Disseminated abscesses due to Mycobacterium wolinskyi and Mycobacterium mageritense: An unusual mixed infection
Verena Gerlinde Frings, Thiên-Trí Lâm, Christoph Lange, Matthias Goebeler, Johanna Stoevesandt

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
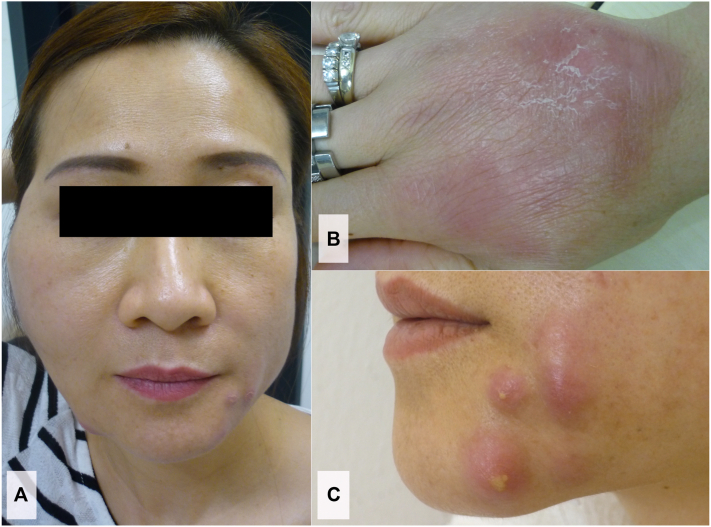 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infectious Diseases and Mycology · Tuberculosis Research and Epidemiology
Introduction
We present a case of disseminated abscesses caused by Mycobacterium wolinskyi and Mycobacterium mageritense in a seemingly immunocompetent individual with no identifiable predisposing factors. Nontuberculous mycobacterial infections represent an infrequent, though possibly underestimated differential diagnosis of cutaneous abscesses unresponsive to standard antibiotic treatment. Genetic defects affecting the interferon-gamma (IFNγ)/interleukin-12 axis and autoantibodies to IFNγ have been described as predisposing factors for active clinical infections with weakly virulent mycobacteria in apparently immunocompetent hosts.1^,^2 The genetically closely related species M. wolinskyi and M. mageritense have been recognized as an occasional cause of surgical site infections.3, 4, 5
Case report
A 46-year-old woman of Asian origin presented to our department with a 2-week history of painful cutaneous nodules accompanied by fever up to 39 °C. Lesions had initially appeared on the chin, subsequently spread to the cheeks and back of the hands, and were unresponsive to intravenous antibiotic treatment with cefuroxime. She declared to be otherwise healthy, denied an increased susceptibility to infections in the past and was not on any medication. She denied any preceding surgical, dental, or cosmetic interventions, or acupuncture. About 1 week prior to the onset of symptoms, she had cleaned her husband’s aquarium without wearing gloves. No other family members were affected.
Clinical examination on admission showed numerous erythematous cutaneous nodules of 1-5 centimeters in diameter (Fig 1) and a painless enlargement of the cervical lymph nodes. Mouth opening was limited due to extensive swelling of the right cheek. Laboratory tests revealed a pronounced leukocytosis (19,300 cells/μL), and a moderately elevated C-reactive protein (3.6 mg/dL; reference value < 0.5 mg/dl). Blood cultures were negative. Serological examination for human immunodeficiency virus was negative. Microscopic examination of pus revealed partially stained gram-positive rods, which proved acid-fast upon Ziehl-Neelsen staining. Nucleic acid amplification tests for M. tuberculosis-specific 16S rRNA were negative; and no M. tuberculosis-reactive T lymphocytes were detected in the Interferon Gamma Release Assay. Cultures from pus aspirates on Columbia Blood Agar and modified Middlebrook 7H9 Broth in a Mycobacteria Growth Indicator Tube system revealed bacterial growth within 5 days. 16S rRNA polymerase chain reaction and subsequent analysis of the 800 base pairs amplification product showed sequences of 2 different Mycobacterium spp. Alignment of both sequences confirmed a mixed infection with M. wolinskyi and M. mageritense. Growth of M. fortuitum was detected in samples of aquarium water but considered unrelated to the patient’s infection. Abnormalities in the IFN-γ/signal transducer and activator of transcription protein 1 signaling pathway could be excluded, as signal transducer and activator of transcription protein 1 phosphorylation was not impaired after stimulation of patient monocytes with lipopolysaccharide and IFN-γ. IFN-γ production after stimulation with Concanavalin A was within normal range.Fig 1. Cutaneous abscesses due to a mixed infection with M. wolinskyi and M. mageritense. Extensive subcutaneous swelling with palpable fluctuation of the right cheek (A). Erythematous nodules of 1-5 centimeters in diameter on the dorsum of the right hand (B), and over the mandibula (C).
All abscesses were incised, rinsed and drained. A quadruple therapy comprising intravenous amikacin (1 g/d), oral linezolid (600 mg/d), oral doxycycline (200 mg/d), and oral moxifloxacin (400 mg/d) led to complete clearance of cutaneous lesions within 12 weeks. Subsequent oral triple therapy with linezolid, doxycycline, and moxifloxacin was carried out for another 3 months. 8 months after completing treatment, she was confirmed to be in continued remission.
