The endoscopist’s third hand: external floss traction-assisted duodenal papillary intubation for hidden papilla
Yan Zhang, Shanbin Wu, Yuping Zhang, Qing Yan, Guoliang Zhao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
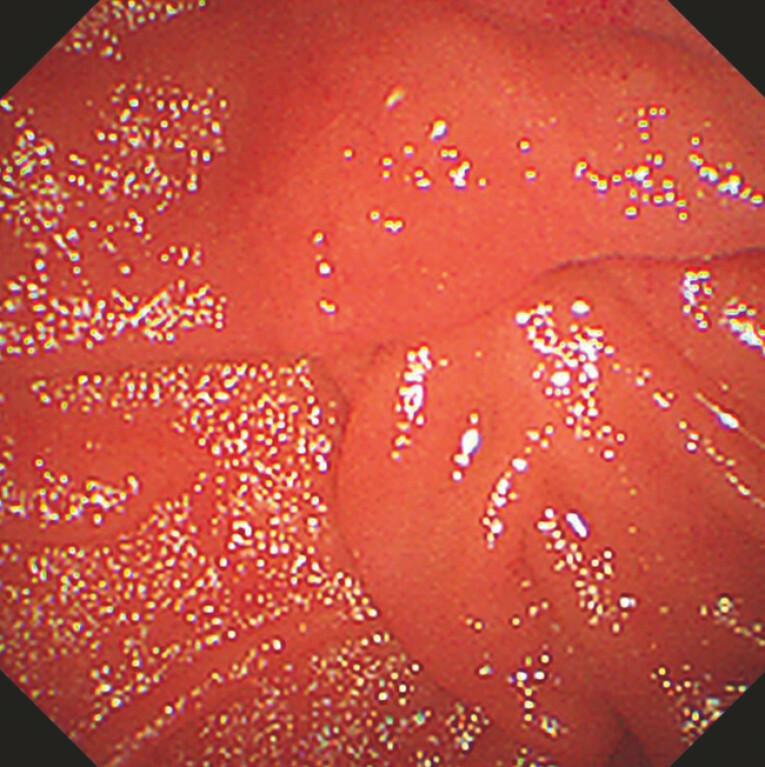 Fig. 1
Fig. 1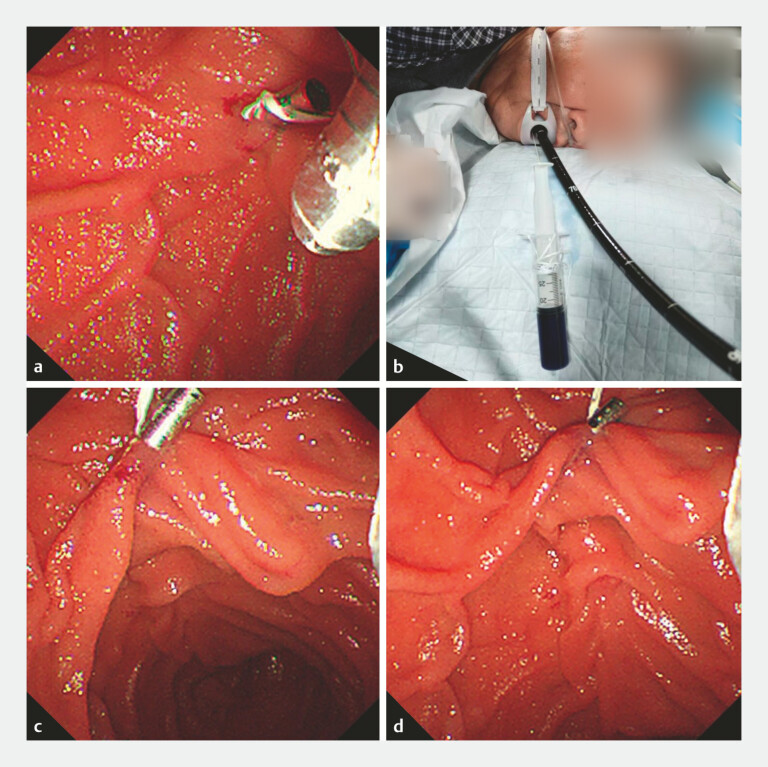 Fig. 2
Fig. 2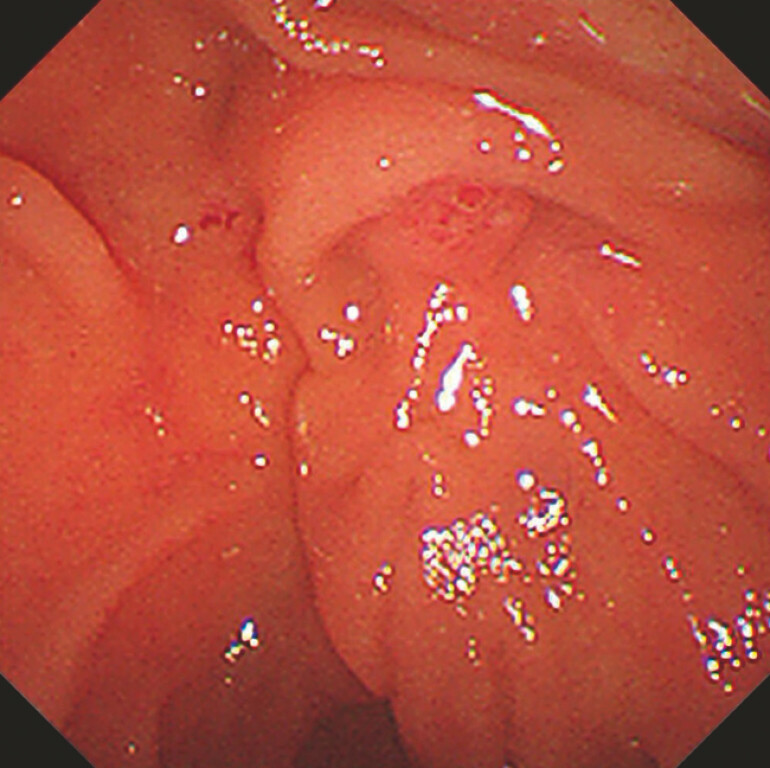 Fig. 3
Fig. 3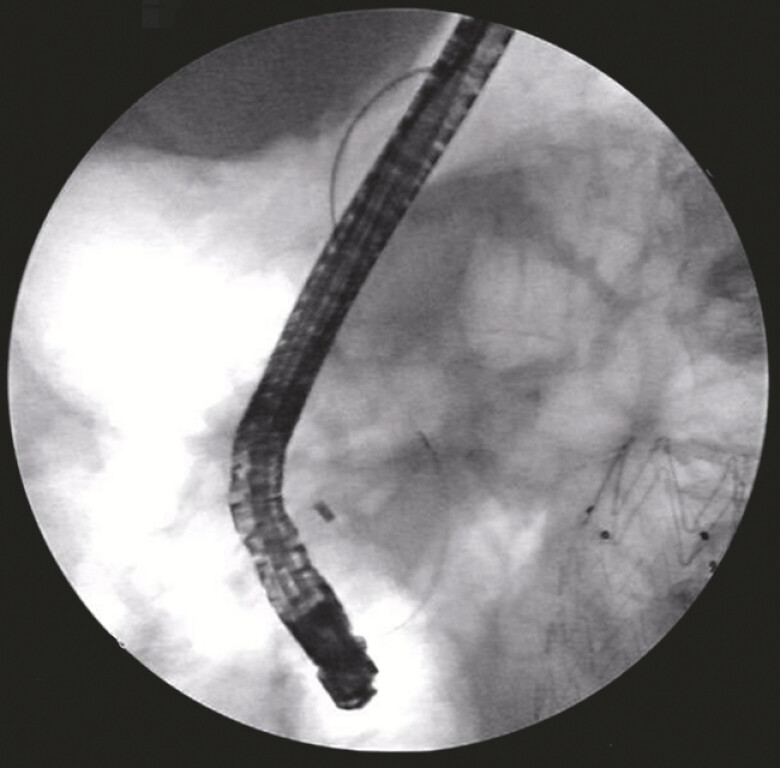 Fig. 4
Fig. 4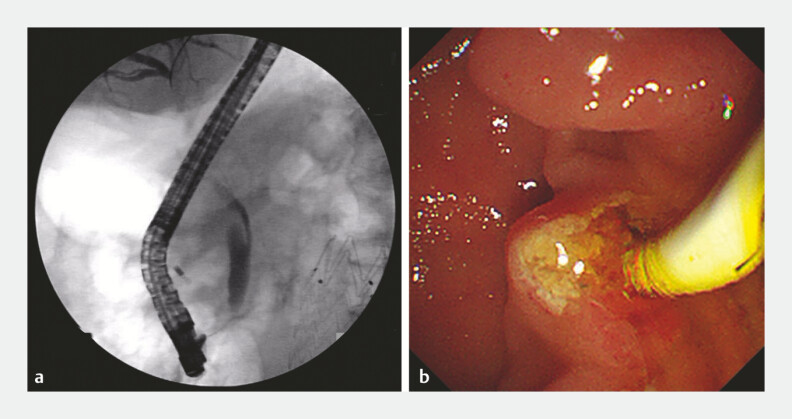 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Esophageal and GI Pathology
Difficult biliary or pancreatic cannulation during endoscopic retrograde cholangiopancreatography (ERCP) is among the leading causes of failed operations 1 . The adequate exposure of the ampullary orifice and reliable fixation of the duodenal papilla are always the basic principles of successful cannulation during ERCP 2 . Inspired by the application of traction in endoscopic treatment of early gastrointestinal tumors, we have developed external floss traction to accomplish difficult cannulation during ERCP.
