low birth weight ( | 1.00 | 1.06 (0.96–1.16) | 2.20 (1.97–2.45) | <0.001 | 0.30 | |
| Prepandemic | 1.00 | 1.00 | 1.10 (0.98–1.24) | 2.23 (1.97–2.53) | 0.007 | |
| Early pandemic | 1.13 (1.06–1.21) | 1.15 (1.07–1.23) | 1.04 (0.84–1.30) | 2.72 (2.10–3.52) | <0.001 | |
| Late pandemic | 1.11 (1.03–1.20) | 1.13 (1.04–1.23) | 1.14 (0.86–1.49) | 2.01 (1.46–2.78) | <0.001 | |
| | <0.001 | <0.001 | 0.97 | 0.99 | ||
| Small for gestational age ( | 1.00 | 0.84 (0.75–0.95) | 1.12 (0.96–1.32) | 0.66 | 0.33 | |
| Prepandemic | 1.00 | 1.00 | 0.84 (0.72–0.98) | 0.98 (0.79–1.21) | 0.13 | |
| Early pandemic | 1.82 (1.70–1.95) | 1.81 (1.69–1.95) | 1.39 (1.10–1.77) | 2.63 (1.93–3.57) | 0.56 | |
| Late pandemic | 1.72 (1.59–1.87) | 1.71 (1.58–1.86) | 1.40 (1.04–1.89) | 2.18 (1.50–3.17) | 0.64 | |
| | <0.001 | <0.001 | <0.001 | <0.001 | ||
| Large for gestational age ( | 1.00 | 1.42 (1.26–1.60) | 3.05 (2.65–3.51) | <0.001 | 0.50 | |
| Prepandemic | 1.00 | 1.00 | 1.51 (1.31–1.74) | 3.19 (2.71–3.76) | <0.001 | |
| Early pandemic | 1.30 (1.19–1.42) | 1.34 (1.21–1.48) | 1.60 (1.23–2.08) | 3.63 (2.60–5.06) | <0.001 | |
| Late pandemic | 1.12 (1.00–1.24) | 1.14 (1.01–1.28) | 1.43 (1.01–2.02) | 3.14 (2.11–4.67) | <0.001 | |
| | <0.001 | <0.001 | 0.89 | 0.85 | ||
| Macrosomia ( | 1.00 | 1.47 (1.30–1.65) | 3.09 (2.70–3.55) | <0.001 | 0.50 | |
| Prepandemic | 1.00 | 1.00 | 1.54 (1.34–1.76) | 3.25 (2.77–3.81) | <0.001 | |
| Early pandemic | 1.28 (1.18–1.40) | 1.32 (1.20–1.46) | 1.61 (1.24–2.08) | 3.47 (2.48–4.84) | <0.001 | |
| Late pandemic | 1.11 (1.00–1.23) | 1.12 (1.00–1.26) | 1.58 (1.14–2.18) | 3.25 (2.21–4.77) | <0.001 | |
| | <0.001 | <0.001 | 0.84 | 0.89 | ||
| Neonatal hypoglycemia ( | 1.00 | 13.1 (12.4–14.0) | 23.7 (21.9–25.7) | <0.001 | 0.004 | |
| Prepandemic | 1.00 | 1.00 | 12.3 (11.4–13.2) | 23.4 (21.3–25.8) | <0.001 | |
| Early pandemic | 1.39 (1.31–1.48) | 1.21 (1.10–1.32) | 20.0 (17.8–22.4) | 33.2 (27.3–40.3) | <0.001 | |
| Late pandemic | 1.37 (1.28–1.47) | 1.38 (1.25–1.52) | 17.9 (15.4–20.7) | 29.8 (24.0–37.0) | <0.001 | |
| | <0.001 | <0.001 | <0.001 | 0.002 | ||
| Neonatal jaundice ( | 1.00 | 1.22 (1.16–1.28) | 1.62 (1.51–1.75) | <0.001 | 0.86 | |
| Prepandemic | 1.00 | 1.00 | 1.24 (1.17–1.31) | 1.60 (1.47–1.74) | <0.001 | |
| Early pandemic | 1.11 (1.07–1.15) | 1.11 (1.07–1.15) | 1.30 (1.16–1.45) | 1.88 (1.55–2.27) | <0.001 | |
| Late pandemic | 0.99 (0.96–1.03) | 0.99 (0.95–1.04) | 1.17 (1.02–1.35) | 1.66 (1.34–2.06) | <0.001 | |
| | 0.04 | 0.51 | 0.81 | 0.40 | ||
| Neonatal respiratory distress syndrome ( | 1.00 | 1.33 (1.24–1.43) | 3.00 (2.75–3.27) | <0.001 | 0.46 | |
| Prepandemic | 1.00 | 1.00 | 1.32 (1.21–1.44) | 3.07 (2.77–3.39) | <0.001 | |
| Early pandemic | 1.20 (1.14–1.27) | 1.20 (1.14–1.27) | 1.50 (1.29–1.76) | 3.72 (3.02–4.59) | <0.001 | |
| Late pandemic | 1.23 (1.16–1.30) | 1.23 (1.15–1.31) | 1.73 (1.43–2.09) | 3.09 (2.41–3.95) | <0.001 | |
| | <0.001 | <0.001 | 0.006 | 0.55 | ||
| Outcomes | Odds ratios (95% confidence intervals) | |||||
