Accuracy of ultrasound estimation of fetal weight in twin pregnancy
Patrick Dicker, Ronan Conroy, Fionnuala McAuliffe, Michael Geary, Sean Daly, John J. Morrison, Stephen Carroll, Fergal D. Malone, Fionnuala M. Breathnach

TL;DR
This study compares different formulas for estimating fetal weight in twin pregnancies and finds that some formulas are more accurate than others.
Contribution
The study evaluates 63 fetal weight estimation formulas in twin pregnancies and identifies the most accurate ones.
Findings
The Hadlock formulas (1984, 1985) were the most accurate with a median percentage error of less than 1%.
The INTERGROWTH-21st formula slightly underestimated birth weight but still showed high sensitivity for detecting low birth weight.
Using fewer ultrasound parameters (AC and HC) in the INTERGROWTH-21st formula did not significantly reduce accuracy.
Abstract
To determine the accuracy of formulas for estimation of fetal weight in twin pregnancy. Inclusion criteria from the ESPRiT twin cohort were twin pregnancies that resulted in live‐born twins without congenital anomalies or twin‐twin transfusion syndrome, ultrasound examination within 3 days of delivery, birth weight (BW) > 500 g and gestational age > 24 weeks. A total of 63 formulas using various combinations of abdominal circumference (AC), femur length (FL), biparietal diameter (BPD) and head circumference (HC) for the estimation of fetal weight (EFW), were compared to BW for accuracy in 226 twin pregnancies/452 fetuses. Using median percentage error (MPE), the most accurate formulas were the Hadlock formulas (1984, 1985 with MPE < 1%) incorporating AC, HC, and FL. The INTERGROWTH‐21st formula, which incorporates AC and HC, marginally underestimated BW (MPE −3.7%). The Hadlock…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
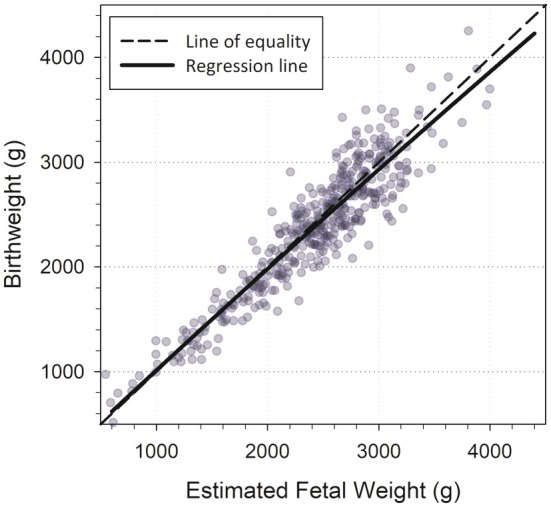 FIGURE 1
FIGURE 1| Label | Biometry used | Formula |
|---|---|---|
| 1984 publication | ||
| A1 | AC | Loge BW = 2.695 + 0.253 × AC − 0.00275 × AC2 |
| A2 | AC, BPD | Log10 BW = 1.1134 + 0.05845 × AC − 0.000604 × AC2 − 0.007365 × BPD2 + 0.000595 × BPD × AC + 0.1694 × BPD |
| A3 | AC, HC | Log10 BW = 1.182 + 0.0273 × HC + 0.07057 × AC − 0.00063 × AC2 − 0.0002184 × HC × AC |
| A4 | AC, FL | Log10 BW = 1.3598 + 0.051 × AC + 0.1844 × FL − 0.0037 × AC × FL |
| A5 | AC, BPD, FL | Log10 BW = 1.4787 − 0.003343 × AC × FL + 0.001837 × BPD2 + 0.0458 × AC + 0.158 × FL |
| A6 | AC, HC, FL | Log10 BW = 1.5662 − 0.0108 × HC + 0.0468 × AC + 0.171 × FL + 0.00034 × HC2 − 0.003685 × AC × FL |
| A7 | AC, HC, BPD, FL | Log10 BW = 1.5115 + 0.0436 × AC + 0.1517 × FL − 0.00321 × AC × FL + 0.0006923 × BPD × HC |
| 1985 publication | ||
| B1 | AC, FL | Log10 BW = 1.304 + 0.05281 × AC + 0.1938 × FL − 0.004 × AC × FL |
| B2 | AC, BPD, FL | Log10 BW = 1.335 + 0.0316 × BPD + 0.0457 × AC + 0.1623 × FL − 0.0034 × AC × FL |
| B3 | AC, HC, FL | Log10 BW = 1.326 − 0.00326 × AC × FL + 0.0107 × HC + 0.0438 × AC + 0.158 × FL |
| B4 | AC, HC, BPD, FL | Log10 BW = 1.3596 + 0.0064 × HC + 0.0424 × AC + 0.174 × FL + 0.00061 × BPD × AC − 0.00386 × AC × FL |
| Characteristic | Summary |
|---|---|
|
|
|
| Maternal age (years) | 33 [27, 39] |
