Impact of severe intra‐abdominal adhesions on early maternal complications following cesarean delivery
Shai Ram, Hila Shalev‐Ram, Shira Alon, Shai Trigerman, Ariel Many, Yariv Yogev, Emmanuel Attali

TL;DR
Severe intra-abdominal adhesions increase the risk of early maternal complications after cesarean delivery.
Contribution
This study is the first large prospective observational analysis linking severe adhesions to specific maternal complications after cesarean delivery.
Findings
Women with severe adhesions had a 28% higher risk of maternal complications after cesarean delivery.
Severe adhesions were independently associated with increased need for blood or iron products and prolonged hospitalization.
No significant differences were found in fever, re-hospitalization, or emergency room visits between groups.
Abstract
The rising rates of cesarean delivery (CD), which are a leading cause of intra‐abdominal adhesions, represent a major concern for maternal health. We aimed to describe early maternal complications following CD in women with severe intra‐abdominal adhesions. A prospective observational study was conducted at a university‐affiliated tertiary medical center (January 2021 and March 2023) in Israel. Women who underwent CD were assessed for intra‐abdominal adhesions by questionnaires completed by the surgeons. Adhesions were evaluated at four anatomical sites: abdomen‐to‐uterus, uterus‐to‐bladder, skin‐to‐fascia, and other intra‐abdominal sites. Each site was scored on a scale of 0–2, with a total score ranging from 0 to 8. Severe adhesions were defined as a total score ≥5. The primary outcome measures were a composite complication which included at least one or more of postoperative need…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
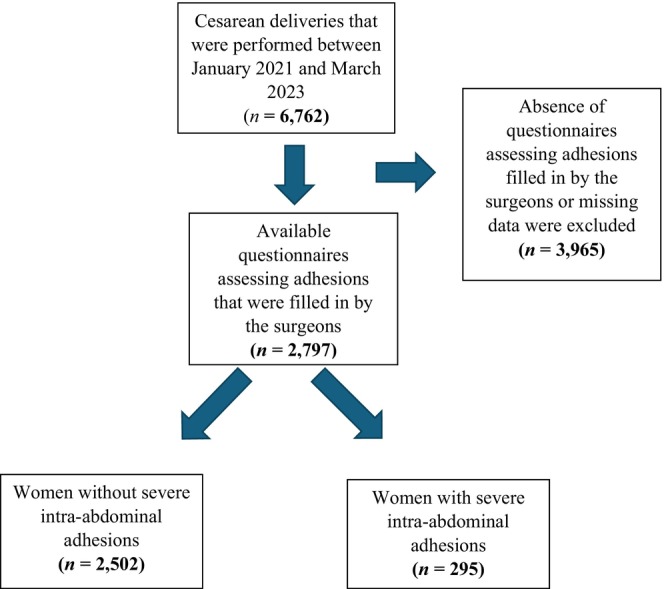 FIGURE 1
FIGURE 1| Variables | Overall | Severe adhesions (score ≥5) |
| |
|---|---|---|---|---|
| No | Yes | |||
| Number, | 2797 | 2502 (89.4) | 295 (10.6) | |
| Maternal age, years, mean (SD) |
|
|
|
|
| Pre‐pregnancy BMI, mean (SD) |
|
|
|
|
| Smoking status, | 137 (5.1) | 117 (4.9) | 20 (6.8) | 0.143 |
| Diabetes mellitus, | 70 (2.5) | 61 (2.4) | 9 (3.1) | 0.660 |
| Chronic hypertension, | 51 (1.8) | 43 (1.7) | 8 (2.7) | 0.329 |
| Adhesion score, mean (SD) |
|
|
|
|
| Previous CD, | ||||
| 0 |
|
|
|
|
| 1 |
|
|
| |
| 2 |
|
|
| |
| 3+ |
|
|
| |
| Gestational age at birth, mean (SD) |
|
|
|
|
| Birth weight (grams), mean (SD) | 3132 (572) | 3129 (570) | 3158 (597) | 0.429 |
| GWG, mean (SD) |
|
|
|
|
| Gestational diabetes mellitus, | 586 (21.0) | 518 (20.7) | 68 (23.1) | 0.389 |
| Gestational hypertension, | 125 (4.5) | 114 (4.6) | 11 (3.7) | 0.616 |
| ART, |
|
|
|
|
| Surgery time, mean (SD) |
|
|
|
|
| Prolonged surgery, |
|
|
|
|
| Maternal complications, | ||||
| Need for blood or iron products |
|
|
|
|