|---|---|---|---|---|---|---|
| Preterm birth ( | 1.00 | 0.78 (0.71–0.87) | 1.49 (1.38–1.60) | 1.37 (1.27–1.48) | <0.001 | 0.22 |
| Prepandemic | 1.00 | 0.79 (0.70–0.89) | 1.55 (1.41–1.69) | 1.41 (1.29–1.54) | <0.001 | |
| Early pandemic | 0.92 (0.85–0.99) | 0.80 (0.63–1.01) | 1.24 (1.03–1.49) | 1.31 (1.09–1.57) | <0.001 | |
| Late pandemic | 1.01 (0.93–1.10) | 0.66 (0.49–0.88) | 1.39 (1.14–1.70) | 1.09 (0.86–1.36) | 0.12 | |
| | 0.50 | 0.34 | 0.09 | 0.03 | ||
| Primary cesarean section ( | 1.00 | 1.24 (1.15–1.34) | 1.56 (1.46–1.68) | 1.85 (1.73–1.97) | <0.001 | 0.70 |
| Prepandemic | 1.00 | 1.18 (1.07–1.30) | 1.58 (1.45–1.72) | 1.82 (1.69–1.96) | <0.001 | |
| Early pandemic | 1.08 (1.01–1.16) | 1.47 (1.24–1.75) | 1.57 (1.33–1.84) | 2.06 (1.77–2.39) | <0.001 | |
| Late pandemic | 1.15 (1.07–1.25) | 1.53 (1.26–1.85) | 1.77 (1.48–2.10) | 2.22 (1.88–2.62) | <0.001 | |
| | <0.001 | 0.004 | 0.40 | 0.01 | ||
| Low birth weight ( | 1.00 | 0.96 (0.85–1.08) | 4.89 (4.59–5.21) | 3.54 (3.31–3.79) | <0.001 | 0.77 |
| Prepandemic | 1.00 | 0.93 (0.81–1.07) | 4.94 (4.58–5.34) | 3.59 (3.32–3.88) | <0.001 | |
| Early pandemic | 1.10 (1.00–1.20) | 1.14 (0.89–1.46) | 4.93 (4.30–5.66) | 3.90 (3.37–4.53) | <0.001 | |
| Late pandemic | 1.06 (0.95–1.18) | 1.00 (0.74–1.35) | 5.29 (4.55–6.17) | 3.37 (2.82–4.02) | <0.001 | |
| | 0.07 | 0.41 | 0.49 | 0.81 | ||
| Small for gestational age ( | 1.00 | 1.63 (1.48–1.80) | 2.40 (2.21–2.60) | 1.68 (1.54–1.84) | <0.001 | 0.06 |
| Prepandemic | 1.00 | 1.56 (1.37–1.77) | 2.47 (2.23–2.74) | 1.64 (1.46–1.83) | <0.001 | |
| Early pandemic | 1.87 (1.72–2.03) | 2.67 (2.19–3.26) | 3.63 (3.08–4.29) | 2.74 (2.27–3.30) | <0.001 | |
| Late pandemic | 1.60 (1.44–1.77) | 2.94 (2.37–3.65) | 3.68 (3.05–4.45) | 3.32 (2.72–4.05) | <0.001 | |
| | <0.001 | <0.001 | <0.001 | <0.001 | ||
| Large for gestational age ( | 1.00 | 1.18 (1.03–1.35) | 1.07 (0.94–1.22) | 1.35 (1.20–1.52) | <0.001 | 0.14 |
| Prepandemic | 1.00 | 1.13 (0.96–1.33) | 1.03 (0.87–1.21) | 1.44 (1.26–1.66) | <0.001 | |
| Early pandemic | 1.32 (1.19–1.47) | 1.75 (1.35–2.27) | 1.20 (0.89–1.63) | 1.47 (1.11–1.94) | 0.49 | |
| Late pandemic | 1.10 (0.97–1.25) | 1.22 (0.86–1.73) | 1.56 (1.15–2.10) | 1.24 (0.88–1.76) | 0.12 | |
| | <0.001 | 0.14 | 0.01 | 0.50 | ||
| Macrosomia ( | 1.00 | 1.19 (1.05–1.36) | 1.05 (0.92–1.20) | 1.34 (1.19–1.50) | <0.001 | 0.12 |
| Prepandemic | 1.00 | 1.15 (0.99–1.35) | 1.00 (0.85–1.18) | 1.44 (1.26–1.65) | <0.001 | |
| Early pandemic | 1.31 (1.18–1.45) | 1.67 (1.28–2.16) | 1.17 (0.87–1.58) | 1.45 (1.10–1.91) | 0.52 | |
| Late pandemic | 1.09 (0.96–1.24) | 1.27 (0.91–1.77) | 1.55 (1.16–2.08) | 1.18 (0.84–1.67) | 0.16 | |
| | 0.001 | 0.17 | 0.007 | 0.36 | ||
| Neonatal hypoglycemia ( | 1.00 | 1.55 (1.41–1.69) | 2.63 (2.45–2.83) | 3.45 (3.24–3.68) | <0.001 | 0.29 |
| Prepandemic | 1.00 | 1.60 (1.43–1.79) | 2.62 (2.39–2.86) | 3.53 (3.27–3.81) | <0.001 | |
| Early pandemic | 1.42 (1.31–1.53) | 2.05 (1.69–2.48) | 3.21 (2.75–3.75) | 4.48 (3.89–5.15) | <0.001 | |
