Combined endoscopic approach with fluoroscopy-guided radial incision and cutting for a complete esophageal stricture
Akito Furuta, Shunsuke Omoto, Shunsuke Ogata, Hironori Tanaka, Mamoru Takenaka, Taro Inoue, Wataru Ono

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
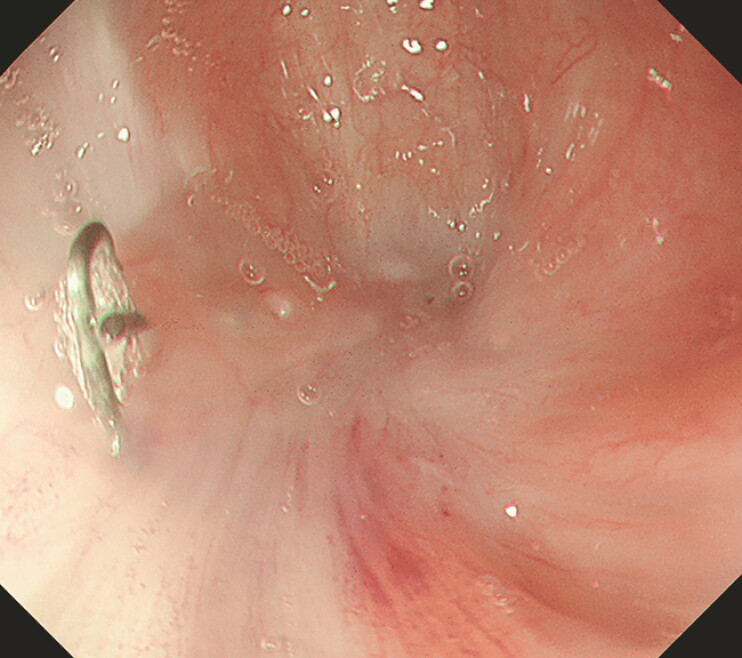 Fig. 1
Fig. 1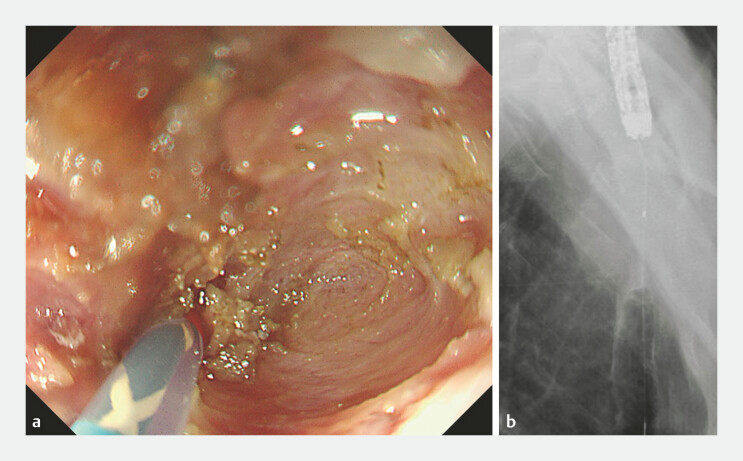 Fig. 2
Fig. 2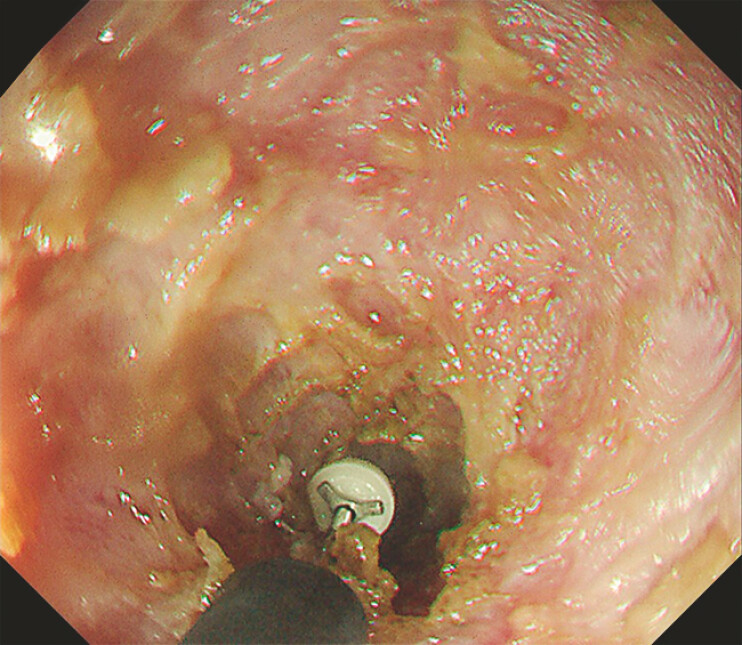 Fig. 3
Fig. 3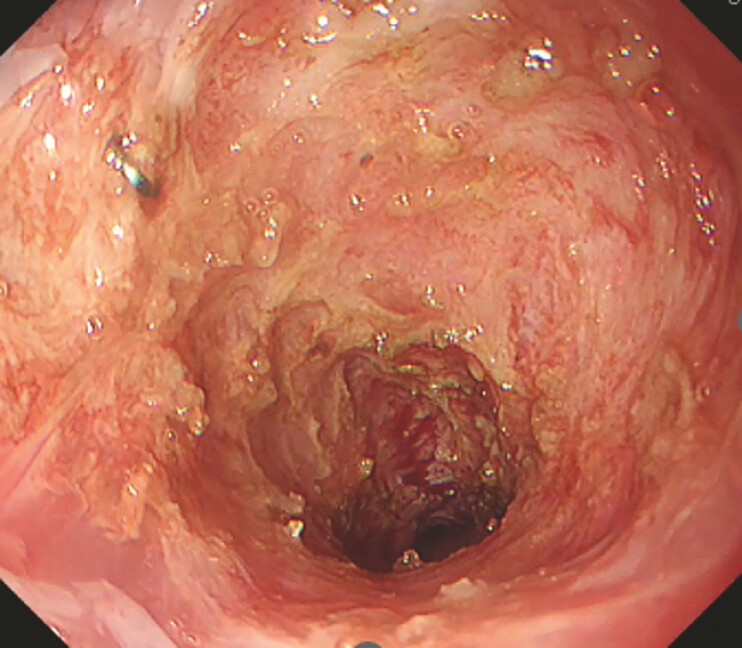 Fig. 4
Fig. 4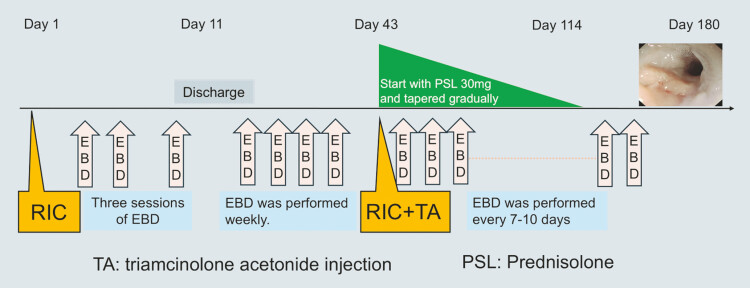 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Tracheal and airway disorders · Dysphagia Assessment and Management
The treatment options for benign esophageal strictures include endoscopic balloon dilation (EBD), bougie dilation, and radial incision and cutting (RIC) 1 2 . RIC has been proposed for refractory cases 3 . While stricture recurrence after RIC has been reported, a multimodal approach combining RIC, EBD, and steroid therapy is suggested as a safe and effective strategy 4 5 .
This video shows a case of a complete esophageal stricture successfully treated with RIC and EBD under fluoroscopic guidance ( Video 1 ).
Complete esophageal stricture successfully managed using a combined endoscopic approach with fluoroscopy-guided radial incision and cutting, along with balloon dilation.Video 1
A 74-year-old man underwent a thoracoscopic esophagectomy for advanced esophageal cancer. On postoperative day (POD) 4, anastomotic leakage occurred and was managed with a fully covered esophageal stent. On POD 46, dysphagia developed due to stent migration, necessitating removal of the stent. Oral intake became impossible and repeated EBD was followed by a poor response. RIC was initiated on POD 86.
On the day of RIC, the stricture had progressed to the extent that the lumen was unidentifiable, and it was assessed as complete stricture ( Fig. 1 ). An initial incision with a flush knife BT-S 2.0 (Fujifilm Medical, Tokyo, Japan) was attempted, but due to the risk of perforation, fluoroscopic guidance was employed. A guidewire and catheter were advanced beyond the stricture to facilitate a safer incision ( Fig. 2 ). Incision and bougienage were alternated, followed by an arc-like IT knife (Olympus, Tokyo, Japan) incision to remove the scar tissue ( Fig. 3 ). The stricture was then dilated with a balloon, allowing the passage of an endoscope ( Fig. 4 ).