| Fever | 23 (0.8) | 18 (0.7) | 5 (1.7) | 0.087 |
| Re‐hospitalization | 71 (2.5) | 64 (2.6) | 7 (2.4) | 1.000 |
| Prolonged hospitalization |
|
|
|
|
| ER visits | 306 (10.9) | 275 (11.0) | 31 (10.5) | 0.879 |
| Variables | RR | CI 2.5% | CI 97.5% |
|
|---|---|---|---|---|
| Need for blood or iron products |
|
|
|
|
| Prolonged hospitalization |
|
|
|
|
| Composite complications |
|
|
|
|
| Re‐hospitalization | 0.932 | 0.43 | 2.01 | 0.858 |
| ER visits | 0.957 | 0.67 | 1.35 | 0.807 |
| Fever | 2.367 | 0.88 | 6.32 | 0.085 |
| Variables | OR | CI 2.5% | CI 97.5% |
|
|---|---|---|---|---|
| Severe adhesions |
|
|
|
|
| Previous CD | 0.798 | 0.60 | 1.04 | 0.105 |
| Diabetes mellitus | 1.607 | 0.89 | 2.87 | 0.109 |
| Chronic hypertension | 1.149 | 0.60 | 2.17 | 0.601 |
| Smoking status | 1.092 | 0.75 | 1.58 | 0.641 |
| Pre‐pregnancy BMI |
|
|
|
|
| Maternal age | 1.013 | 0.99 | 1.03 | 0.145 |
| Adhesions score | Abdomen–uterus | Uterus–bladder | Skin–fascia | Other sites |
|---|---|---|---|---|
| None–0, | 1559 (75.21) | 1468 (70.71) | 1369 (65.69) | 1827 (89.65) |
| Filmy–1, | 296 (14.28) | 390 (18.79) | 417 (20.01) | 141 (6.92) |
| Dense–2, | 218 (10.52) | 218 (10.5) | 298 (14.3) | 70 (3.43) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Hernia repair and management · Intestinal Malrotation and Obstruction Disorders
INTRODUCTION
1
Postoperative adhesions represent a frequent obstacle in abdominal surgeries.1 Cesarean deliveries (CDs) are prominent contributors to the development of intra‐abdominal adhesions among women of childbearing age.2 Given the ongoing rise in CD rates, now exceeding 30% in the US,3, 4 the occurrence of intra‐abdominal adhesions following CD has emerged as a matter of considerable concern. The occurrence of adhesions is closely linked to the number of prior CD, which is a primary risk factor for their formation.2, 5, 6, 10, 14 Approximately 25%–46% of cases exhibit adhesion formation following the first CD, with rates increasing to 43%–75% after the second CD and reaching as high as 83% after the third CD.2, 5, 6 Intra‐abdominal adhesions associated with CD have been linked to several complications, including bowel obstruction,2, 11 bladder and urinary tract injuries2, 12, 13 and prolonged delivery time.5, 6, 7 Furthermore, post‐CD adhesions can lead to increased blood transfusion requirements14 and serve as a risk factor for various gynecologic issues, such as infertility, an increased risk of ectopic pregnancy,2, 15, 16 chronic pain,15 and a rise in the rate of re‐hospitalizations.8
Considering the high prevalence of intra‐abdominal adhesions following CD and the resultant risk of substantial maternal complications, together with the scarcity of existing research on this topic, we aimed to delineate the early postoperative complications in women with severe intra‐abdominal adhesions.