| Late pandemic | 1.33 (1.21–1.46) | 1.71 (1.35–2.16) | 3.79 (3.21–4.48) | 4.48 (3.82–5.26) | <0.001 | |
| | <0.001 | 0.18 | <0.001 | <0.001 | ||
| Neonatal jaundice ( | 1.00 | 1.19 (1.13–1.25) | 1.57 (1.50–1.65) | 1.45 (1.39–1.52) | <0.001 | 0.09 |
| Prepandemic | 1.00 | 1.20 (1.13–1.27) | 1.53 (1.45–1.62) | 1.40 (1.33–1.48) | <0.001 | |
| Early pandemic | 1.08 (1.04–1.12) | 1.27 (1.14–1.42) | 1.74 (1.57–1.94) | 1.72 (1.54–1.92) | <0.001 | |
| Late pandemic | 0.96 (0.92–1.01) | 1.08 (0.95–1.23) | 1.67 (1.48–1.88) | 1.52 (1.34–1.72) | <0.001 | |
| | 0.995 | 0.41 | 0.05 | 0.02 | ||
| Neonatal respiratory distress syndrome ( | 1.00 | 1.19 (1.10–1.29) | 2.74 (2.59–2.91) | 2.64 (2.50–2.80) | <0.001 | 0.52 |
| Prepandemic | 1.00 | 1.22 (1.11–1.34) | 2.72 (2.53–2.92) | 2.71 (2.53–2.90) | <0.001 | |
| Early pandemic | 1.20 (1.12–1.28) | 1.39 (1.17–1.65) | 3.07 (2.70–3.49) | 2.97 (2.60–3.38) | <0.001 | |
| Late pandemic | 1.20 (1.12–1.30) | 1.22 (0.99–1.50) | 3.45 (3.00–3.98) | 2.93 (2.51–3.41) | <0.001 | |
| | <0.001 | 0.60 | 0.001 | 0.22 | ||
| Outcomes | Odds ratios (95% confidence intervals) | |||||
|---|---|---|---|---|---|---|
|
|
|
|
| |||
| Preterm birth ( | 1.00 | 1.10 (0.98–1.22) | 1.16 (1.10–1.23) | 1.61 (1.47–1.77) | <0.001 | 0.01 |
| Primary cesarean section ( | 1.00 | 1.31 (1.19–1.44) | 1.50 (1.43–1.58) | 2.21 (2.05–2.39) | <0.001 | 0.90 |
| Low birth weight ( | 1.00 | 0.89 (0.77–1.03) | 3.05 (2.89–3.21) | 2.96 (2.71–3.22) | <0.001 | 0.17 |
| Small for gestational age ( | 1.00 | 0.85 (0.72–1.00) | 1.97 (1.86–2.10) | 1.35 (1.19–1.52) | <0.001 | 0.11 |
| Large for gestational age ( | 1.00 | 1.26 (1.08–1.47) | 1.03 (0.94–1.14) | 2.47 (2.20–2.78) | <0.001 | <0.001 |
| Macrosomia ( | 1.00 | 1.29 (1.11–1.49) | 1.02 (0.93–1.12) | 2.52 (2.25–2.82) | <0.001 | <0.001 |
| Neonatal hypoglycemia ( | 1.00 | 15.4 (14.3–16.6) | 2.33 (2.17–2.50) | 24.7 (23.1–26.5) | <0.001 | <0.001 |
| Neonatal jaundice ( | 1.00 | 1.16 (1.09–1.23) | 1.36 (1.32–1.41) | 1.68 (1.59–1.78) | <0.001 | 0.53 |
| Neonatal respiratory distress syndrome ( | 1.00 | 1.20 (1.09–1.33) | 2.08 (1.99–2.18) | 3.10 (2.89–3.32) | <0.001 | 0.18 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Impact on Reproduction · Gestational Diabetes Research and Management · Pregnancy and preeclampsia studies
Introduction
Hyperglycemic disorders during pregnancy and hypertensive disorders of pregnancy (HDP) are the most common pregnancy complications worldwide due to increasing maternal age and higher prevalence of obesity as well as unhealthy lifestyle habits among women.