A linear purpuric rash in an elderly man
Vinh Nguyen, Christopher N. Nguyen, Dario Kivelevitch

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
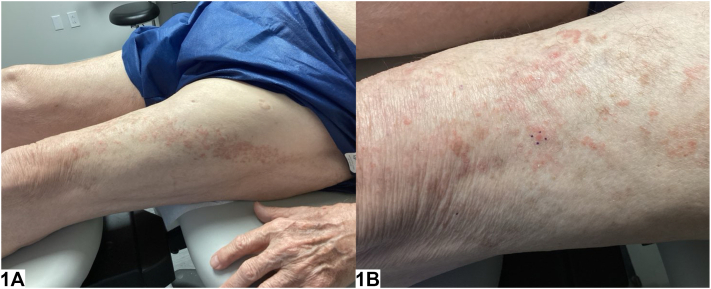 Figure 1
Figure 1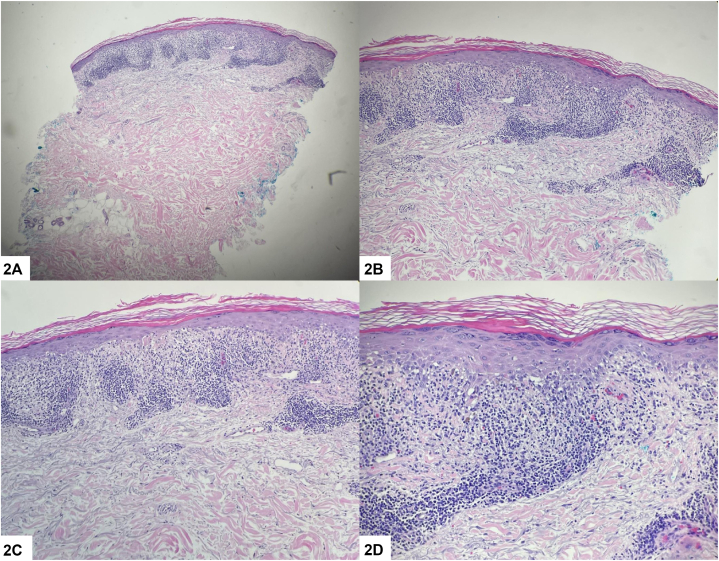 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Cutaneous lymphoproliferative disorders research · Sarcoidosis and Beryllium Toxicity Research
Case presentation
An 88-year-old male presented to the dermatology clinic for evaluation of a rash on his left thigh. This rash had been present for several months and was asymptomatic. His primary care physician diagnosed the rash as atopic dermatitis; however, there was no improvement with emollients or triamcinolone 0.1% cream. He denied a history of herpes zoster and had received the shingles vaccine. On physical exam, there were red-brown papules coalescing into plaques in a linear distribution across his left thigh (Fig 1). A punch biopsy showed band-like lymphocytic infiltrate at the dermal-epidermal junction, along with erythrocyte extravasation and hemosiderin deposition (Fig 2).Fig 1. Fig 2
Question 1: what is the diagnosis?
- A.Linear lichenoid pigmented purpura
- B.Lichen striatus
- C.Linear lichen planus
- D.Linear Darier disease
- E.Linear psoriasis
Answers:
- A.Linear lichenoid pigmented purpura – Correct. Pigmented purpuric dermatosis (PPD) describes a group of chronic skin disorders characterized by distinct red-to-golden brown macules, patches, and papules with petechiae.1^,^2 PPD is generally divided into 55 major variants, with linear pigmented purpura – also known as unilateral linear capillaritis – being a rarer form. It often presents unilaterally on an extremity, sometimes in a blaschkoid distribution such as in our patient.1^,^3^,^4 On histology, lymphocytic inflammation with extravasated erythrocytes in the upper dermis is seen.1^,^4 Our patient’s histology was consistent with a lichenoid pattern, helping further classify the diagnosis as the even more rare linear lichenoid pigmented purpura.4
- B.Lichen striatus – Incorrect. Lichen striatus primarily occurs in children, and skin biopsy shows peri-eccrine lymphocytic inflammation.4
- C.Linear lichen planus – Incorrect. Linear lichen planus presents with significant pruritus, deep purple-colored lesions, and postinflammatory hyperpigmentation.4 In addition, histology shows a lichenoid band of inflammation in the papillary dermis with epidermal hyperplasia and hypergranulosis but without extravasated erythrocytes.4
- D.Linear Darier disease – Incorrect. Segmental Darier disease is typically composed of keratotic, sometimes crusted, papules that are pink to red-brown rather than purpuric. Histopathologic findings include acantholysis and dyskeratosis.
