Endoscopic ultrasonography-guided hepaticogastrostomy with a novel 0.018-inch guidewire and a slim-delivery metallic stent
Shotaro Tsunoda, Haruo Miwa, Hiromi Tsuchiya, Kazuki Endo, Ritsuko Oishi, Yuichi Suzuki, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
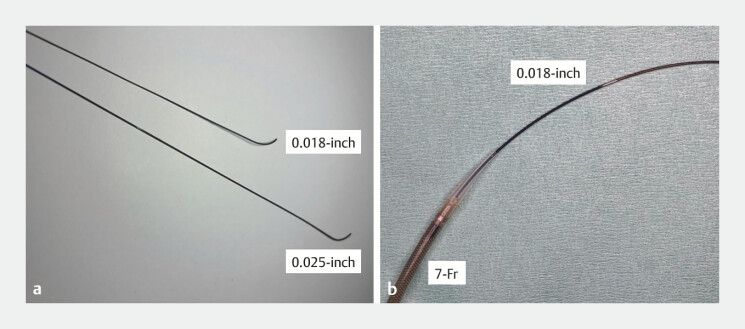 Fig. 1
Fig. 1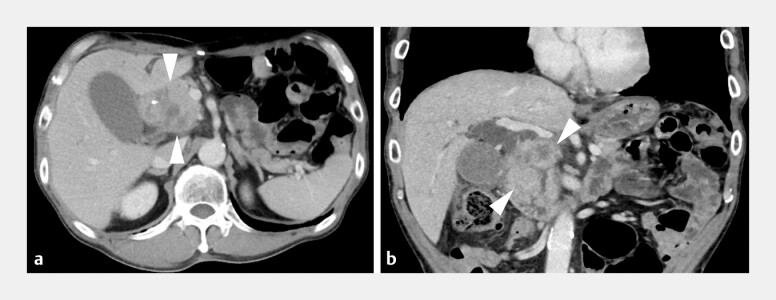 Fig. 2
Fig. 2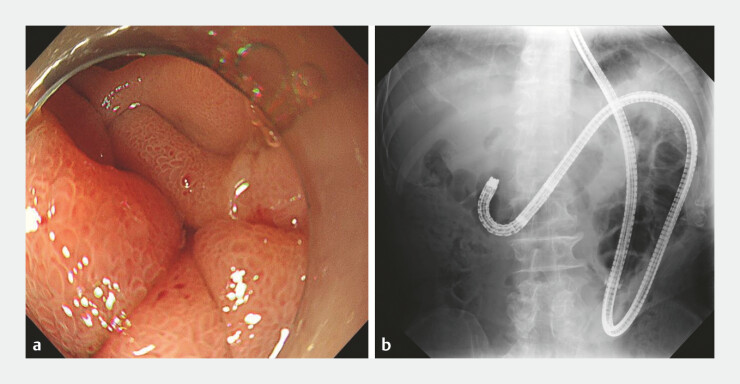 Fig. 3
Fig. 3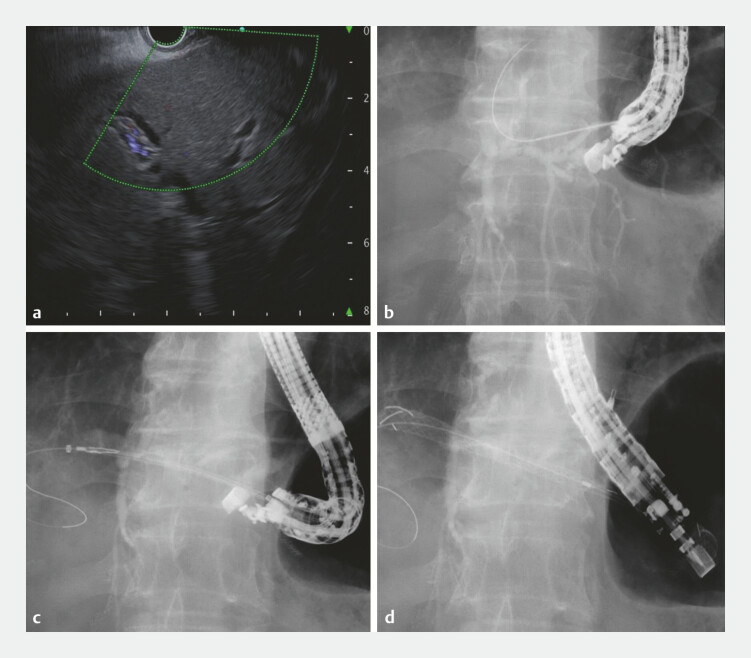 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Pediatric Hepatobiliary Diseases and Treatments
The utility of 22-gauge needle for endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS) has been reported; however, a dedicated guidewire has not been developed 1 2 3 4 5 . Recently, a novel 0.018-inch guidewire (J-wire NM; J-MIT) without markers was developed to prevent guidewire stacking and a stiff shaft for smooth stent delivery. Additionally, a 7-Fr slim-delivery metallic stent (Niti-S EUS-BD system End Bare Single Flare; Taewoong Medical Co., Ltd.) has an ultra-tapered tip designed to minimize the gap with a 0.018-inch guidewire ( Fig. 1 ). Herein, we report a case in which EUS-HGS was successfully performed using a novel 0.018-inch guidewire and slim-delivery metallic stent ( Video 1 ).