^1,2^ Hyperglycemic disorders during pregnancy can arise from pre-existing conditions such as type 1 diabetes and type 2 diabetes to gestational diabetes mellitus (GDM), which emerges during pregnancy. HDP encompasses chronic hypertension that exists before pregnancy, gestational hypertension that develops during pregnancy, pre-eclampsia, and eclampsia. These maternal issues are associated with both immediate and long-term adverse outcomes, including increased risks of cesarean section, premature birth, low birth weight (LBW), excessive birth weight (macrosomia), newborn low blood sugar, respiratory problems in newborns, and higher risks of hypertension, diabetes, metabolic syndrome, and cardiovascular disease in the future.^3–10^ This presents a significant health challenge for both mothers and their children.
The coronavirus disease 2019 (COVID-19) pandemic, caused by the novel severe acute respiratory syndrome coronavirus 2, has heightened concern regarding its impact on maternal and neonatal health. Several observational studies and systematic reviews have investigated the pandemic’s impact on hyperglycemic disorders during pregnancy and HDP as well as adverse maternal and neonatal outcomes.^11–14^ These adverse outcomes include elevated risks of severe maternal morbidity, preterm birth, stillbirth, LBW, and potential neurodevelopmental challenges in offspring. However, another systematic review suggested that COVID-19 infection did not significantly affect pregnancy outcomes.^15^ This indicates that the full impact of COVID-19 on pregnancy outcomes remains unclear. Notably, there have been no studies exploring how COVID-19 affects the relationship between maternal hyperglycemic and hypertensive disorders and adverse pregnancy outcomes. The objectives of the present study were to assess the joint associations of maternal hyperglycemic and hypertensive disorders during pregnancy with adverse pregnancy outcomes across the COVID-19 pandemic in a comprehensive observational study utilizing data from the Louisiana Medicaid database.
Methods
Study design, population, and data source
The present study conducted a retrospective analysis of electronic health records from the Louisiana Medicaid dataset. Medicaid administrative data, collected by the Centers for Medicaid and Medicare Services, are primarily derived from reimbursement claims, reflecting the payment for services provided. These claims data are clinically reliable and encompass a broad array of essential health care attributes, including admission and discharge dates, diagnostic and procedure codes, source of care, and demographic information (such as date of birth, age, race and ethnicity, and sex).
Our analysis focused on women who gave birth between January 1, 2016, and December 31, 2021. We excluded records of nonfirst-time pregnancies, nonsingleton births, and cases with unknown race or ethnicity, culminating in a final sample of 110,447 pregnant women for our analysis (Fig. 1). Pregnancies were identified using the Tenth Revisions of the International Classification of Disease (ICD-10) code. The study and analytic plan were approved by the Institutional Review Boards at the Pennington Biomedical Research Center and the Louisiana Department of Health. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline.