| BMI ≥30 kg/m2 | 34 (15%) |
| Nulliparity | 113 (51%) |
| Chorionicity | |
| Monochorionic | 52 (23%) |
| Dichorionionic | 174 (77%) |
| GA at delivery (week) | 36.3 [32.0, 38.0] |
| Preterm delivery (<34 weeks) | 42 (19%) |
| BW discordance ≥18% | 73 (32%) |
| GA at last examination (week) | 36.1 [31.7, 37.7] |
|
|
|
| Birth weight (grams) | 2440 [1490, 3080] |
| Low BW (<5th centile) | 48 (11%) |
| Sex | |
| Female | 234 (52%) |
| Male | 216 (48%) |
| Fetal presentation at last examination | |
| Breech | 105 (28%) |
| Transverse | 57 (15%) |
| Cephalic | 212 (57%) |
| Formula | Biometry used | MPE | |PE| ≤ 10% | PE > 10% (a) | PE < −10% (b) | a/b | SGA (<5th centile) | |
|---|---|---|---|---|---|---|---|---|
| % | % |
| % | % | Ratio | % | ||
| Most accurate formula | ||||||||
| Hadlock A6 | AC, HC, FL | −0.5 | 69 | Ref | 17 | 14 | 1.2 | 15 |
| Least accurate formula | ||||||||
| Kohorn | BPD | 13.8 | 35 | <0.001 | 60 | 5 | 12.0 | 1 |
| Other key formulas | ||||||||
| Hadlock B3 | AC, HC, FL | 1.0 | 68 | 0.465 | 21 | 11 | 1.9 | 13 |
| Stirnemann et al. | AC, HC | −3.7 | 66 | 0.192 | 13 | 21 | 0.6 | 16 |
| Hadlock B4 | AC, HC, BPD, FL | 1.8 | 69 | 0.879 | 22 | 9 | 2.5 | 13 |
| Outcome | Subgroup |
| Hadlock et al. B3 | Hadlock et al. A6 | Stirnemann et al. | Hadlock et al. B4 |
|---|---|---|---|---|---|---|
| LBW | BW < 5th centile | 48 | 81 | 92 | 89 | 86 |
| BW ≥ 5th centile | 402 | 14 | 17** | 24*** | 14 | |
| BW discordance | ≥18% | 144 | 30 | 34 | 42** | 32 |
| <18% | 306 | 16 | 20** | 25*** | 15 | |
| Chorionicity | Monochorionic | 102 | 18 | 21 | 28* | 18 |
| Dichorionic | 348 | 21 | 26** | 31*** | 21 | |
| Presenting twin | Presenting twin | 226 | 23 | 26 | 31** | 22 |
| Non‐presenting twin | 224 | 18 | 23* | 29*** | 20 | |
| Sex | Female | 215 | 27 | 31* | 33* | 27 |
| Male | 234 | 14 | 19* | 28*** | 15 | |
| Presentation at last ultrasound | Breech | 105 | 23 | 26 | 27 | 24 |
| Transverse | 57 | 25 | 30 | 32 | 27 | |
| Cephalic | 212 | 20 | 25* | 33*** | 19 | |
| HC/AC ratio | >1.1 | 61 | 49 | 54 | 70** | 51 |
| ≤1.1 | 389 | 15 | 19** | 23*** | 15 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Assisted Reproductive Technology and Twin Pregnancy · Prenatal Screening and Diagnostics
INTRODUCTION
1
Numerous formulas have been proposed for the estimation of fetal weight (EFW) in utero. EFW is a proxy for fetal size and, using birth weights as a basis for comparison, formulas have been developed using various combinations of measurements of fetal abdominal circumference (AC), head circumference (HC), femur length (FL) and biparietal diameter (BPD). Nevertheless, in practice, an EFW is interpreted as the actual in utero weight of a fetus. Owing to reduced growth velocity in the third trimester, and lower birth weights relative to singleton pregnancies,1, 2, 3, 4 accurate estimation of fetal weight in twins is desirable, particularly in the context of high rates of iatrogenic and spontaneous preterm delivery and evaluation for inter‐twin growth discordance. Serial determination of fetal weight is recommended by NICE,5 ISUOG,6 ACOG,7 RCOG8, 9 throughout pregnancy for both monochorionic and dichorionic twin gestations.
