Neurological Manifestations of HEV Infection: A Rare Phenomenon or an Underrecognized Reality?
Maider Iza, Daniel Ramos, Arnau Llauradó, Juan Luis Restrepo‐Vera, Mercedes Pallero, Galo Granados, Jose Alemany, Javier Sotoca, Júlia Sampol, Sergi Martí, Daniel Sanchez‐Tejerina, Maria Salvadó, Raul Juntas

TL;DR
This paper reports two cases where hepatitis E virus (HEV) caused neurological issues, suggesting HEV might be a rare but under-recognized cause of such conditions.
Contribution
The study highlights HEV as a potential cause of rare neurological manifestations through detailed clinical case descriptions.
Findings
HEV can cause neuralgic amyotrophy with diaphragmatic paralysis, as seen in a 43-year-old male.
HEV can lead to acute meningoradiculitis, as observed in a 37-year-old male with neurological symptoms and liver dysfunction.
Abstract
This study aimed to describe neurological manifestations secondary to hepatitis E virus (HEV) through the description of two clinical cases. Two different cases of neuralgic amyotrophy and meningoradiculitis are evaluated in the emergency department of a tertiary referral hospital in 2024. Case 1: A 43‐year‐old male presented to the emergency department with proximal weakness and pain in the right upper extremity associated with acute onset of orthopnea. Laboratory tests revealed elevated AST/ALT levels (184/1164 IU/L) and positive HEV IgM and IgG, with detectable serum HEV viral load. Cerebrospinal fluid (CSF) was negative for HEV RNA. A significant decrease in forced vital capacity was observed on transition from the upright to the supine position. Electromyography showed severe bilateral phrenic nerve involvement. The diagnosis of neuralgic amyotrophy with diaphragmatic paralysis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1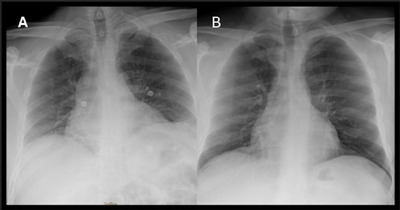 FIGURE 2
FIGURE 2| Patient 1 | Patient 2 | |
|---|---|---|
| Demographic features | ||
| Age at onset | 43 years | 37 years |
| Sex | Male | Male |
| Immunocompetent | Yes | Yes |
| Clinical symptoms and course | Pain and weakness in right arm. Dyspnea and orthopnea | Paresthesia and weakness in upper and lower limbs |
| Antecedent events | Ingestion of undercooked meat | Ingestion of undercooked meat |
| Clinical phenotype | Bilateral, right > left |
Bilateral, right upper limb > left upper limb Left lower limb > right lower limb |
| Clinical course and outcome at outpatient basis | No longer pain, residual weakness and dyspnea | Full recovery |
|
Weakest muscles at outpatient basis | Deltoid muscle, right > left | None |
| mRS scale at onset | 2 | 1 |
| mRS scale at outpatient basis | 1 | 0 |
| Biochemical and virologic studies | ||
| Timing (days after symptom onset) | 1 | 4 |
| AST (8–34 IU/L) | 184 | 238 |
|
ALT (10–49 IU/L) FA (46–116 IU/L) GGT (7–73 IU/L) |
1164 221 223 |
626 181 399 |
| Bilirubin (0.30–1.20 mg/dL) | 0.33 | 1.48 |
| Autoimmune study | ANA and anti‐SSA (Ro60) positive | Negative |
| Anti‐HEV | IgM and IgG positive | IgM and IgG positive |
| Initial HEV viral load, log IU/mL | 83,000 IU/mL | 22,000 IU/mL |
| HEV viral load, log IU/mL at outpatient basis | Negative | 86 IU/mL |
| CSF analysis | ||
| Basic parameters | No pleocytosis, mild hyperproteinorrachia of 74 mg/dL |
Pleocytosis of 55 cells/µL with 100% lymphocytes, mild hyperproteinorrachia of 113 mg/dL |
| HEV RNA | Positive | Positive |
| Neurophysiological study | ||
| Pattern | Demyelinating | Not altered |
| Most affected nerves | Right long thoracic nerve and bilateral phrenic nerves | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis Viruses Studies and Epidemiology · Liver Disease and Transplantation · Macrophage Migration Inhibitory Factor
Introduction
1
Hepatitis E virus (HEV) is a significant contributor to liver disease worldwide, accounting for up to 70% of adult sporadic hepatitis cases in endemic regions (Iqbal et al. 2023). In developed countries, it is primarily transmitted to humans through the consumption of contaminated meat or water contaminated with fecal matter (Goel and Aggarwal 2017; Kenney and Meng 2019; Aslan and Balaban 2020).