Participants flow chart.
Hyperglycemic and hypertensive disorders in pregnancy
Hyperglycemic and hypertensive disorders during pregnancy were identified using ICD-10 codes. GDM cases were identified by using the ICD-10 code O24.4, which represents “gestational diabetes mellitus.” Identification of diabetes that was present before pregnancy was done using the ICD-10 codes O24.0 and O24.1, which refer to pre-existing diabetes that occurred in pregnancy for types 1 and 2 diabetes, respectively. Participants during pregnancy were divided into three subgroups according to their glucose status: normal glucose, GDM, and diabetes before pregnancy. HDP included pre-existing chronic hypertension, gestational hypertension, pre-eclampsia, and eclampsia. Pre-existing chronic hypertension before pregnancy was identified by the ICD-10 code O10 that selected women who had elevated blood pressure predating the pregnancy and ICD-10 code O11 that selected women who had preeclampsia superimposed on chronic hypertension. Gestational hypertension was identified using the ICD-10 code O13 that specifically selected women who were diagnosed at or after 20 weeks’ gestation. Pre-eclampsia was identified by the ICD-10 code O14 that selected women who were diagnosed at or after 20 weeks’ gestation. Eclampsia was identified by the ICD-10 code O15. Participants in pregnancy were classified into four subgroups according to their blood pressure status: normal blood pressure, gestational hypertension, pre-eclampsia or eclampsia, and pre-existing hypertension.
Definition of COVID-19 pandemic periods
The definition of COVID-19 pandemic periods was as follows: pregnancies impacted by the pandemic were those with deliveries after March 13, 2020, which marked the date of the first COVID-19 case reported in Louisiana. As a result, we established three groups based on delivery dates corresponding to the calendar years: the prepandemic period (from January 1, 2016, to March 12, 2020), the early pandemic period (from March 13, 2020, to March 12, 2021), and the late pandemic period (from March 13, 2021, to December 31, 2021). In addition, participants were further categorized into subgroups based on the presence of hyperglycemic and hypertensive disorders during pregnancy across different stages of the COVID-19 pandemic, with the specific numbers in Supplementary Table S1.
Adverse pregnancy outcomes
Adverse pregnancy outcomes were identified using the ICD-10 codes. Maternal outcomes included primary cesarean section (ICD-10 codes O66.4, O75.82, and O82, except O34.21), which was defined as cesarean section performed to women with no previous history of cesarean delivery. Neonatal outcomes were preterm birth (birth at <37 gestational weeks, ICD-10 codes O60.1 and P07.3), LBW (birth weight <2,500 g, ICD-10 codes P07.0 and P07.1), macrosomia (birth weight ≥4,000 g, ICD-10 codes P08.0 and P08.1), small for gestational age (SGA, birth weight <10^th^ percentile for a given gestational age, ICD-10 codes P05.0 and P05.1), large for gestational age (LGA, birth weight >90^th^ percentile for a given gestational age, ICD-10 code P08.1), neonatal hypoglycemia (ICD-10 codes P70.0, P70.1, and P70.4), neonatal jaundice (ICD-10 code P59), and neonatal respiratory distress syndrome (NRDS, ICD-10 code P22).
Statistical analysis
One-way analysis of variance and Chi-square tests were used to identify any differences in the characteristics of the women in the study and the prevalence of adverse pregnancy outcomes according to the COVID-19 pandemic status. We applied binary logistic regression models to assess the single and joint effects of different levels of maternal hyperglycemic or hypertensive disorders during pregnancy and the COVID-19 pandemic on adverse maternal–perinatal outcomes. All analyses were adjusted for maternal age, race, and ethnicity. We reported adjusted odds ratios (ORs) along with 95% confidence intervals (CIs) to delineate the relationship between predictor and outcome variables. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using R software, version 4.3.2.
Results
Effect of the COVID-19 pandemic on adverse pregnancy outcomes
The final analysis included 110,447 participants, among whom 82,266 delivered prepandemic, 16,305 were exposed to the early stages of the COVID-19 pandemic, and 11,876 to the late stages. Over these periods, there were minor shifts in maternal age, race, and ethnicity (all p < 0.001), as shown in Table 1. Deliveries during both the early and late stages of the pandemic compared with deliveries during prepandemic showed a significantly higher prevalence of hyperglycemic disorders during pregnancy, HDP, primary cesarean sections, LBW, SGA, LGA, macrosomia, neonatal hypoglycemia, neonatal jaundice, and NRDS (all p < 0.001), along with a slightly lower incidence of preterm birth (p = 0.03).