MATERIALS AND METHODS
2
Study design
2.1
This was a prospective observational study designed to assess early maternal post‐CD complications encountered by women with intra‐abdominal adhesions. All consecutive women, for whom the surgeon complete the questionnaires, and underwent a CD between January 2021 and March 2023 at a single university affiliated tertiary center in Israel, were included in the study population. The study was approved by the local institutional review board (0579‐21 TLV).
Adhesions were assessed and recorded by questionnaires that were filled out by surgeons immediately after each CD. This questionnaire is described and validated in our previous study,17 and addressed four main anatomical sites: (1) abdomen‐to‐uterus, (2) uterus‐to‐bladder, (3) skin‐to‐fascia, and (4) other (adhesions in the ovarian area, omentum, intestine, or any other intra‐abdominal site). The surgeons were asked to rank the observed adhesions between zero and two: none (score = 0), filmy (score = 1), or dense (score = 2). Filmy adhesions were defined as those that are weak and therefore easily removed without the need of a device, whereas the removal of dense adhesions required scissors, scalpels, or diathermy. The total score for the four sites could range between 0 and 8. The score of 5 and above was considered as a severe degree of adhesions. Women for whom the surgeon did not complete the questionnaires or there was missing information regarding the preoperative, intraoperative, or primary outcome variables, were excluded.
The data that were extracted from electronic medical records included details of maternal medical history, background morbidity, CD, and surgical details. Gestational weight gain (GWG) was determined by computing the difference between the woman's pregestational weight and her weight at the time of admission for the index CD. The duration of surgery was calculated as the time that had elapsed from the initiation of the incision to the conclusion of the operation. Prolonged surgery time was defined as duration surpassing the 90th percentile.
The main outcome measures were risk factors for maternal complications, which encompassed the following criteria: postoperative need for blood or iron products during hospitalization, fever as indicated by a body temperature exceeding 38.0°C during postoperative hospitalization and requiring antibiotic treatment, prolonged hospitalization as defined by postoperative hospital stays exceeding the 90th percentile, re‐hospitalization and emergency room visits within 30 days following hospital discharge. Re‐hospitalization and emergency room visits referred to hospitalization in the gynecology department and visits to the gynecology emergency department, respectively. Composite complication was considered if any one or more of these complications occurred.
Statistical analysis
2.2
Descriptive statistics were used to assess the distribution of variables. Continuous variables are summarized as mean values with standard deviations, and categorical variables are summarized as counts and percentages. The comparison between the study groups, women with severe adhesions and those without, was conducted using a Chi‐square for categorical variables and a t‐test for continuous variables. The risk ratio (RR) was calculated for each complication separately and for all complications as a composite outcome, comparing the population of women with severe adhesions (score ≥5) to those with non‐severe adhesions (≤4) by a logit model, with 95% confidence interval (CI). Finally, in order to determine whether severe adhesions constitute an independent risk factor for the maternal complications, a univariate analysis was performed for the composite complications. Variables with a P value of less than 0.05, were included in a multivariate model to calculate the odds ratio (OR). The analyses were carried out using Python version 3.73. Significance was defined as a P value of less than 0.05.
RESULTS
3
Overall, during the study time, 6762 CDs were performed at our medical center, and the questionnaires assessing for adhesions were filled for 2797 CDs which were included in this study. There were 295 cases (10.6%) of severe adhesions (Figure 1). The characteristics of the study population are presented in Table 1. The mean maternal age in the study group as well as the pre‐pregnancy body mass index (BMI, calculated as weight in kilograms divided by the square of height in meters) were significantly higher compared to women without severe adhesions (35.9 vs. 34.6, P < 0.001 and 25.2 vs. 24.1, P = 0.003, respectively). There were no significant differences in smoking status, diabetes mellitus, or chronic hypertension between the two groups.
Flow chart of the study participants.