Recent studies have shed light on the extrahepatic manifestations of HEV infection, particularly its neurological complications such as neuralgic amyotrophy (NA) or Parsonage–Turner syndrome (PTS), Guillain–Barré syndrome (GBS), encephalitis/myelitis, mononeuritis multiplex or meningoradiculitis (Ripellino et al. 2018; Woolson et al. 2014; Dalton et al. 2016; Jha et al. 2021). The current recommended approach for neurological complications is to modulate the immune response that typically involves using intravenous immunoglobulin (IVIG) administered over 5 days, with a dosage of 2 g/kg (Abravanel et al. 2018). There is also some evidence supporting the use of prednisolone with a gradual tapering off (Ripellino et al. 2019; Van Eijk et al. 2009).
Patients and Methods
2
A comprehensive description is provided for two cases of patients admitted to the University Hospital of Vall d'Hebron, Barcelona, Spain. Data were collected from the medical histories of the two patients after prior informed consent.
Case Report 1
2.1
A 43‐year‐old man with a medical history of type 2 diabetes, hypertriglyceridemia, psoriasis, and schizophrenia consulted at the emergency department on March 24 due to pain in both upper limbs and right brachial weakness, associated with sudden dyspnea and orthopnea. The patient did admit to having previously eaten undercooked pork meat. The physical examination showed no indications of liver failure. He had slight weakness of the right deltoid muscle as well as right right‐winged scapula (Figure 1). Bilateral diaphragmatic elevation was observed on the chest x‐ray (Figure 2). The blood analysis depicted hepatic cytolysis and mild cholestasis (Table 1). EBV, HAV, HBV, HCV, HIV, CMV, Coxiella burnetii, and Toxoplasma gondii were excluded. HEV serology resulted in positive IgM and HEV RNA positive (83,000 International Unit [IU]/mL). We did not perform HEV genotype sequencing. CSF analysis showed mild hyperproteinorrachia of 74 mg/dL and no pleocytosis. HEV RNA analysis yielded a negative result in the CSF. An electrophysiological study revealed impairment of the right long thoracic nerve and severe neuropathy of both phrenic nerves, characterized by significantly reduced amplitudes and prolonged distal latency. Respiratory function tests revealed a 49.8% forced vital capacity decrease from upright to supine position (from 2.66 to 1.34 L) (Table 1).
Physical examination of patient #1 showing right winged scapula, amyotrophy in supraspinatus and infraspinatus fossae, and abduction impairment.
Chest x‐ray performed in patient #1. (A) Chest x‐ray: April 6, 2024: Mild elevation of both diaphragms. (B) Chest x‐ray: August 3, 2024: No elevation can be observed in diaphragms.
Thus, the diagnosis of NA with diaphragmatic paralysis secondary to HEV was made. Treatment consisted of IVIG at a dose of 0.4 g/kg/day for 5 days and noninvasive mechanical ventilation. Corticosteroid therapy was not applied due to active viral replication. Ribavirin was also not administered.
During his hospital stay, the HEV viral load in the blood decreased progressively to undetectable levels. Liver function parameters also normalized. In addition, the patient experienced neurological improvement with increased strength and decreased pain. Given the patient's favorable progression, he was discharged from the hospital on April 16.
Three months later, at the time of the last assessment, he still experienced a slight difficulty in arm abduction. Additionally, he required the use of noninvasive mechanical ventilation during sleep and naps.
Case Report 2
2.2
A 37‐year‐old male with no significant past medical history presented to the emergency department on March 21 with a 10‐day history of tingling and weakness that began in the hands and progressed to the arms, followed by similar symptoms in the lower extremities, beginning in the feet and progressing proximally to the thighs. The patient acknowledged having previously consumed undercooked pulled pork. Physical examination did not show any signs of liver failure. Two days prior to the onset of these symptoms, he had experienced a self‐limited episode of diarrhea.