In the context of twin pregnancy, comparative studies have used a limited number of EFW formulas, without consensus on the most accurate formula.10, 11, 12, 13, 14 These studies were performed prior to development of the INTERGROWTH‐21st estimated fetal weight standard.15 In this study, we sought to compare the accuracy of a comprehensive set of fetal weight formulas,10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55 including formulas developed specifically for twin gestations.13, 14 We also sought to determine if a formula with optimal accuracy performs better than existing formulas, recommended for singletons, in the detection of low birth weight (LBW) for gestational age and for significant birth weight discordance.
MATERIALS AND METHODS
2
The prospective evaluation of sonographic predictors of restricted growth in twins study (ESPRiT Study53, 54, 55) was conducted at eight academic perinatal centers in Ireland, all with tertiary neonatal intensive care facilities. Institutional review board approval was obtained at each participating site and the study participants gave written informed consent. Inclusion criteria were all twin pregnancies presenting to the study centers between 11 and 22 completed weeks of gestation, with both fetuses alive at the time of enrolment, and with intact membranes. Monoamnionicity, a major structural abnormality in either twin, or fetal aneuploidy (either suspected or confirmed) led to exclusion from the study.
All patients who met the inclusion criteria underwent a program of intensive fetal surveillance carried out by dedicated research ultrasonographers using standardized ultrasonographic equipment (GE Voluson Expert 730; GE Healthcare Ultrasound, Milwaukee, Wisconsin). Chorionicity was assigned by standard ultrasonographic criteria at the first ultrasonographic evaluation and confirmed with placental pathology. A study‐specific pregnancy dating protocol was implemented across all centers.
Two‐weekly growth scans were performed from 16 weeks of gestation until delivery for monochorionic twin pairs and from 24 weeks until delivery in dichorionic pregnancies. Standard fetal biometry was recorded (abdominal circumference, biparietal diameter, head circumference, femur length). Biparietal diameter was assessed inner‐to‐outer and abdominal circumference and head circumference were assessed using the ellipse method. The Hadlock 4‐parameter formula (1985), which incorporates biparietal diameter, was used to determine estimated fetal weight, with other formulas used when a fetal biometry parameter was not available.22 A quality review system was in place which required weekly submission by ultrasonographers of images to a central ultrasonography quality assurance committee. All prenatal and ultrasonographic data were contemporaneously transferred to an ultrasonography software system (Viewpoint; MDI Viewpoint, Jacksonville, Florida), uploaded onto a live web‐based central consolidated database and screened for potential anomalous findings. Database quality reports were generated prospectively at regular intervals with a feedback loop between the data management team and the study‐dedicated sonographers.
Study population and evaluation
2.1
From the unselected prospective cohort of twins, we selected those twins with an ultrasound examination within 3 days of delivery. We evaluated the accuracy of EFW formulas in this group using several statistical measures and for their determination of small‐for‐gestational age (SGA) status. We then evaluated the association of SGA, defined by a variety of formulas, and the observation of low birth weight (LBW) for gestational age. The prevalence of SGA in subgroups of the study population was explored.
Formulas for comparison
2.2
We took a similar set of formulas considered by Hammami et al.56 in their assessment of singleton pregnancies, excluding those formulas targeting large‐for‐gestational age fetuses and pregnancies complicated by diabetes. In addition, we included the following formulas:
- Two formulas developed specifically for twins13, 14 both incorporating AC and FL alone.
- Seven alternative formulas proposed by Hadlock et al.22 that is, their earlier 1984 suite of formulas. To avoid potential confusion, the complete suite of formulas are presented in Table 1, with labels “A” and “B”. The Hadlock formula incorporating HC, AC and FL from the subsequent 1985 publication,23 formula B3, is commonly applied in singleton pregnancies.
- The volumetric formulas of Shinozuka39, 40 and Jackson et al.30 which include BPD for determination of EFW.
