A case of annular pancreas complicated with pancreatic ductal adenocarcinoma diagnosed with linear endoscopic ultrasound
Songming Ding, Hengkai Zhu, Xuliang Chen, Shanjie Dong, Qiyong Li, Hua Guo

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
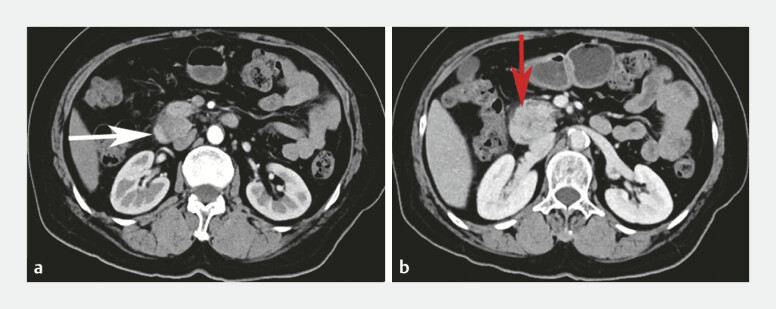 Fig. 1
Fig. 1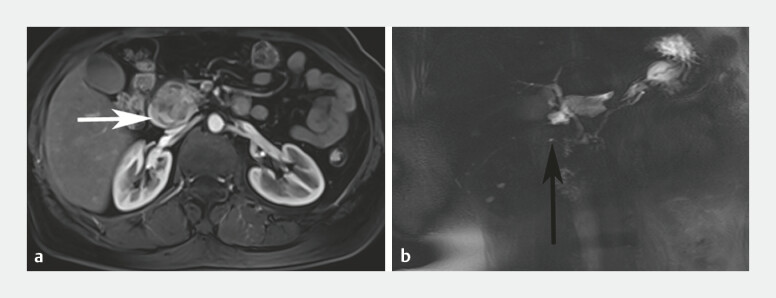 Fig. 2
Fig. 2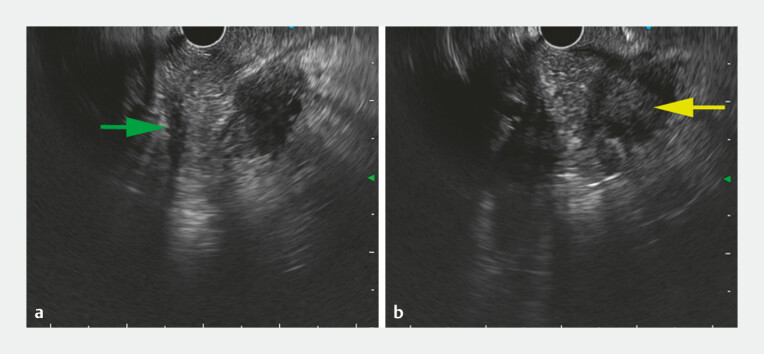 Fig. 3
Fig. 3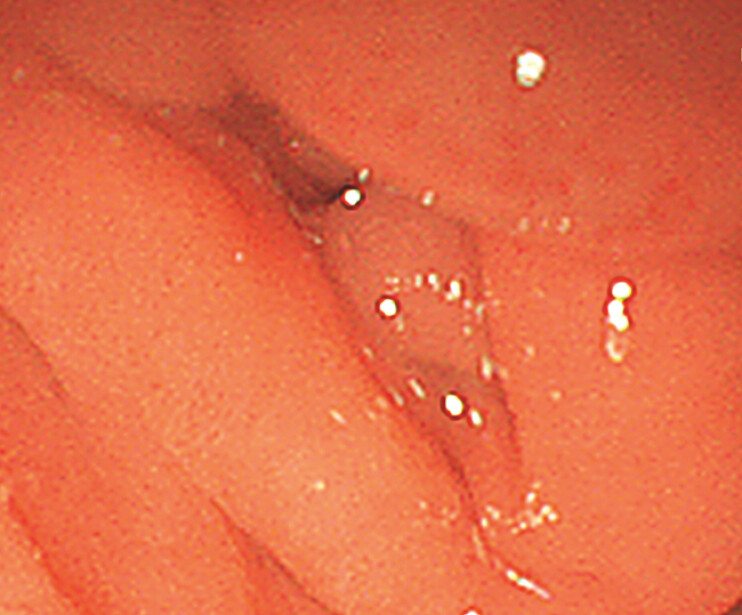 Fig. 4
Fig. 4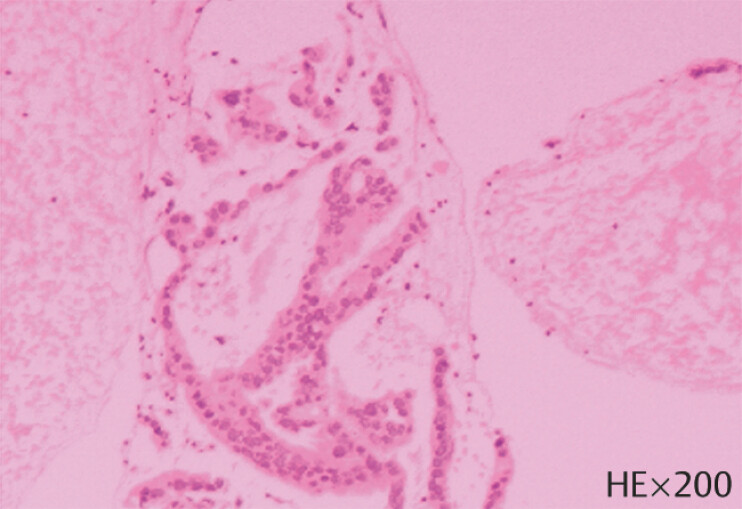 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Pancreatitis Pathology and Treatment · Intestinal Malrotation and Obstruction Disorders
Annular pancreas (AP) is an uncommon congenital anomaly characterized by pancreatic tissue partially or completely encircling the duodenum 1 . AP complicated with pancreatic ductal adenocarcinoma (PDAC) is extremely rare to be reported 2 3 . The diagnosis of AP can be confirmed by endoscopic ultrasound (EUS) 4 5 . Here, we present a patient diagnosed with AP accompanied by PDAC through linear EUS and EUS-guided fine-needle biopsy (EUS-FNB).