Compared with deliveries before the COVID-19 pandemic, the multivariable-adjusted (maternal age, race, and ethnicity) relative risks of adverse pregnancy outcomes among deliveries in the early pandemic and the late pandemic periods were significantly higher for primary cesarean section (OR: 1.11, 95% CI: 1.05–1.17; OR: 1.19, 95% CI: 1.12–1.27), LBW (OR: 1.13, 95% CI: 1.06–1.21; OR: 1.11, 95% CI: 1.03–1.20), SGA (OR: 1.82, 95% CI: 1.70–1.95; OR: 1.72, 95% CI: 1.59–1.87), LGA (OR: 1.30, 95% CI: 1.19–1.42; OR: 1.12, 95% CI: 1.00–1.24), macrosomia (OR: 1.28, 95% CI: 1.18–1.40; OR: 1.11, 95% CI: 1.00–1.23), neonatal hypoglycemia (OR: 1.39, 95% CI: 1.31–1.48; OR: 1.37, 95% CI: 1.28–1.47), neonatal jaundice (OR: 1.11, 95% CI: 1.07–1.15; OR: 0.99, 95% CI: 0.96–1.03), and NRDS (OR: 1.20, 95% CI: 1.14–1.27; OR: 1.23, 95% CI: 1.16–1.30), respectively (Table 2).
Associations between hyperglycemic disorders and adverse pregnancy outcomes across the COVID-19 pandemic
Women with GDM during pregnancy and women with diabetes before pregnancy were significantly associated with increased ORs of preterm birth (1.18 and 1.68, all p < 0.001), primary cesarean section (1.36 and 2.26, all p < 0.001), LGA (1.42 and 3.05, all p < 0.001), macrosomia (1.47 and 3.09, all p < 0.001), neonatal hypoglycemia (13.1 and 23.7, all p < 0.001), neonatal jaundice (1.22 and 1.62, all p < 0.001), and NRDS (1.33 and 3.07, all p < 0.001), respectively, compared with women with normal glucose tolerance during pregnancy (Table 2 and Supplementary Table S2).
When stratified analyses were utilized, the positive association of hyperglycemic disorders during pregnancy with the risks of primary cesarean section, LBW, LGA, macrosomia, neonatal hypoglycemia, neonatal jaundice, and NRDS before the COVID-19 pandemic was consistent with those during the early and late pandemic (Table 2).
Associations between HDP and adverse pregnancy outcomes across the COVID-19 pandemic
Compared with normal blood pressure during pregnancy, gestational hypertension was associated with higher odds of primary cesarean section, SGA, LGA, macrosomia, neonatal hypoglycemia, neonatal jaundice, and NRDS and was associated with lower odds of preterm birth (all p < 0.05). Moreover, pre-eclampsia or eclampsia and pre-existing hypertension significantly elevated the odds of preterm birth, primary cesarean section, LBW, SGA, neonatal hypoglycemia, neonatal jaundice, and NRDS (all p < 0.05), respectively (Table 3 and Supplementary Table S3). Pre-existing hypertension was associated with increased odds of LGA and macrosomia (all p < 0.05).
When stratified analyses were utilized, the positive associations of gestational hypertension, pre-eclampsia or eclampsia and pre-existing hypertension with the risks of primary cesarean section, LBW, SGA, neonatal hypoglycemia, neonatal jaundice, and NRDS remained consistent mostly before the COVID-19 pandemic and during the early and late pandemic (Table 3). The associations of pre-existing hypertension with the risks of LGA and macrosomia were consistent before the COVID-19 pandemic and during the early and late pandemic.