TABLE 1: The Hadlock suite of formulas from 1984 22 and 1985. 23
A total of 63 EFW formulas13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52 were compared. The required biometry inputs (in cm units) and generic code for all the formulas are provided as Appendix S1. Three key formulas are presented for comparison in the tables: the Hadlock B3 formula (commonly applied in singletons, which uses AC, HC and FL), the Stirnemann et al.15 formula (the INTERGROWTH‐21st standard, which uses AC and HC) and the Hadlock B4 formula (used prospectively in this study population and uses all four biometry parameters).
Measures of accuracy
2.3
To determine the proximity of the EFW determinations to birth weight, comparisons were made using percentage error (PE):
Median PE was used to rank the formulas from “most accurate” to “least accurate”. However, the percentage within 10% of birth weight (|PE| ≤ 10%) was also considered as a meaningful summary as this quantifies variability in PE. Formulas were then compared for agreement using McNemar's test for paired data. We assessed whether PE indicated overestimation of BW (PE > 10%) or underestimation of BW (PE < −10%) and summarized these results as a ratio.
Using the INTERGROWTH‐21st fetal growth chart standard for singletons,57 we defined small‐for‐gestational age (SGA) as EFW < 5th centile for each formula. The fifth centile was chosen as this is the lowest available centile from the INTERGROWTH‐21st standard.
Perinatal outcomes and subgroup comparisons
2.4
With SGA defined using the different EFW formulas, we sought to determine their predictive accuracy for low birth weight (LBW), defined as birth weight < 5th centile using the WHO‐UK standard.58, 59 The INTERGROWTH‐21st standard for birth weight60 was not considered because this reference range begins at 33 weeks' gestation. Predictive accuracy for birth weight discordance of ≥18% was also evaluated. In this study population, the 18% discordance in BW was found to be an independent predictor of adverse perinatal outcome.53 The sensitivity and false‐positive rate for the detection of LBW and BW discordance ≥18% was examined.
A comparative analysis of the most accurate formula and the three key formulas were examined for prevalence of SGA. The following fetal factors were considered in this analysis: chorionicity; fetal presentation; baby gender and HC/AC > 1.1. The cutoff of 1.1 for the HC/AC ratio was determined from the study by Grantz et al.2 as a potential indicator of growth disproportionality.
RESULTS
3
Among 1028 enrolled twin pregnancies, there were 15 congenital anomalies, 24 twin pairs with a previable single or dual death (gestational age at delivery <24 weeks or birth weight <500 g), 16 cases of twin‐twin transfusion syndrome (TTTS), eight pregnancies that delivered outside of a participating study center and 17 participants withdrew from the study. These cases were excluded from further analysis and, with some overlap in these criteria, resulted in 948 twin‐pairs for further evaluation. Of these, 226 twin‐pairs (452 fetuses) had an ultrasound examination within 3 days of delivery.
The median [IQR] maternal age was 33 [27, 39] years and the ethnicity of the study participants was primarily Caucasian (88%) in this subcohort. Body mass index (BMI, calculated as weight in kilograms divided by the square of height in meters) in excess of 30 at enrolment occurred in 15% of participants and 51% of participants were nulliparous. Monochorionic and dichorionic twins represented 23% and 77% of pregnancies, respectively. The rate of preterm delivery was 19% and the rate of SGA (EFW < 5th centile using the singleton standard) was 11% (Table 2).
A comparison of birth weights and estimated fetal weights in those with an ultrasound examination within 3 days of delivery is shown in Figure 1. EFW, as assessed using the Hadlock B4 and other formulas during the study, overestimates birth weights by a small degree on average (regression line) and this overestimation increases as birth weight levels increase in the study population.
Scatterplot of birth weight versus estimated fetal weight at last examination within 3 days of delivery (N = 452).
Comparison of fetal weight formulas
3.1
The full set of accuracy results, across all formulas considered, are provided as Appendix S1. Table 3 presents a select set of key comparisons from the 63 EFW formulas. The most accurate formula, as judged by median percentage error (MPE), is the earlier published Hadlock 3‐parameter formula that uses HC, AC and FL (Formula A6, Table 1).22 The MPE is −0.5%, indicating that this formula underestimates birth weight by a small percentage across the whole study population. A total of 69% of fetuses were within 10% of birth weight, with overestimation (PE > 10%) and underestimation (PE < −10%) of birth weight reasonably well balanced (17% and 14%, respectively). The percentage considered SGA < 5th centile was 15%.