Other notable group differences included gestational age at birth (38.2 vs. 38.6, P < 0.001) and gestational weight gain (4.2 vs. 7.5 kg, respectively, P = 0.022). Furthermore, the severe adhesions group had higher rates of prolonged surgery duration (in 26.1% vs. 20.0%, P = 0.041) and prolonged hospitalization (14.2% vs. 9.6%, P = 0.015), (Table 1). Prolonged surgery duration and prolonged hospitalization, both defined in the methods section as time exceeding the 90th percentile, were found to be more than 79 min for surgery duration and over 4.58 days for hospitalization, respectively.
Table 2 describes the risk ratio for each complication in women with severe intra‐abdominal adhesions compared to those without and the risk for composite complication. Women with severe intra‐abdominal adhesions had a significantly higher need for postoperative blood or iron products administration (RR = 1.71, 95% CI: 1.15–2.55, P = 0.007) as well as more prolonged hospitalization (RR = 1.49, 95% CI: 1.10–2.03, P = 0.009). The risk for composite complication was also higher in the severe adhesions group (RR = 1.28, 95% CI: 1.12–1.45, P < 0.001). There were no significant group differences in re‐hospitalization, emergency room visits, or post‐CD fever. Table 3 describes a multivariate analysis conducted to characterize variables that independently affect maternal complications. It can be observed that even in the multivariate analysis, the most significant factor is severe adhesions (OR = 1.444, CI: 1.06–1.95, P value 0.017).
Table 4 presents the adhesion scores across different anatomical sites observed during cesarean delivery and rated by the surgeons.
DISCUSSION
4
The findings of the current study revealed a significant association between severe intra‐abdominal adhesions following CD with maternal complications, specifically the need for blood or iron products, and prolonged postoperative hospitalization.
The correlations between the severity of adhesions following CD and maternal complications have not been thoroughly investigated in the existing literature. Most of the reports in the literature refer to maternal complications after repeat CD5, 6, 9, 10, 11 and not specifically to those associated with the presence or severity of adhesions. However, several reports have correlated severe adhesions with repeat CD.2, 5, 6, 10, 14 Tulandi et al.5 reviewed the medical records of 1283 women who underwent repeat CD and showed that increased adhesion development and a longer time to delivery were found with each subsequent CD. However, complication rates in the repeat CDs of those women were comparable with primary CD. In contrast, Silver et al.10 conducted a prospective observational cohort of 30 132 women who had CD, and found that blood transfusion, the duration of operative time and hospital stay significantly increased with increasing number of CD. Makoha et al.9 also found that morbidity increased with successive CDs before and through the third CD. Neither of those studies showed correlation between the number of CD and the occurrence of post‐CD fever, as did this study.
In addition, previous studies examined the impact of prolonged surgery duration on postoperative maternal complications,18, 19, 20 which were defined similarly to our study, as time exceeding the 90th percentile. Those studies found that prolonged surgery is an indicator for maternal complications such as the need for blood transfusions, prolonged hospitalization, infection necessitating antibiotics, and readmission.18, 19, 20 In the present study, women with severe adhesions had a longer surgery duration and a higher rate of prolonged surgery, which may explain the association between severe intra‐abdominal adhesions following CD with maternal complications that were found.
Since repeat CD correlated with maternal complications and with intra‐abdominal adhesions, it is logical to examine if severe adhesions may participate as a main cause for post‐CD complications. Taken together, these findings emphasize the importance of identifying women who are at risk for severe adhesions, given the expectation of a post‐CD course that bears a higher risk for maternal complications. Anticipating such complications following CD may enable expeditious implementation of appropriate management.