Joint associations of hyperglycemic disorders and HDP with adverse pregnancy outcomes
When we assessed the joint associations of hyperglycemic disorders during pregnancy and HDP with adverse pregnancy outcomes, women were divided into four groups based on results from Tables 2 and 3: women with normal glucose and blood pressure during pregnancy, women with hyperglycemic disorders during pregnancy only (GDM during pregnancy or diabetes before pregnancy), HDP only (gestational hypertension, pre-eclampsia, eclampsia, or pre-existing chronic hypertension), and both hyperglycemic disorders during pregnancy and HDP (Table 4 and Supplementary Table S4). In comparison with normal glucose and blood pressure during pregnancy, hyperglycemic disorders during pregnancy were only associated with the higher risks of primary cesarean section (OR: 1.31, 95% CI: 1.19–1.44), LGA (OR: 1.26, 95% CI: 1.08–1.47), macrosomia (OR: 1.29, 95% CI: 1.11–1.49), neonatal hypoglycemia (OR: 15.4, 95% CI: 14.3–16.6), neonatal jaundice (OR: 1.16, 95% CI: 1.09–1.23), and NRDS (OR: 1.20, 95% CI: 1.09–1.33); HDP only was associated with the higher risks of preterm birth (OR: 1.16, 95% CI: 1.10–1.23), primary cesarean section (OR 1.50, 95% CI 1.43–1.58), LBW (OR: 3.05, 95% CI: 2.89–3.21), SGA (OR: 1.97, 95% CI: 1.86–2.10), neonatal hypoglycemia (OR: 2.33, 95% CI: 2.17–2.50), neonatal jaundice (OR: 1.36, 95% CI: 1.32–1.41), and NRDS (OR: 2.08, 95% CI: 1.99–2.18); the presence of both hyperglycemic disorders during pregnancy and HDP was associated with the highest risks of above all adverse pregnancy outcomes (all p for trend <0.001).
Discussion
In this Louisiana surveillance study, delivery during the early and late COVID-19 pandemic was associated with significantly higher risks of most adverse pregnancy outcomes. Both hyperglycemic disorders during pregnancy and HDP were associated with greater risks of most adverse pregnancy outcomes, and most of these associations were consistent before the COVID-19 pandemic and during the early and late pandemic.
There is accumulating evidence that COVID-19 infection during pregnancy is linked to adverse maternal–perinatal outcomes. A multinational cohort study across 18 countries revealed that pregnancies affected by COVID-19 faced increased risks of preeclampsia and preterm birth compared with those without infection.^16^ A systematic review and meta-analysis showed increased risks of maternal death, cesarean section, preterm birth, stillbirth, and admission to the neonatal intensive care unit among COVID-19-infected women.^17^ In addition to the direct impact of COVID-19 infection on pregnancy outcomes, the effect of the COVID-19 pandemic on pregnancy outcomes even among those without infection was also reported. A global systematic review observed the increased rate of ruptured ectopic pregnancies, stillbirths, and maternal deaths during the pandemic than before the pandemic.^18^ On the contrary, several studies showed an overall decline in the rate of preterm birth during the pandemic period,^19–21^ which was consistent with our findings. That might be due to differences in enforcement of lockdown orders during the pandemic, population heterogeneity, access to health care, and societal stressors.^22^ These findings were intriguing and might potentially provide the clues to solving the long-standing challenges in preventing preterm birth.
Our findings are in agreement with other studies on the association between hyperglycemic disorders during pregnancy and adverse maternal–perinatal outcomes.^23^ Since the onset of the COVID-19 pandemic, there is a growing interest in the association between GDM and COVID-19. Studies have shown that COVID-19 infection might increase the severity of GDM or promote the de novo onset of GDM by causing acute β-cell dysfunction, which led to increased prevalence of GDM and even adverse maternal–perinatal outcomes.^24–26^ However, comprehensive data on the combined effect of these conditions on pregnancy outcomes remain scarce. In the present study, we observed that only the association between hyperglycemic disorders and preterm birth varied across COVID-19 pandemic periods; however, GDM was not significantly increasing the risk of preterm birth during the late pandemic, contrary to overall population trends. This discrepancy may be explained by factors such as higher gestational weight gain during the pandemic, treatment differences (metformin or insulin), and other pregnancy complications.^27,28^ Further research is needed to confirm our findings and uncover the mechanisms underlying these differential associations.
The present study also indicated that HDP was associated with an increased risk of adverse pregnancy outcomes. Interestingly, we observed a paradoxical negative statistical association between gestational hypertension and preterm birth in this study, contrasting with another study that found no significant association between gestational hypertension and preterm birth.^29^ In addition, we noted that an increased risk of preterm birth, LGA, and macrosomia associated with HDP during the early and late COVID-19 pandemic was lower than the risk observed in the prepandemic period. These variations may be attributed to a pre-eclampsia-like syndrome induced by COVID-19, which can cause endothelial damage and alterations in angiotensin-converting enzyme 2-related pathways, similar to the changes seen in preeclampsia.^30,31^ Furthermore, other pertinent factors not considered in the present study, such as history of preterm delivery, parity, maternal body mass index, and additional pregnancy complications, should also be taken into account.^32^ These findings underscore the importance of using representative and diverse samples with comprehensive data and highlight the necessity for further research in this area.