The formula identified as least accurate was that of Kohorn33 and this finding was consistent across all the accuracy measures. The percentage within 10% of birth weight was 35% and this was statistically significantly (P < 0.001) when compared to the Hadlock A6 formula.
Two key comparisons were those of the Hadlock B4 formula (used in this study) and the Hadlock B3 formula (commonly used for singletons). Both of these formulas originate from the later 1985 paper by Hadlock et al.23 These show similar MPE, indicating a marginal overall overestimation of birth weight (1.8% and 1.0%, respectively) overall. These formulas also had similar percentages within 10% of birth weight (68% and 69%, respectively), not statistically significant when compared to the most accurate formula (Hadlock A6). However, overestimation (in excess of +10%) was approximately twice as likely to occur than underestimation (<−10%) with these formulas. This imbalance is reflected in the ratio of overestimation to underestimation, 2.5 and 1.9, for Hadlock B4 and B3, respectively. The percentage defined as SGA using these formulas were similar to the Hadlock B6 formula.
The INTERGROWTH‐21st formula (Stirnemann et al.15) was also included as a key comparator. The MPE was −3.7% and the percentage within 10% of birth weight was 66%, not statistically significant when compared to the most accurate formula. In contrast to the Hadlock formulas, this formula was almost twice as likely to underestimate rather than overestimate birth weights (ratio = 0.6), for twin examinations within 3 days of delivery. The percentage defined as SGA was 16% using this formula.
Using SGA defined for each formula as presented in Table 3, the detection rates for LBW (BW <5th centile) and significant birth weight discordance (≥18%) are presented in Table 4. The least accurate formula, that of Kohorn,33 was excluded from this analysis. All formulas exhibited high detection rates for LBW (>80%), with the Hadlock A6 and Stirnemann15 formulas having better sensitivity (92% and 89%, respectively) than the other formulas. The false positive rates (SGA percent for BW ≥5%) were higher for Hadlock A6 and Stirnemann15 formulas, 17% and 25%, respectively.
TABLE 4: Percent SGA (EFW < 5th centile) according to perinatal outcome and study subgroup.
Similar results are found when considering BW discordance ≥18% as an outcome. However, the Stirnemann15 formula has a higher detection rate (42%) when compared to the Hadlock A6 formula (34%). Fetal factors that may influence fetal weight estimation are also presented in Table 4.
In fetuses differing in proportionality, as illustrated by the HC/AC ratio, there was a significant disparity in SGA prevalence rates between the Stirnemann15 formula and the Hadlock formulas. In those with HC/AC > 1.1, the Stirnemann formula15 identified 70% as SGA, compared to approximately 50% for the Hadlock formulas.
DISCUSSION
4
Hadlock et al.22, 23 proposed several EFW formulas based on the availability of fetal biometric parameters. The applicability of Hadlock's formulas has been validated in diverse populations, from Rio de Janeiro61 to the eastern regions of Nepal.62 The INTERGROWTH‐21st standard for estimation of fetal weight15 was conducted with a strong ultrasound quality protocol for singleton pregnancies in six countries, bolstered by a comprehensive and robust statistical evaluation. It has been recommended as a prescriptive international standard to complement the WHO Child Growth Standards.63 This formula uses abdominal circumference and head circumference alone in the determination of fetal weight.
Several comparative studies10, 11, 12, 13, 14 of formulas for estimation of fetal weight in twins have been performed on a limited selection of formulas, prior to the introduction of the fetal weight formula by the INTERGROWTH‐21st consortium.
Summary of main findings
4.1
Our results suggest that the Hadlock A6 formula, which uses AC, HC and FL, performs better than the Hadlock B3 formula, which uses the same biometry parameters, in twin pregnancy. The same formula was identified by Khalil et al.12 as providing the most accurate representation of fetal size in twins.
Our results also indicate that the INTERGROWTH‐21st formula did not have a lower detection rate for LBW and performed better for detection of significant birth weight discordance than the Hadlock A6 or Hadlock B3 formulas. Where significance discordance in AC to HC might be evident, the INTERGROWTH‐21st formula is potentially a better alternative than the Hadlock formulas. The overall small degree of underestimation of birth weight might be ascribed to growth in the 3 days from ultrasound examination to delivery.