During physical examination, the patient had a slight distal weakness in flexors and extensors of the wrist and in the interosseus muscles of the right upper limb and a slight proximal weakness in quadriceps and hamstring of the lowers limbs. The reflexes were absent. Additionally, the patient exhibited hypoesthesia in the distal regions of both the upper and lower extremities.
The blood analysis showed hepatic cytolysis and cholestasis. Blood tests rendered a positive result for HEV IgM antibodies and a positive HEV PCR (22,000 IU/mL). We did not carry out HEV genotype sequencing. Serologic analysis showed negative results for HIV, HAV, HBV, and HCV.
A posterior lumbar puncture and CSF analysis revealed pleocytosis of 55 cells/µL with 100% lymphocytes and mild hyperproteinorrachia of 113 mg/dL. Additionally, the CSF was positive for HEV RNA, with a viral load of 250 IU/mL. An electrophysiological study was also performed that exhibited normal sensoy and motor nerve conduction, along with normal F responses and somatosensory evoked potentials (SSEP) (Table 1).
The cerebral and spinal MRI was not performed due to the subsequent rapid clinical recovery of the patient, although the findings of areflexia and distal sensory deficit led us to suspect a probable polyradiculopathy. Therefore, a diagnosis of meningoradiculitis due to HEV was made. IVIG (0.4 g/kg/day for 5 days) was initiated. He did not receive corticosteroid therapy due to ongoing viral replication; ribavirin was neither associated. Five days after initiating treatment, he reported an almost complete resolution of symptoms. During his hospital stay, the levels of transaminases were gradually normalized, and viral load of HEV in plasma was also reduced (viral load of 2100 IU/mL on March 25). Thus, the patient was discharged on March 26.
In the follow‐up visit 2 weeks after hospital discharge, he had a completely normal neurological examination. The blood analysis showed almost normal levels of AST and ALT at 44 IU/L and 97 IU/L, respectively. HEV replication was also reduced, with a viral load of 86 IU/mL.
Discussion
3
Neurological complications have been previously reported in individuals infected with HEV, including GBS, NA, encephalitis, myelitis, and meningoradiculitis (Dalton et al. 2016). Recent research has also explored the relationship between HEV exposure and chronic inflammatory demyelinating polyneuropathy (CIDP) (Pischke et al. 2024).
In our two patients, the liver function abnormalities were mild and neither had clinical jaundice. Both patients developed HEV‐associated neurologic manifestations following an acute onset. This highlights the importance of considering viral hepatitis as a diagnostic possibility even when clinical or biochemical signs are subtle, a point that has been highlighted in previous studies (Mclean et al. 2017).
The patient affected by NA had bilateral brachial plexus involvement leading to secondary diaphragmatic paralysis. This finding is consistent with previous reports (Van Eijk et al. 2017; Scanvion et al. 2017). Electrophysiological examination revealed a patchy multineuropathy previously described in NA and HEV (Velay et al. 2017). Although phrenic nerve involvement has been noted (Scanvion et al. 2017), it is crucial to emphasize the severe and acute nature of the involvement in this case, which required the implementation of noninvasive mechanical ventilation.
The patient with meningoradiculitis presented with paresthesias and weakness in the four limbs. Other studies have also reported an association between HEV and meningoradiculitis (Perrin et al. 2015; Kamar et al. 2010). It is important to highlight in our patient the clear alteration of CSF characterized by lymphocytosis and a high level of protein, despite the EMG results being entirely normal. It is also important to highlight that due to the significant clinical improvement exhibited by the patient, a cerebral or spinal MRI was not conducted. This decision could be considered a potential limitation in this case.
However, the first patient had a positive HEV viral load in the CSF, we did not observe this in the second patient. This indicates the two hypotheses: one could be that HEV has a preference for neuronal tissue due to neurotropic variants, and the other one would be that it is an immune‐mediated entity, resulting in cross‐reactions between viral epitopes and self‐antigens (Perrin et al. 2015; Abravanel et al. 2018; Fousekis et al. 2020). Unfortunately, there was no evaluation conducted on the intrathecal synthesis of anti‐HEV IgM in the CSF.
The first patient did show seroconversion after 1 month of clinical onset, whereas the second patient still showed positivity for HEV RNA after 2 weeks of clinical onset. This is due to the fact that HEV RNA is detected in the bloodstream for approximately only 4 weeks, while IgM+ can be detected for a longer period of 6–9 months (Kamar et al. 2017; Huang et al. 2010). This also means that patients who are referred late to the neurologist may present a negative HEV PCR and it should be taken into account when assessing these patients.