A 70-year-old man was referred for ERCP for suspected common bile duct stones. After insertion of a therapeutic duodenoscope, redundant duodenal folds became visible in the descending duodenum, initially giving rise to a “hidden papilla” situation. We developed the external floss traction-assisted duodenal papillary intubation method to effectively accomplish successful biliary cannulation and stone extraction ( Video 1 ).
External floss traction-assisted duodenal papillary intubation for hidden papilla.Video 1
Attempts were made to access the biliary tree using the guidewire-aided cannulation technique; however, as the ampulla of Vater was hidden under duodenal folds, attempts to gain access were unsuccessful ( Fig. 1 ). Subsequently, the external floss traction method was applied to pull the duodenal folds ( Fig. 2 ), and the ampullary orifice became visible ( Fig. 3 ). Successful cannulation of the bile duct was finally achieved ( Fig. 4 ), and bile duct sand-like stones were successfully removed ( Fig. 5 ). Then, a nasobiliary drainage tube was placed smoothly into the bile duct, with fluent drainage of bile juice.
Redundant duodenal folds became visible in the descending duodenum, initially giving rise to a “hidden papilla” situation.
The external floss traction method. a The floss was fixed to the clip, and the clip was applied to the duodenal fold. b The floss was secured externally and was pulled to apply traction. c, d After external floss traction, the ampullary orifice became visible.
The visible ampullary orifice.
Successful cannulation of the bile duct was finally achieved.
Successful removal of bile duct stones. a Cholangiography showed no significant filling defect. b A small number of sand-like stones were removed by the lithotomy balloon.
In this patient, the technique of external floss traction was employed to optimize the view of the papilla, and led to successful biliary cannulation in a short time. As the external floss traction method does not interfere with ERCP instruments and is inexpensive, easily accessible, and simple and convenient to manipulate, it may be applied to routine biliary cannulation in any patient where a traction technique is required.
Endoscopy_UCTN_Code_TTT_1AR
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Kapral C Aabakken LERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20205212714910.1055/a-1075-408031863440 · doi ↗ · pubmed ↗
- 2Takenaka M Arisaka Y Sakai AA novel biliary cannulation method for difficult cannulation cases using a unique, uneven, double-lumen cannula (uneven method)Endoscopy 201850 E 229E 23010.1055/a-0624-931729895066 · doi ↗ · pubmed ↗