Cutaneous macroglobulinosis with Waldenström macroglobulinemia and Bing-Neel syndrome: A case report
Amir Khogeer, Alain Dupuy

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2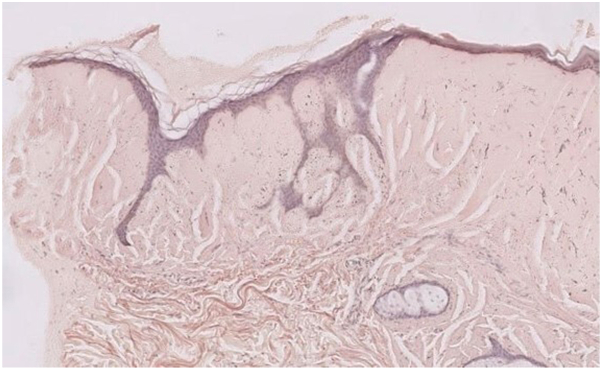 Figure 3
Figure 3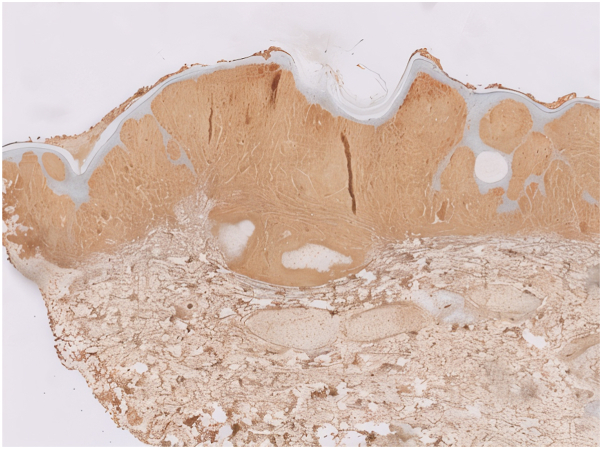 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Immunodeficiency and Autoimmune Disorders · Lymphoma Diagnosis and Treatment
Introduction
Waldenström macroglobulinemia (WM) is a lymphoproliferative neoplasm of B cells characterized by small lymphocytes and monoclonal IgM gammopathy.1 Specific cutaneous manifestations related to WM, collectively termed cutaneous macroglobulinosis (CM), result from neoplastic B-cell infiltration and monoclonal IgM deposition in the skin.2 Bing-Neel syndrome (BNS) is a rare neurological manifestation of WM characterized by lymphoplasmacytic infiltration into the leptomeningeal tissue and/or the central nervous system.3 More than 100 cases of BNS have been reported, including those documented by Simon et al (44 cases) and Ina Ly et al (36 cases).4^,^5
This article details the case of a 55-year-old male with CM secondary to WM, who later developed BNS. This is among the few documented cases of a patient presenting with WM, CM, and BNS simultaneously.
Case report
A 55-year-old male presented with diffuse skin infiltration affecting the hands, forearms, arms, and neck, characterized by multiple flesh-colored and dark micropapules. Three years earlier, he had been diagnosed with anti-myelin-associated glycoprotein paraprotein neuropathy related to Waldenström macroglobulinemia following peripheral neuropathy in the lower limbs. Skin examination revealed flesh-colored to dark micropapules across the hands, forearms, arms, neck, knees, chest, and face, with no lymphadenopathy or hepatosplenomegaly (Figs 1 and 2).Fig 1. Flesh-colored, translucent papules grouped into plaque located on the elbow.Fig 2. Dark, translucent papules grouped into plaque located on the knee.
Blood tests showed hemoglobin at 13.8 g/dL, platelets at 352 × 10^9^/L, and leukocytes at 11.3 × 10^9^/L. Serum electrophoresis revealed a monoclonal peak in the β2 region with significantly elevated IgM levels (33 g/L).