On the day when radial incision and cutting (RIC) was carried out, the stricture had progressed to the extent that the lumen was unidentifiable, and it was assessed as complete stricture.
a, b Under fluoroscopic guidance, a guidewire and catheter were advanced beyond the stricture to facilitate a safer incision.
After advancing the incision to a certain extent, a switch was made to an IT knife and the scar tissue was removed in an arc-like manner.
The stricture was successfully dilated, allowing the passage of an endoscope.
The patient underwent repeated EBD and an additional RIC followed by an injection of 40 mg triamcinolone acetonide. Oral prednisolone therapy was subsequently initiated at a dose of 30 mg per day. Six months after the initial RIC, he was able to consume almost all solid foods without difficulty or stricture recurrence ( Fig. 5 ).
The patient underwent repeated endoscopic balloon dilation and an additional RIC, followed by steroid therapy. Six months after the initial RIC, he showed significant improvement, being able to consume almost all solid foods without difficulty and without stricture recurrence.
This case demonstrates that a comprehensive multimodal approach combining fluoroscopy-guided RIC, EBD, and steroid therapy can provide a safe and effective treatment strategy for complete esophageal strictures.
Endoscopy_UCTN_Code_TTT_1AO_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yoda Y Yano T Kaneko K Endoscopic balloon dilatation for benign fibrotic strictures after curative nonsurgical treatment for esophageal cancer Surg Endosc 2012262877288310.1007/s 00464-012-2273-922543993 · doi ↗ · pubmed ↗
- 2Kano Y Kadota T Inaba A Efficacy and safety of repeated endoscopic radial incision and cutting procedure for benign esophageal stricture Endosc Int Open 202311 E 230E 23610.1055/a-2005-767836910847 PMC 9995178 · doi ↗ · pubmed ↗
- 3Mitani Y Hirohashi K Tamaoki M Efficacy and safety of radial incision and cutting for nonsurgical refractory benign esophageal stricture Endosc Int Open 202412 E 1035 E 104210.1055/a-2382-621339263558 PMC 11387040 · doi ↗ · pubmed ↗
- 4Muto M Ezoe Y Yano T Usefulness of endoscopic radial incision and cutting method for refractory esophagogastric anastomotic stricture (with video)Gastrointest Endosc 20127596597222520877 10.1016/j.gie.2012.01.012 · doi ↗ · pubmed ↗
- 5Ikeda T Matsui H Combined endoscopic techniques for esophageal pinhole-like stenosis after photodynamic therapy JJSLSM 20234413614210.2530/jslsm.jslsm-44_0023 · doi ↗