The limitations of our study are the small sample size of twins having an ultrasound within 3 days of delivery and the relative homogeneity of ethnicity in the study population. Strengths of the study were the prospective recruitment, assessment of fetal biometry and ascertainment of outcomes in an unselected population and the comprehensive set of EFW formulas considered for comparison, including the INTERGROWTH‐21st standard.
Implications for further research
4.2
In the context of research in twins, the Hadlock B3 formula for estimation of fetal weights seems well‐established. This formula has been used to determine references ranges in large twin populations,64, 65 to determine customized centiles in twins66 and has been combined with birth weights to determine a birth weight reference that seeks avoid biases associated with preterm delivery.67 Nevertheless, given the considerable overestimation relative to underestimation of birth weights in twins using the Hadlock B3 formula, it seems that the INTERGROWTH‐21st formula merits consideration for use in twin gestations. Further studies evaluating EFW formulas in more ethnically diverse populations, and the potential influence of chorionicity, may add to the evidence provided by our study.
CONCLUSION
5
We have identified that among 63 published formulas for the estimation of fetal weight, one of Hadlock's 1984 models (incorporating HC, AC and FL) performed better than the commonly used 1985 formula, in the prediction of birth weight in a prospectively recruited twin population. Our results also indicate that the INTERGROWTH‐21 standard should be explored further in twin gestations. In this study, the INTERGROWTH‐21st standard, which incorporates AC and HC, did not show lower detection rates for LBW. The frequency and intensity of twin ultrasound surveillance is such that restriction of ultrasound examination to two parameters in ultrasound could be recommended without a reduction in accuracy.
AUTHOR CONTRIBUTIONS
Patrick Dicker was responsible for data management, statistical analysis and manuscript writing. All other authors (Ronan Conroy, Fionnuala McAuliffe, Michael Geary, Sean Daly, John J. Morrison, Stephen Carroll, Fergal D. Malone, Fionnuala M. Breathnach) recruited patients for the study and/or provided input to manuscript preparation.
FUNDING INFORMATION
This study (secondary analysis) was conducted without funding.
CONFLICT OF INTEREST STATEMENT
The authors have no conflicts of interest.
Supporting information
Appendix S1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gielen M , Lindsey PJ , Derom C , et al. Twin‐specific intrauterine ‘growth’ charts based on cross‐sectional birthweight data. Twin Res Hum Genet. 2008;11:224‐235.18361725 10.1375/twin.11.2.224 · doi ↗ · pubmed ↗
- 2Grantz KL , Grewal J , Albert PS , et al. Dichorionic twin trajectories: the NICHD fetal growth studies. Am J Obstet Gynecol. 2016;215(2):221.e 1‐221.e 16.10.1016/j.ajog.2016.04.044PMC 496740227143399 · doi ↗ · pubmed ↗
- 3Giorgione V , Briffa C , Di Fabrizio C , Bhate R , Khalil A . Perinatal outcomes of small for gestational age in twin pregnancies: twin vs. singleton charts. J Clin Med. 2021;10(4):643. doi:10.3390/jcm 10040643 33567545 PMC 7916041 · doi ↗ · pubmed ↗
- 4Lin D , Rao J , Fan D , et al. Should singleton birth weight standards be applied to identify small‐for‐gestational age twins?: analysis of a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21(1):446.34172024 10.1186/s 12884-021-03907-1PMC 8234673 · doi ↗ · pubmed ↗
- 5National Institute for Health and Care Excellence . Twin and triplet pregnancy. 2019. https://www.nice.org.uk/guidance/ng 137. Accessed June 29, 2024.31513365 · pubmed ↗
- 6Khalil A , Rodgers M , Baschat A , et al. ISUOG practice guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol. 2016;47(2):247‐263. doi:10.1002/uog.15821 26577371 · doi ↗ · pubmed ↗
- 7American College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics , Society for Maternal‐Fetal Medicine . Multifetal gestations: twin, triplet, and higher‐order multifetal pregnancies: ACOG practice bulletin, number 231. Obstet Gynecol. 2021;137(6):e 145‐e 162.34011891 10.1097/AOG.0000000000004397 · doi ↗ · pubmed ↗
- 8Kilby MD , Baker PN , Critchley H , Field D . Multiple Pregnancy Study‐Group Statement: consensus Views Arising From the 50th Study Group. Royal College of Obstetricians and Gynaecologists. RCOG Press; 2006. ISBN 1‐904752‐22‐5.