CDs are characterized by intraoperative complications primarily involving damage to adjacent organs, such as the bladder, intestines, vascular injury, significant bleeding, and infections.21 In this study, we examined early complications, which may be derivatives of these intraoperative complications and were thus selected for analysis. However, the study did not consider women who required a relaparotomy. Although this factor may be reflected in prolonged hospitalization and the need for blood transfusions, which are identified as complications associated with severe adhesions, it was not examined independently. Furthermore, the data was not available for the 3965 excluded due to missing data since questionnaires assessing adhesions were not filled in by the surgeons and thus could not be compared to the sample of participants included. Additionally, various factors that could influence maternal complications were not considered, such as the urgency of the surgery, prolonged rupture of membranes, blood loss estimation during the surgery, maternal complications in previous deliveries, and the results of preoperative laboratory tests. Finally, other specific morbidities that may be correlated with severe adhesions, such as bladder, bowel, and ureteric injury, were not examined in our study.
Notable advantages of the present study are its prospective design, the large sample size, the fact that the analyses were based upon multiple potential risk factors for maternal complications and the use of a validated scoring system for post‐CD adhesion assessment.17
CONCLUSION
5
This study demonstrates the significant impact of severe intra‐abdominal adhesions following CD with an increased risk of early maternal complications. These findings underscore the importance of identifying women at risk for severe adhesions that may guide efforts to reduce post‐surgical complications. Further research is required to substantiate these findings and explore measures to contain adhesion severity.
AUTHOR CONTRIBUTIONS
Shai Ram: Design, planning, conduct, data analysis and manuscript writing. Hila Shalev Ram: Design, planning and manuscript writing. Shira Alon: Planning, conduct and data analysis. Shai Trigerman: Design, planning, conduct and manuscript writing. Ariel Many: Design, conduct, planning and manuscript writing. Yariv Yogev: Design, planning and manuscript writing. Emmanuel Attali: Design, planning and manuscript writing.
FUNDING INFORMATION
None.
CONFLICT OF INTEREST STATEMENT
The authors report no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Wilde RLTG . Postoperative abdominal adhesions and their prevention in gynaecological surgery expert consensus position. Part 2—steps to reduce adhesions. Gynecol Surg. 2007;4(4):243.
- 2Awonuga AO , Fletcher NM , Saed GM , Diamond MP . Postoperative adhesion development following cesarean and open intra‐abdominal gynecological operations: a review. Reprod Sci. 2011;18(12):1166‐1185. doi:10.1177/1933719111414206 21775773 PMC 3343100 · doi ↗ · pubmed ↗
- 3Cole SK . Cesarean section rates. Lancet. 1980;315(8168):606. doi:10.1016/S 0140-6736(80)91104-6 6102336 · doi ↗ · pubmed ↗
- 4Michas F . Cesarean sections in selected countries 2018. 2021 https://www.statista.com/statistics/283123/cesarean‐sections‐in‐oecd‐countries/
- 5Tulandi T , Agdi M , Zarei A , Miner LSV . Adhesion development and morbidity after repeat cesarean delivery. Am J Obstet Gynecol. 2009;201:56. e 1‐56. e 6.10.1016/j.ajog.2009.04.03919576375 · doi ↗ · pubmed ↗
- 6Morales KJ , Gordon MC , Bates GW . Postcesarean delivery adhesions associated with delayed delivery of infant. Am J Obstet Gynecol. 2007;196(5):461.e 1‐461.e 6. doi:10.1016/j.ajog.2006.12.017 17466702 · doi ↗ · pubmed ↗
- 7Shenhav S , Grin L , Kapustian V , Anteby EY , Gdalevich M , Gemer O . Quantifying the effects of postcesarean adhesions on incision to delivery time. J Matern Neonatal Med. 2019;32(15):2500‐2505. doi:10.1080/14767058.2018.1439010 29415600 · doi ↗ · pubmed ↗
- 8Hesselman S , Högberg U , Råssjö EB , Schytt E , Löfgren M , Jonsson M . Abdominal adhesions in gynaecologic surgery after caesarean section: a longitudinal population‐based register study. BJOG. 2018;125(5):597‐603. doi:10.1111/1471-0528.14708 28444984 · doi ↗ · pubmed ↗