a A novel 0.018-inch guidewire (J-wire NM; J-MIT) without markers was developed for endoscopic ultrasound-guided hepaticogastrostomy to prevent guidewire stacking at the needle tip. b Novel self-expandable metallic stent with a 7-Fr slim-delivery system (Niti-S EUS-BD system End Bare Single Flare; Taewoong Medical Co., Ltd.) features an ultra-tapered tip that minimizes the gap with a 0.018-inch guidewire.
A novel 0.018-inch guidewire without markers and a 7-Fr slim-delivery metallic stent were useful for endoscopic ultrasonography-guided hepaticogastrostomy.Video 1
A 64-year-old man who had previously undergone distal gastrectomy with Roux-en Y reconstruction for advanced gastric cancer was admitted to our hospital due to obstructive jaundice caused by a recurrent tumor ( Fig. 2 ). As balloon enteroscopy could not reach the papilla of Vater due to tumor infiltration ( Fig. 3 ), EUS-HGS was attempted. The slightly dilated B3 was punctured using a 22-gauge needle (Expect Slim-line; Boston Scientific Co.) ( Fig. 4 ). After the cholangiography, the novel 0.018-inch guidewire migrated outside of the bile duct; however, it was safely removed without guidewire stacking. After re-puncture, the guidewire was successfully inserted into the bile duct. Subsequently, tract dilation was performed using a 7-Fr bougie dilator dedicated to a 0.018-inch guidewire (ES Dilator Soft; Zeon Medical, Inc.). To minimize the risk of bile leakage, the novel metallic stent (8-mm, 12-cm) with a 7-Fr slim delivery system was inserted without guidewire exchange. The metallic stent was successfully placed from the bile duct to the stomach. The patient was discharged without adverse events following the improvement of jaundice.
Computed tomography images show huge lymph node metastases (arrowheads) that obstruct the common bile duct and the duodenum. a Axis plane. b Coronal plane.
Balloon enteroscopy reveals tumor infiltration at the duodenum that prevent to reach the papilla of Vater. a Endoscopic image. b Fluoroscopic image.
Endoscopic ultrasonography-guided hepatogastrostomy. a The slightly dilated bile duct is shown at segment 3. b Although the novel 0.018-inch guidewire migrates outside the bile duct, it can be removed without guidewire stacking. c After the guidewire insertion into the bile duct, a 7-Fr slim delivery of a novel metallic stent (Niti-S EUS-BD system End Bare Single Flare; Taewoong Medical Co., Ltd.) is inserted along the guidewire. d The metallic stent is successfully placed from the bile duct to the stomach.
To the best of our knowledge, this is the first report of EUS-HGS using a novel 0.018-inch guidewire and an ultra-tapered, slim-delivery metallic stent.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isayama H Nakai Y Itoi T Clinical practice guidelines for safe performance of endoscopic ultrasound/ultrasonography-guided biliary drainage: 2018 J Hepatobiliary Pancreat Sci 20191624926910.1002/jhbp.631PMC 706489431025816 · doi ↗ · pubmed ↗
- 2Kanno Y Ito K Sakai T Novel combination of a 0.018-inch guidewire, dedicated thin dilator, and 22-gauge needle for EUS-guided hepaticogastrostomy Video GIE 2020535535810.1016/j.vgie.2020.04.00332817927 PMC 7426615 · doi ↗ · pubmed ↗
- 3Ogura T Ueno A Okuda A Expanding indications for endoscopic ultrasound-guided hepaticogastrostomy for patients with insufficient dilatation of the intrahepatic bile duct using a 22G needle combined with a novel 0.018-inch guidewire (with video)Dig Endosc 20223422222734351029 10.1111/den.14101 · doi ↗ · pubmed ↗
- 4Ogura T Opening a new window of interventional endoscopic ultrasound using a 22-G needle with dedicated dilation device Endoscopy 20245601 E 1104 E 110510.1055/a-2489-833439657929 PMC 11631545 · doi ↗ · pubmed ↗
- 5Hara K Okuno N Haba S How to perform EUS-guided hepaticogastrostomy easier and safer J Hepatobiliary Pancreat Sci 20202756356410.1002/jhbp.77432511837 · doi ↗ · pubmed ↗