- E.Linear psoriasis – Incorrect. Linear psoriasis typically presents as intensely pruritic, erythematous, and scaly papules and plaques along Blaschko’s lines. Biopsy would not show a lichenoid infiltrate.5
Question 2: which is the most common underlying cause of this condition?
- A.Hepatitis C
- B.Medication-induced
- C.Liver disease
- D.Genetic mosaicism
- E.Idiopathic
Answers:
- A.Hepatitis C – Incorrect. Hepatitis C is associated with the development of lichen planus.
- B.Medication-induced – Incorrect. Although medications are frequently reported as triggers for PPD, the etiology of PPD is unknown.1 Identified medication triggers include acetaminophen, aspirin, chlordiazepoxide, glipizide, and hydralazine.1^,^2^,^4
- C.Liver disease – Incorrect. PPD is rarely associated with systemic disorders such as hyperlipidemia, diabetes mellitus, rheumatoid arthritis, thyroid disease, liver disease, and hematologic or solid neoplasms.2
- D.Genetic mosaicism – Incorrect. Genetic mosaicism is believed to play a role in the pathogenesis of linear psoriasis, although the exact mechanism is not completely understood.5
- E.Idiopathic – Correct. Most cases of PPD are idiopathic. PPD results from minimal inflammation and hemorrhage of vessels of the superficial dermis, most commonly capillaries, in the absence of coagulopathy.2^,^3 Physical activity, prolonged standing, venous hypertension, capillary fragility, and local infections are underlying factors that may lead to the development or worsen preexisting PPD.2
Question 3: what other variants of this entity can also present with lichenoid inflammation on histopathology?
- A.Lichen aureus
- B.Pigmented purpuric lichenoid dermatitis of Gougerot and Blum
- C.Purpura annularis telangiectodes of Majocchi
- D.A & B
- E.A, B, & C
Answers:
- A.Lichen aureus – Incorrect. Although lichen aureus does have a lichenoid infiltrate, this is not the only variant of PPD that may show the lichenoid pattern.2^,^4
- B.Pigmented purpuric lichenoid dermatitis of Gougerot and Blum – Incorrect. Similar to lichen aureus, pigmented purpuric lichenoid dermatitis of Gougerot and Blum may also have a lichenoid infiltrate.2^,^4
- C.Purpura annularis telangiectodes of Majocchi – Incorrect. Purpura annularis telangiectodes of Majocchi does not typically have a lichenoid infiltrate, but rather a perivascular pattern of lymphocytic inflammation, which is similar to Schamberg disease.2
- D.A & B – Correct. Both of those variants exhibit a lichenoid inflammatory pattern.3
- E.A, B, & C – Incorrect. See explanation for answer choice C.3
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sardana K.Sarkar R.Sehgal V.N.Pigmented purpuric dermatoses: an overview Int J Dermatol 437200448248810.1111/j.1365-4632.2004.02213.x 15230884 · doi ↗ · pubmed ↗
- 2Spigariolo C.B.Giacalone S.Nazzaro G.Pigmented purpuric dermatoses: a complete narrative review J Clin Med 10112021228310.3390/jcm 1011228334070260 PMC 8197337 · doi ↗ · pubmed ↗
- 3Kimak A.Zebrowska A.Therapeutic approach in pigmented purpuric dermatoses-A scoping review Int J Mol Sci 2552024264410.3390/ijms 2505264438473891 PMC 10932383 · doi ↗ · pubmed ↗
- 4Momin Z.K.Vandergriff T.W.Nezafati K.Linear lichenoid pigmented purpura: an unusual histopathologic pattern JAAD Case Rep 292022111310.1016/j.jdcr.2022.08.04936186405 PMC 9522877 · doi ↗ · pubmed ↗
- 5Martora F.Fabbrocini G.Picone V.Blasio C.Ruggiero A.Megna M.A case of linear psoriasis in a young patient with Down syndrome and review of the literature J Cosmet Dermatol 222202368668810.1111/jocd.1531735980674 PMC 10087020 · doi ↗ · pubmed ↗