Endoscopic ultrasonography-guided choledochoduodenostomy without tract dilation using a novel ultra-tapered slim-delivery metallic stent
Haruo Miwa, Ritsuko Oishi, Shotaro Tsunoda, Kazuki Endo, Yuichi Suzuki, Hiromi Tsuchiya, Shin Maeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
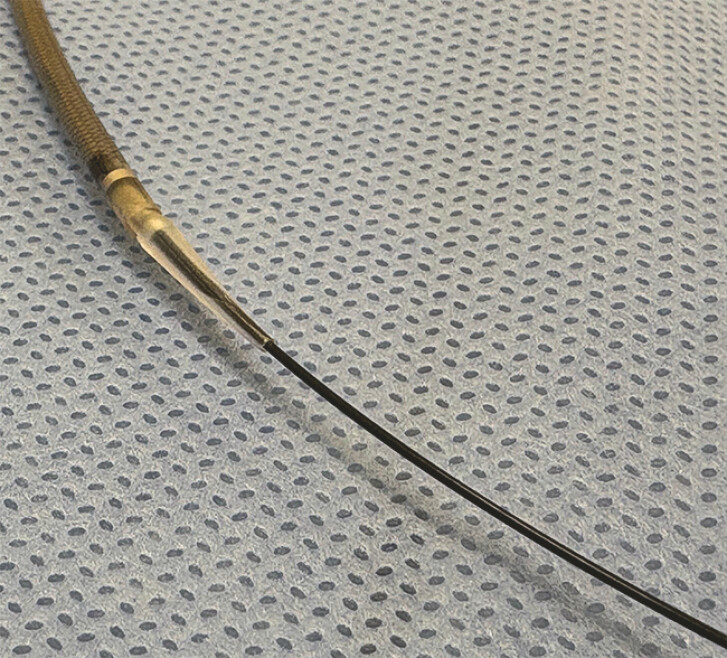 Fig. 1
Fig. 1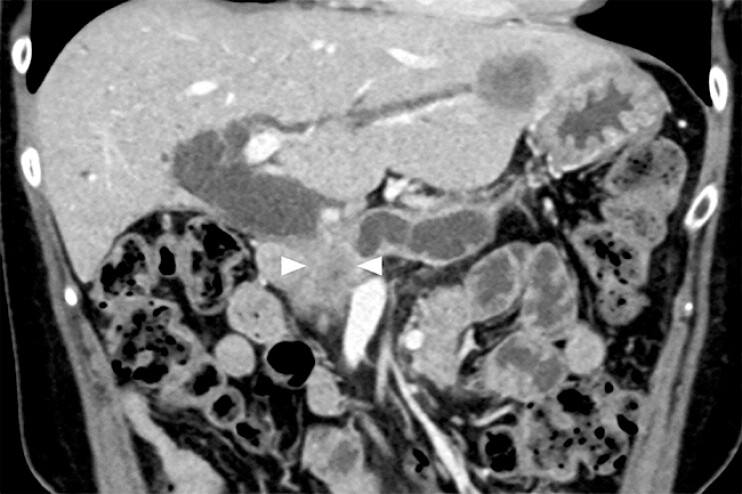 Fig. 2
Fig. 2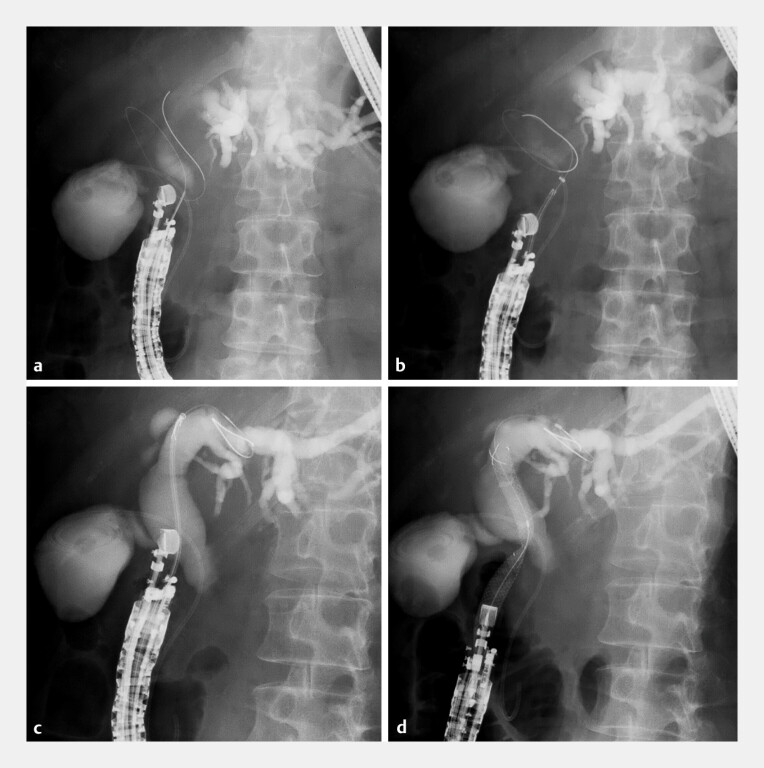 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pediatric Hepatobiliary Diseases and Treatments
Several techniques for endoscopic ultrasonography-guided choledochoduodenostomy (EUS-CDS) without tract dilation have been reported to reduce the risk of bile leakage 1 2 3 4 . However, bile leakage may still occur, particularly when the insertion of the stent delivery system is challenging. A novel self-expandable metallic stent (SEMS) with a 7-Fr slim delivery system (Niti-S EUS-BD system End Bare Single Flare; Taewoong Medical Co., Ltd., Gimpo, South Korea) features an ultra-tapered tip designed for use with a 0.025-in guidewire ( Fig. 1 ). Its cross-wire structure provides a high radial force that minimizes the risk of stent migration. Herein, we present a case of EUS-CDS performed without tract dilation using this novel SEMS ( Video 1 ).
