Reverse sphincterotomy assisted accessory pancreatic duct cannulation
Fan Fan, Jin-Hui Yi, Qian Tong, Liang-Hao Hu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
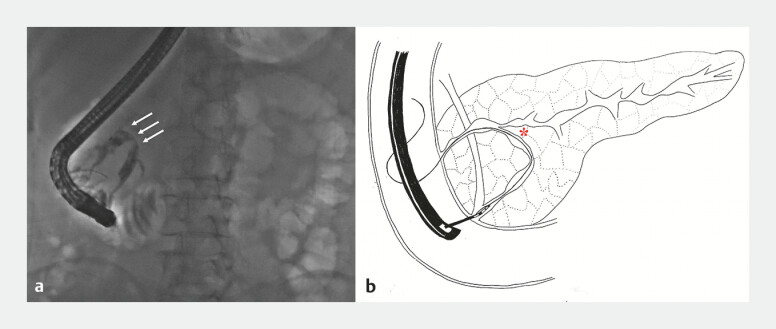 Fig. 1
Fig. 1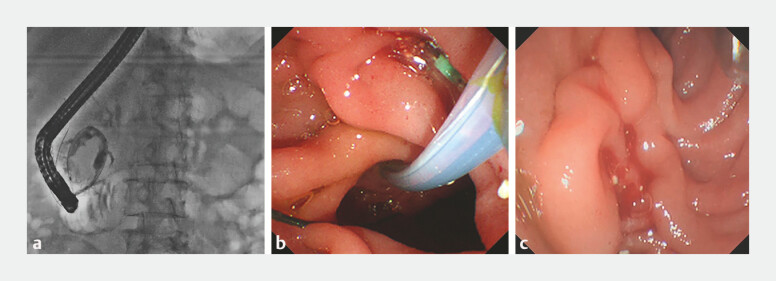 Fig. 2
Fig. 2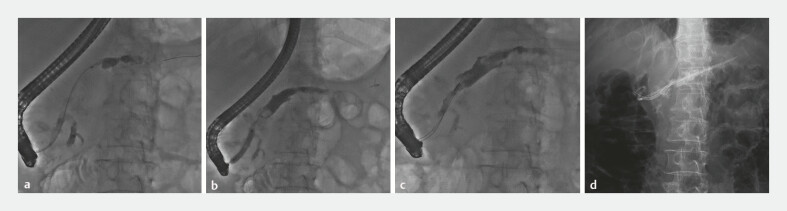 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPediatric Hepatobiliary Diseases and Treatments · Pancreatitis Pathology and Treatment · Gastrointestinal disorders and treatments
A 61-year-old woman admitted to our hospital with pancreatic duct stones. She underwent extracorporeal shockwave lithotripsy followed by endoscopic retrograde cholangiopancreatography (ERCP). Pancreatography demonstrated significant tortuosity of the main pancreatic duct (MPD) ( Fig. 1 a ) and acute angle between the ventral and proximal pancreatic duct which created technical difficulty in advancing the guidewire into the proximal pancreatic duct ( Fig. 1 b ). In this context, we attempted cannulation via minor papilla. However, the inconspicuous orifice of the minor papilla rendered cannulation challenging.
*a Pancreatography demonstrated significant tortuosity of the main pancreatic duct (marked by the white arrows). b A schematic diagram demonstrating the acute angle between the ventral and proximal pancreatic duct (marked by the ) and showing of passage of the guidewire through the main pancreatic duct into the accessory pancreatic duct and subsequent retrograde passage through the minor papilla.
Ultimately, we advanced the guidewire retrogradely through the MPD into the accessory pancreatic duct (APD) and finally into the duodenal lumen via the minor papilla ( Fig. 2 a ). A sphincterotome was then passed retrogradely through a minor papilla along the guidewire. Reverse sphincterotomy was performed with the orientation toward 6–8 o’clock and enabled cannulation without any intraoperative complications ( Fig. 2 b, c ). Successful cannulation of APD was achieved through minor papilla ( Fig. 3 a ). Following dilation of APD with a balloon catheter ( Fig. 3 b ), the stones were extracted with a balloon extractor and a retrieval basket ( Fig. 3 c ). Two plastic stents (10 Fr, 5 cm and 7 Fr, 10 cm) were subsequently placed into APD ( Fig. 3 d ). The patient was observed for 2 days without any complications. And, no abdominal pain was revealed at 1-month follow-up.
a The guidewire passed retrogradely through the main pancreatic duct into the accessory pancreatic duct and coiled in the duodenal lumen. b A sphincterotome passed reversely through the minor papilla along the guidewire and performed reverse sphincterotomy. c The orifice of minor papilla after reverse sphincterotomy.
a Pancreatography showed successful cannulation through the accessory pancreatic duct. b A balloon catheter was used to dilate the accessory pancreatic duct. c A retrieval basket was used to clear the pancreatic duct stones. d Two plastic stents (10 Fr, 5 cm and 7 Fr, 10 cm) were placed in the accessory pancreatic duct.
ERCP is the first-line treatment for chronic pancreatitis (CP) patients 1 2 3 . However, cannulation of MPD can sometimes be difficult in cases such as pancreas divisum, MPD distortion, or obstruction due to pancreatic duct stones. In such scenarios, cannulation of APD serves as an alternative approach 4 . According to the experience of our center, approximately 20% of CP patients achieved treatment through minor papilla. Nevertheless, APD cannulation can be challenging if the orifice of minor papilla is inconspicuous. In this case, we employed a reverse sphincterotomy technique to facilitate the cannulation of minor papilla in a patient with CP, MPD distortion, and an inconspicuous accessory papillary orifice ( Video 1 ).
Reverse sphincterotomy assisted accessory pancreatic duct cannulation.Video 1
Endoscopy_UCTN_Code_TTT_1AR_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dumonceau JM Delhaye M Tringali A Endoscopic treatment of chronic pancreatitis: European Society of Gastrointestinal Endoscopy (ESGE) Guideline – Updated August 2018 Endoscopy 20195117919310.1055/a-0822-083230654394 · doi ↗ · pubmed ↗
- 2Zou WB Ru N Wu H Guidelines for the diagnosis and treatment of chronic pancreatitis in China (2018 edition)Hepatobiliary Pancreat Dis Int 20191810310910.1016/j.hbpd.2019.02.00430922816 · doi ↗ · pubmed ↗
- 3Strand DS Law RJ Yang DAGA Clinical Practice Update on the Endoscopic Approach to Recurrent Acute and Chronic Pancreatitis: Expert Review Gastroenterology 20221631107111410.1053/j.gastro.2022.07.07936008176 · doi ↗ · pubmed ↗
- 4Cai YL Wang F Liu M Reverse cannulation and dilation successfully assist the cannulation of the accessory pancreatic duct Endoscopy 202456 E 1042 E 104310.1055/a-2462-182539592101 PMC 11597888 · doi ↗ · pubmed ↗