Strengths and Limitations
This study’s strengths include its large and diverse samples from a southern state, providing a significant breadth of data. Moreover, this study highlights findings from an underserved population in the United States, offering valuable insights for public health and policymakers.
Several limitations should be considered. First, adverse pregnancy outcomes using Medicaid claims data were limited by its nature as a claims database rather than a research database. A study examined preeclampsia in the U.S. Medicaid Analytical Extraction and found that the positive predictive value of preeclampsia was 67% when cross-checked with hospital records.^33^ Moreover, other studies have demonstrated high validity of Medicaid data in research.^34,35^ In the present analysis, we have no data to verify the diagnosis and rely on the accuracy of the claims. Second, due to its observational design and reliance on administrative data, the present study cannot ascertain the mechanisms driving the observed differences in the associations of maternal hyperglycemic disorders during pregnancy and HDP with adverse pregnancy outcomes throughout the COVID-19 pandemic periods. Third, while the study samples were representative of a metropolitan area, the findings may not extend to other regions, limiting generalizability. Fourth, the analysis lacked data on several important factors such as parity, maternal body mass index, gestational weight gain, and other pregnancy-related conditions, which were crucial confounders that could influence outcomes. Lastly, the study’s scope was confined to the initial 2 years of the COVID-19 pandemic, leaving the long-term effects on these associations undetermined.
Conclusions
The risks of adverse maternal and neonatal outcomes significantly increased during the early and late stages of the COVID-19 pandemic. Both hyperglycemic disorders during pregnancy and HDP were associated with greater risks of most adverse pregnancy outcomes, and most of these associations were consistent before the COVID-19 pandemic and during the early and late pandemic.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Intyre HD, Catalano P, Zhang C, et al. Gestational diabetes mellitus. Nat Rev Dis Primers 2019;5(1):47; doi: 10.1038/s 41572-019-0098-831296866 · doi ↗ · pubmed ↗
- 2Wu P, Green M, Myers JE. Hypertensive disorders of pregnancy. BMJ 2023;381:e 071653; doi: 10.1136/bmj-2022-07165337391211 · doi ↗ · pubmed ↗
- 3Pan L, Leng J, Liu G, et al. Pregnancy outcomes of Chinese women with gestational diabetes mellitus defined by the IADPSG’s but not by the 1999 WHO’s criteria. Clin Endocrinol (Oxf) 2015;83(5):684–693; doi: 10.1111/cen.1280125903847 · doi ↗ · pubmed ↗
- 4Li W, Liu H, Qiao Y, et al. Metabolic syndrome of weight change from pre-pregnancy to 1–5 years post-partum among Chinese women with prior gestational diabetes. Diabet Med 2015;32(11):1492–1499; doi: 10.1111/dme.1279025962467 PMC 4615340 · doi ↗ · pubmed ↗
- 5Yuan X, Liu H, Wang L, et al. Gestational hypertension and chronic hypertension on the risk of diabetes among gestational diabetes women. J Diabetes Complications 2016;30(7):1269–1274; doi: 10.1016/j.jdiacomp.2016.04.02527185731 PMC 5512696 · doi ↗ · pubmed ↗
- 6Shen Y, Wang P, Wang L, et al. Gestational diabetes with diabetes and prediabetes risks: A large observational study. Eur J Endocrinol 2018;179(1):51–58; doi: 10.1530/eje-18-013029743168 PMC 6009844 · doi ↗ · pubmed ↗
- 7Li W, Wang L, Liu H, et al. Maternal gestational diabetes and childhood adiposity risk from 6 to 8 years of age. Int J Obes (Lond) 2024;48(3):414–422; doi: 10.1038/s 41366-023-01441-y 38123838 PMC 10965231 · doi ↗ · pubmed ↗
- 8Zhang S, Wang L, Leng J, et al. Hypertensive disorders of pregnancy in women with gestational diabetes mellitus on overweight status of their children. J Hum Hypertens 2017;31(11):731–736; doi: 10.1038/jhh.2017.1728300070 PMC 5600626 · doi ↗ · pubmed ↗