Discussion
Both M. wolinskyi and M. mageritense are nontuberculous rapidly growing mycobacteria (RGM). Both species have a worldwide distribution and can be found in natural and treated water, sewage, and dirt.6 Pathogenic RGM species primarily belong to the M. fortuitum group, the M. chelonae/abscessus group, or the M. smegmatis group.6 M. wolinskyi has been described as a distinct species within the M. smegmatis group in 1999.7 M. mageritense was defined as a new species in 1997. Due to its phenotype and biochemical properties (ability to utilize mannitol, inositol, and sorbitol) it was originally considered a member of the M. fortuitum third biovariant complex. Genetically it is, however, more closely aligned to the M. smegmatis group, and its 16S rRNA sequence differs by only 9 base pairs from that of M. wolinskyi.3^,^6
Infections with M. wolinskyi and M. mageritense have been observed in both overtly immunosuppressed and seemingly immunocompetent hosts.5 The hereditary predisposition to infections caused by weakly virulent mycobacteria in otherwise healthy individuals has been referred to as ‘Mendelian susceptibility to mycobacterial disease’. Several Mendelian susceptibility to mycobacterial disease-related genes, most of which are involved in the IFNγ-/interleukin-12 axis, have to date been identified. Identifiable genetic defects, however, account for only half of the known Mendelian susceptibility to mycobacterial disease cases.1^,^2 Autoantibodies to IFNγ have likewise been identified as a predisposing factor for nontuberculous mycobacterial infections. They are more prevalent in Asian populations,8 but have been ruled out in our present case. Given the exceedingly low prevalence of M. wolinskyi/M. mageritense-related diseases, we strongly suspect that some kind of either genetically defined or acquired immunodeficiency is a prerequisite for active clinical infection, even in patients lacking any previous indication of overt immunosuppression.
M. wolinskyi and M. mageritense are mainly associated with cutaneous infections, osteomyelitis, and bacteremia. Infections are usually preceded by surgery or penetrating trauma, and occasionally by cosmetic procedures.3, 4, 5 Our case of a spontaneous infection without a history of a preceding trauma represents an exception to this pattern. While it is the hitherto first description of a simultaneous infection with M. wolinskyi and M. mageritense, mixed infections of other nontuberculous Mycobacteria species are not uncommon and have been associated with environmental exposure.9 No environmental source, however, could be identified in the present case.
While RGM are commonly resistant to standard antituberculosis agents, no standardized treatment recommendations have to date been established. Though macrolides (eg clarithromycin) are considered appropriate to treat other nontuberculous mycobacterial infections, several RGM species including M. mageritense and M. wolinskyi are naturally resistant.3 Intrinsic macrolide resistance has been demonstrated to be conferred by the rRNA methylase erm(40) gene.10 Both M. wolinskyi and M. mageritense are commonly susceptible to amikacin, quinolones, and linezolid.3 Administration of at least 2 active antimicrobial agents is advocated.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bustamante J.Boisson-Dupuis S.Abel L.Casanova G.L.Mendelian susceptibility to mycobacterial disease: genetic, immunological, and clinical features of inborn errors of IFN-γ immunity Semin Immunol 2620144544702545322510.1016/j.smim.2014.09.008PMC 4357480 · doi ↗ · pubmed ↗
- 2Khavandegar A.Mahdaviani S.A.Zaki-Dizaji M.Genetic, immunologic, and clinical features of 830 patients with Mendelian susceptibility to mycobacterial diseases (MSMD): A systematic review J Allergy Clin Immunol 1532024143214443834118110.1016/j.jaci.2024.01.021PMC 11880893 · doi ↗ · pubmed ↗
- 3Wallace R.J.Jr.Brown-Elliott B.A.Hall L.Clinical and laboratory features of Mycobacterium mageritense J Clin Microbiol 402002293029351214935410.1128/JCM.40.8.2930-2935.2002 PMC 120677 · doi ↗ · pubmed ↗
- 4Yoo S.J.Lee K.H.Jung S.N.Heo S.T.Facial skin and soft tissue infection caused by Mycobacterium wolinskyi associated with cosmetic procedures BMC Infect Dis 1320134792413152210.1186/1471-2334-13-479PMC 3852821 · doi ↗ · pubmed ↗
- 5Dupont C.Terru D.Aguilhon S.Source-case investigation of Mycobacterium wolinskyi cardiac surgical site infection J Hosp Infect 9320162352392721027110.1016/j.jhin.2016.03.024 · doi ↗ · pubmed ↗
- 6Brown-Elliott B.A.Philley J.V.Rapidly growing mycobacteria Microbiol Spectr 5201710.1128/microbiolspec.tnmi 7-0027-2016 PMC 1168746028084211 · doi ↗ · pubmed ↗
- 7Brown B.A.Springer B.Steingrube V.A.Description of Mycobacterium wolinskyi and Mycobacterium goodii, two new rapidly growing species related to Mycobacterium smegmatis and associated with human wound infections: a cooperative study from the international working group on mycobacterial taxonomy Int J Syst Bacteriol 491999149315111055533010.1099/00207713-49-4-1493 · doi ↗ · pubmed ↗
- 8Browne S.K.Burbelo P.D.Chetchotisakd P.Adult-onset immunodeficiency in Thailand and Taiwan N Engl J Med 36720127257342291368210.1056/NEJ Moa 1111160 PMC 4190026 · doi ↗ · pubmed ↗