A skin biopsy revealed positive Periodic Acid–Schiff staining, negative Congo red staining, and a markedly thinned epidermis with ridge stretching. The dermis was filled with abundant hyaline material and demonstrated perivascular lymphocytic infiltration, neovascularization, and eosinophilic deposits (Fig 3). Immunohistochemical examination showed strong IgM positivity, confirming the diagnosis of CM associated with WM (Fig 4).Fig 3. Histopathologic features of the skin biopsy showing positive Periodic Acid–Schiff staining with hyaline material in the dermis, perivascular lymphocytic infiltration, and neovascularization (H&E, ×200).Fig 4. Immunohistochemical staining demonstrating strong positivity for IgM in the dermis (IgM IHC, ×200).
The patient was diagnosed with CM associated with WM and started on 2 cycles of RCD (rituximab, cyclophosphamide, and dexamethasone). He was referred to the oncology department, where treatment was initiated.
After the first 2 cycles, he reported progressive cognitive, memory, hearing, and visual impairments. BNS was suspected. A magnetic resonance imaging scan with gadolinium revealed no morphological abnormalities or suspicious contrast enhancement in the brain or meninges. A lumbar puncture with flow cytometry revealed lymphoplasmacytic cells with clonality, confirming the diagnosis of BNS. The patient’s treatment regimen was adjusted, replacing cyclophosphamide with fludarabine, given its superior meningeal penetration. He received 6 cycles of rituximab and intrathecal injections. Over time, the patient reported gradual improvements in cognitive, visual, and auditory functions, along with a progressive regression of cutaneous lesions. Six months post-therapy, laboratory evaluation showed serum IgM: 2.7 g/L and a normal lumbar puncture revealing rare nonatypical lymphocytes and no proteinorrhagia (0.71 g/L).
Discussion
CM is a rare manifestation of WM, occurring in approximately 5% of cases.2 CM often mirrors IgM levels and disease activity. In this case, CM regressed with effective treatment for WM and BNS, supporting its role as a marker of disease progression.
BNS, a rare complication of WM, typically arises after WM diagnosis and has varied clinical presentations, often delaying diagnosis.3
According to the classification proposed by Ina Ly et al, BNS can be divided into 2 subtypes: type A, characterized by direct neoplastic infiltration of the CNS, and type B, associated with IgM deposition leading to immune-mediated damage. Based on the presence of clonal lymphoplasmacytic cells in the cerebrospinal fluid, our case is consistent with type A involvement.5
The diagnosis of BNS remains challenging, with some experts considering a histological biopsy of the cerebrum or meninges as the gold standard, though cerebrospinal fluid flow cytometry remains a key diagnostic tool.6
Conclusion
This case underscores the complexities of WM when accompanied by CM and BNS. CM can serve as a marker of WM activity, while BNS represents a severe neurological complication requiring early detection and specific treatment. The patient’s improvement following tailored therapy highlights the importance of a comprehensive approach in managing these interconnected conditions.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kaseb H.Gonzalez-Mosquera L.F.Parsi M.Lymphoplasmacytic Lymphoma 2024 Stat Pearls 30020728 · pubmed ↗
- 2Gressier L.Hotz C.Lelièvre J.D.Cutaneous macroglobulinosis: a report of 2 cases Arch Dermatol 146220101651692015702710.1001/archdermatol.2009.359 · doi ↗ · pubmed ↗
- 3Nanah A.Al Hadidi S.Bing-Neel syndrome: update on the diagnosis and treatment Clin Lymphoma Myeloma Leuk 2172021 e 643e 64810.1016/j.clml.2021.09.01434674984 · doi ↗ · pubmed ↗
- 4Simon L.Fitsiori A.Lemal R.Bing-Neel syndrome: clinical and imaging findings in 44 cases Haematologica 100122015158715942638521110.3324/haematol.2015.133744 PMC 4666335 · doi ↗ · pubmed ↗
- 5Ly K.I.Fintelmann F.J.Forghani R.Bing-Neel syndrome: a multicenter retrospective study of 36 patients Clin Lymphoma Myeloma Leuk 11220111801852185655510.3816/CLML.2011.n.043 · doi ↗ · pubmed ↗
- 6Minnema M.C.Kimby E.D’Sa S.Diagnosis and treatment of Bing-Neel syndrome: an evidence-based review Haematologica 10212009434810.3324/haematol.2016.147728 PMC 521023127758817 · doi ↗ · pubmed ↗