Shallow endoscopic submucosal dissection using a gas-free immersion system to prevent strictures after esophageal dissections
Tatsuma Nomura, Hiroaki Kumazawa, Takanobu Mitani, Yoshiaki Isono, Tomohiro Sase, Tomonori Saito, Katsumi Mukai

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
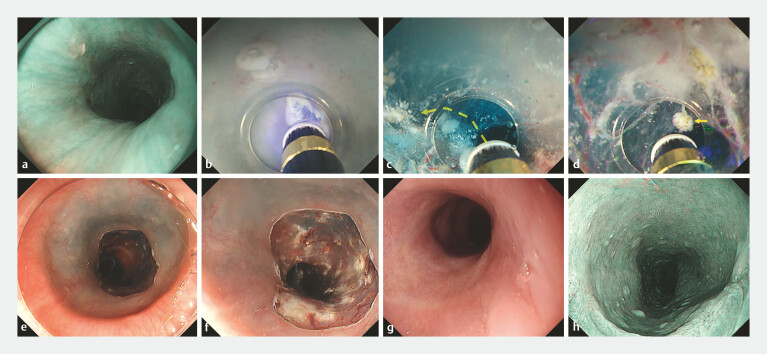 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Dysphagia Assessment and Management
Prevention of strictures after extensive esophageal endoscopic mucosal dissection (ESD) is important 1 2 . Currently, local injection or oral administration of steroids is widely used to prevent strictures; however, there is still no established method. In early esophageal cancer, there is a lymph node metastasis risk if even a small amount of extension is observed in the submucosa; therefore, there is no need for extensive submucosal resection for curable esophageal cancer. By leaving a thick submucosal layer above the muscle layer, it is possible to prevent esophageal stricture caused by damage to the muscle layer due to knife discharge during dissection. Therefore, we propose a submucosal dissection method that intentionally leaves a thick submucosal layer of the esophagus directly below the intrinsic esophageal gland. In this method, we used a gas-free immersion system (GFI). This saline-immersion method uses a 4 mm tapered tip hood to provide a 1.3-fold magnifying effect for precise ESD 3 4 .
The patient was a man in his 60s with a wide early esophageal cancer of the cervical esophagus ( Fig. 1 , Video 1 ). First, we made a circumferential incision, fixed the clip with a line to the normal mucosa on the oral side and applied traction. A tapered-tip CAST hood was then used to accurately dissect the submucosa directly below the muscularis mucosa through saline immersion 5 . Depending on whether the esophageal gland was identified or not, the dissection was performed directly below it or in the shallow submucosa directly below the muscularis mucosa, respectively. The tumor was completely resected within approximately 29 min. Triamcinolone 80 mg was injected locally, and the patient received oral steroids for 6 weeks. The tumor was diagnosed as a squamous cell carcinoma, pT1a. Follow-up endoscopy showed that the cervical esophagus had not narrowed, and the normal lumen width was maintained.
Partial-circumferential ESD of the cervical esophagus using a gas-free immersion system for shallow submucosal dissection. a Early esophageal cancer in the cervical esophagus. b Incision using a tapered tip hood on the mucosa, which narrowed after the local injection. c The submucosal layer shows the intrinsic esophageal gland (yellow arrow). The muscularis mucosa and intrinsic esophageal gland were visualized underwater using an endoscope, and the submucosal layer just below them was dissected. d The submucosal layer shows the esophageal gland, and the submucosal layer just below it is precisely dissected (yellow dotted arrow). The submucosal layer remains thick above the muscle layer. e Mucosal defect of 50 mm in diameter after ESD. f Defect after ESD after local steroid injection. Histopathology revealed that the lesion had been completely resected and that it was a squamous cell carcinoma with a depth of pT1a-LPM. g, h Ten weeks later, the ulcer had completely healed, and there was no stricture on endoscopy. Abbreviation: ESD, endoscopic submucosal dissection; LPM, lamina propria mucosa.
Shallow dissection using a gas-free immersion system for submucosal resection of the cervical esophagus and mucosal defects after healing.Video 1
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ishihara R Oyama T Takeuchi M Multicenter retrospective analysis of complications and risk factors in endoscopic resection for esophageal cancer across Japan Esophagus 20242143043710.1007/s 10388-024-01073-38981974 · doi ↗ · pubmed ↗
- 2Xu Y Wu Y Deng W More efficient endoscopic submucosal dissection with deep endotracheal intubation for superficial cervical esophageal carcinoma: a dual-center, prospective, randomized controlled study Gastrointest Endosc 202510165565810.1016/j.gie.2024.09.01839278284 · doi ↗ · pubmed ↗
- 3Nomura T Sugimoto S Hayashi Y Colorectal endoscopic submucosal dissection using a gas-free saline-immersion dissection technique Endoscopy 20235501 E 1039 E 104010.1055/a-2155-610737714199 PMC 10504036 · doi ↗ · pubmed ↗
- 4Nomura T Mitani T Toyoda J Gas-free immersion system with dual-channel scope for rapid hemostasis during gastric endoscopic submucosal dissection Endoscopy 20245601 E 734E 73539137911 10.1055/a-2376-1851 PMC 11321902 · doi ↗ · pubmed ↗
- 5Nomura T Sugimoto S Oyamada JGI endoscopic submucosal dissection using a calibrated, small-caliber-tip, transparent hood for lesions with fibrosis Video GIE 2021630130434278091 10.1016/j.vgie.2021.03.001PMC 8267961 · doi ↗ · pubmed ↗