A novel self-expandable metallic stent with a 7-Fr slim delivery system (Niti-S EUS-BD system End Bare Single Flare; Taewoong Medical Co., Ltd., Gimpo, South Korea) featuring an ultra-tapered tip that minimizes the gap with a 0.025-in guidewire.
A novel ultra-tapered slim-delivery metallic stent was used to perform endoscopic ultrasonography-guided choledochoduodenostomy without the need for tract dilation in a 64-year-old woman with unresectable pancreatic cancer, biliary obstruction, and liver metastasis.Video 1
A 64-year-old woman with unresectable pancreatic cancer complicated by biliary obstruction was admitted to our hospital. Computed tomography revealed multiple metastases in the left liver lobe ( Fig. 2 ). Initial transpapillary biliary drainage was attempted, but the guidewire could not be passed through the stricture. EUS-CDS was subsequently performed. A dilated common bile duct was punctured using a 19-gauge Franseen needle (TopGain; Medi-Globe GmbH, Grassau, Germany), and a 0.035-in guidewire was introduced. An attempt was made to insert a fully covered SEMS with an 8-Fr delivery system, but the tip of the system was unable to pass through the bile duct wall.
Computed tomography of a 64-year-old woman with unresectable pancreatic cancer and biliary obstruction (arrowheads) revealed liver metastasis in the left lobe.
A tapered catheter was then inserted, and the guidewire was exchanged for a 0.025-in version (VisiGlide 2; Olympus Medical Systems, Tokyo, Japan). Utilizing the ultra-tapered tip and the 7-Fr slim delivery system, the novel SEMS (8-mm diameter, 10-cm length) was advanced smoothly into the bile duct without the need for tract dilation. The stent was successfully deployed from the left hepatic duct to the duodenum ( Fig. 3 ). The patient recovered uneventfully and was discharged without adverse events.
Endoscopic ultrasonography-guided choledochoduodenostomy. a The dilated common bile duct was punctured using a 19-gauge Franseen needle. b A fully covered metallic stent with an 8-Fr delivery system could not pass through the bile duct wall. c The novel metallic stent with an ultra-tapered tip and 7-Fr slim-delivery system was smoothly advanced into the bile duct. d The metallic stent was placed successfully.
To the best of our knowledge, this is the first reported case of EUS-CDS performed without tract dilation using a novel SEMS with an ultra-tapered slim delivery system. This simple approach offers a safe technique for EUS-CDS.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogura T Itoi T Technical tips and recent development of endoscopic ultrasound-guided choledochoduodenostomy DEN Open 20211 e 810.1002/deo 2.835310149 PMC 8828248 · doi ↗ · pubmed ↗
- 2Koga T Hijioka S Nagashio Y Prospective clinical trial of EUS-guided choledochoduodenostomy without fistula dilation for malignant distal biliary obstruction Endosc Ultrasound 20231240941637969165 10.1097/eus.0000000000000009 PMC 10631599 · doi ↗ · pubmed ↗
- 3Okuno N Hara K Haba S The new potential for using Franseen needles in interventional EUS Intern Med 2024632723272710.2169/internalmedicine.3207-2338403760 PMC 11557192 · doi ↗ · pubmed ↗
- 4Inoue T Ibusuki M Kitano R Endoscopic ultrasound-guided choledochoduodenostomy using a novel, ultra-stiff, high-sliding guidewire and a dumbbell-shaped metal stent Endoscopy 202456 E 140E 14110.1055/a-2241-203038359881 PMC 10869224 · doi ↗ · pubmed ↗