The patient was a 78-year-old woman suffering from abdominal distension and anorexia, which had lasted for 2 months. In the last 1 week, the above-mentioned malaise was intensified, and abdominal pain occurred occasionally. Thus, she was admitted to our hospital in order to seek clinical evaluation and treatment in March 2023.
On admission, physical examination revealed no anemia and yellowish discoloration of skin and sclera. Carbohydrate antigen 19-9 (CA19-9) was elevated to 477.5 U/ml (≤43 U/ml). Contrast-enhanced computed tomography (CT) suggested a ring of pancreas surrounding the duodenum and a space-occupying lesion in the pancreatic head ( Fig. 1 ). Contrast-enhanced magnetic resonance imaging (MRI) indicated the existence of AP, but it was not sure whether it was combined with focal pancreatitis or pancreatic cancer ( Fig. 2 ). Linear EUS showed that the pancreas extended to the outer side of the duodenum ( Fig. 3 a ). Meanwhile, the pancreatic duct was observed coursing around the duodenum ( Video 1 ). AP was confirmed. Furthermore, linear EUS showed a hypoechoic mass in the intersection of AP and pancreatic head, measuring 24 × 21 mm, which resulted in significant dilation of the accessory pancreatic duct ( Fig. 3 b ). Noteworthily, the descending part of the duodenum had a narrowed lumen and the endoscopy could not pass through ( Fig. 4 ). Using a 22-gauge needle, we punctured the hypoechoic mass at the duodenal bulb. Histopathology showed poorly differentiated PDAC ( Fig. 5 ).
Contrast-enhanced abdominal CT scan. a A ring of pancreas was seen around the second part of the duodenum (white arrow). b A hypodense mass was indicated (red arrow). Abbreviation: CT, computed tomography.
Contrast-enhanced abdominal MRI. a MRI showed a ring of pancreas surrounding the descending part of the duodenum (white arrow). b MRI depicted the course of the annular pancreatic duct (black arrow). Abbreviation: MRI, magnetic resonance imaging.
Linear EUS view at the duodenal bulb. a Pancreatic parenchyma extension to the outer side of the duodenum with the hypoechoic pancreatic duct coursing around the duodenum (green arrow). b EUS represented a hypoechoic lesion in the intersection of the annular pancreas (AP) and pancreatic head (yellow arrow). Abbreviation: EUS, endoscopic ultrasound.
Linear endoscopic ultrasound (EUS) scanning and EUS-guided fine-needle biopsy (EUS-FNB).Video 1
The endoscopy showed the narrowing of the second part of the duodenum.
A pathological examination of the EUS-FNB showed the poorly differentiated adenocarcinoma. Abbreviation: EUS-FNB, endoscopic ultrasound-guided fine-needle biopsy.
In conclusion, EUS is effective for the definitive diagnosis of AP. If CA19-9 is elevated in AP patients, the possibility of coexisting PDAC should be considered.
Endoscopy_UCTN_Code_CCL_1AZ_2AL
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Benassai G Perrotta S Furino E Ductal adenocarcinoma in anular pancreas Int J Surg 20152101 S 95S 9710.1016/j.ijsu.2015.04.08626118607 · doi ↗ · pubmed ↗
- 2Kawaida H Kono H Watanabe M Pancreaticoduodenectomy for pancreas carcinoma occurring in the annular pancreas: report of a case Clin J Gastroenterol 2015822322710.1007/s 12328-015-0579-626153253 PMC 4548008 · doi ↗ · pubmed ↗
- 3Hayasaki A Kuriyama N Usui MA Case of Robot-Assisted Pylorus-Preserving Pancreatoduodenectomy for Branch-Duct Intraductal Papillary Mucinous Neoplasms Complicated With an Annular Pancreas Asian J Endosc Surg 202518 e 7002210.1111/ases.70022 PMC 1172537239799733 · doi ↗ · pubmed ↗
- 4Kandpal H Bhatia V Garg P Annular pancreas in an adult patient: diagnosis with endoscopic ultrasonography and magnetic resonance cholangiopancreatography Singapore Med J 200950 e 29e 3119224066 · pubmed ↗
- 5Chatterjee A Rana SS Endoscopic Ultrasound in Pancreatic Duct Anomalies Diagnostics (Basel)202313312910.3390/diagnostics 1319312937835872 PMC 10572994 · doi ↗ · pubmed ↗