Both the patients were treated with IVIG. There is not much evidence regarding immunomodulatory treatment in patients with HEV and neurological complications, although some reports have been published where an improvement in neurological symptoms has been observed (Perrin et al. 2015; Abravanel et al. 2018; Silva et al. 2016).
In conclusion, this study delineates two cases that support the causal relationship between HEV and neurological complications. Clinicians should have a low threshold for testing HEV in patients with unexplained neurological symptoms and abnormal liver function test results. Early diagnosis and immunomodulatory treatment may lead to a better prognosis, reducing the chances of long‐term neurological complications.
Author Contributions
Maider Iza: conceptualization, data curation, formal analysis. Daniel Ramos: data curation, formal analysis. Arnau Llauradó: conceptualization, data curation, formal analysis, investigation, project administration. Juan Luis Restrepo‐Vera: methodology, project administration. Mercedes Pallero: resources, supervision. Galo Granados: resources, supervision. Jose Alemany: methodology, project administration. Javier Sotoca: investigation, methodology, project administration. Júlia Sampol: resources, supervision. Sergi Martí: resources, validation. Daniel Sanchez‐Tejerina: conceptualization, data curation, investigation, methodology, project administration. Maria Salvadó: conceptualization, data curation, formal analysis, investigation, methodology, project administration. Raul Juntas: conceptualization, data curation, formal analysis, investigation, methodology, project administration.
Ethics Statement
We confirm that we have read the journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Consent
Patients consented for the publication of details.
Conflicts of Interest
The authors declare no conflicts of interest.
Peer Review
The peer review history for this article is available at https://publons.com/publon/10.1002/brb3.70585
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abravanel, F. , J. Pique , E. Couturier , et al. 2018. “Acute hepatitis E in French Patients and Neurological Manifestations.” Journal of Infection 77, no. 3: 220–226.29966614 10.1016/j.jinf.2018.06.007 · doi ↗ · pubmed ↗
- 2Aslan, A. T. , and H. Y. Balaban . 2020. “Hepatitis E Virus: Epidemiology, Diagnosis, Clinical Manifestations, and Treatment.” World Journal of Gastroenterology 26, no. 37: 5543–5560.33071523 10.3748/wjg.v 26.i 37.5543 PMC 7545399 · doi ↗ · pubmed ↗
- 3Dalton, H. R. , N. Kamar , J. J. J. Van Eijk , et al. 2016. “Hepatitis E Virus and Neurological Injury.” Nature Reviews Neurology 12: 77–85.26711839 10.1038/nrneurol.2015.234 · doi ↗ · pubmed ↗
- 4Dalton, H. R. , G. W. Webb , B. C. Norton , and K. L. Woolson . 2016. “Hepatitis E Virus: Time to Change the Textbooks.” Digestive Diseases 34: 308–316.27170383 10.1159/000444468 · doi ↗ · pubmed ↗
- 5Fousekis, F. S. , I. V. Mitselos , and D. K. Christodoulou . 2020. “Extrahepatic Manifestations of Hepatitis E Virus: An Overview.” Clinical and Molecular Hepatology 26, no. 1: 16–23.31601068 10.3350/cmh.2019.0082 PMC 6940480 · doi ↗ · pubmed ↗
- 6Goel, A. , and R. Aggarwal . 2017. “Advances in Hepatitis E. II Epidemiology, Clinical Manifestations, Treatment and Prevention.” Expert Review of Gastroenterology & Hepatology 10: 1065–1074.10.1080/17474124.2016.118536527148907 · doi ↗ · pubmed ↗
- 7Huang, S. , X. Zhang , H. Jiang , et al. 2010. “Profile of Acute Infectious Markers in Sporadic Hepatitis E.” P Lo S ONE 5, no. 10: e 13560.21042408 10.1371/journal.pone.0013560 PMC 2958841 · doi ↗ · pubmed ↗
- 8Iqbal, H. , B. F. Mehmood , A. Sohal , and M. Roytman . 2023. “Hepatitis E Infection: A Review.” World Journal of Virology 12, no. 5: 262–271.38187497 10.5501/wjv.v 12.i 5.262PMC 10768387 · doi ↗ · pubmed ↗