Salvage endoscopic intermuscular dissection: curative treatment for residual rectal adenocarcinoma after chemoradiotherapy
Francisca Côrte-Real, Nuno Nunes, Ana Rita Silva, Nadine Amaral, Ana Catarina Rego, Maria Antónia Duarte

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
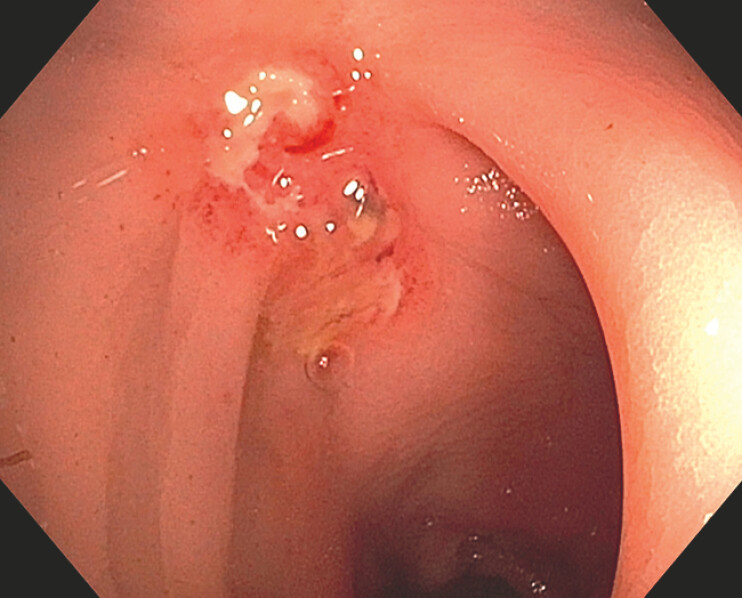 Fig. 1
Fig. 1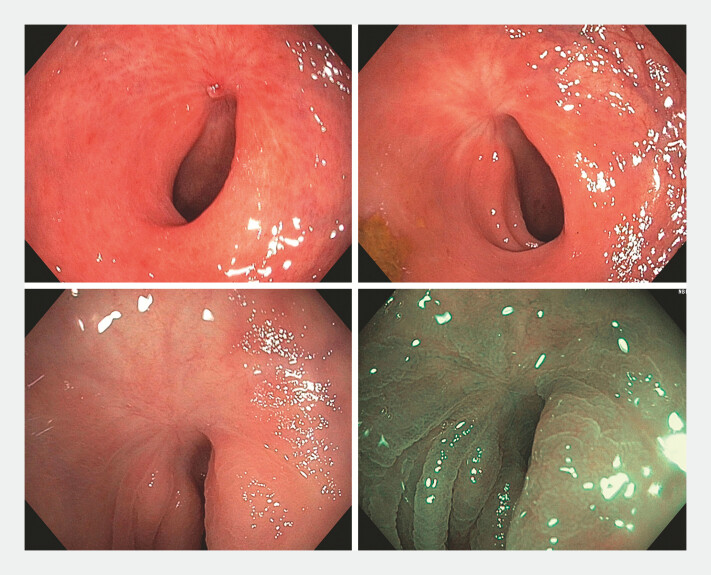 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Colorectal Cancer Surgical Treatments · Gastrointestinal Tumor Research and Treatment
We report the case of a 53-year-old male patient who underwent a total colonoscopy due to hematochezia and tenesmus. A circumferential vegetative lesion measuring approximately 50 mm in diameter, located 6 cm from the anal margin, was observed. Histology confirmed a moderately differentiated adenocarcinoma. The patient had a history of acute myocardial infarction 6 months earlier. Laboratory tests showed no anemia, and carcinoembryonic antigen (CEA) levels were within the normal range.
Pelvic magnetic resonance imaging (MRI) staged as T3bN0, with extramural vascular invasion (EMVI), without involvement of the mesorectal fascia. Computed tomography ruled out metastases.
The patient underwent neoadjuvant chemoradiotherapy, achieving a complete response on follow-up pelvic MRI. However, rectosigmoidoscopy revealed a flat lesion with central ulceration, measuring 20 mm ( Fig. 1 ). Histology confirmed the presence of adenocarcinoma.
Residual rectal adenocarcinoma.
The patient refused surgery. Following a discussion in a multidisciplinary team meeting, he underwent endoscopic intermuscular dissection of the lesion ( Video 1 ). Histology demonstrated an R0 resection of a moderately differentiated adenocarcinoma invading the submucosa, with preservation of the muscularis propria. No lymphovascular invasion, perineural invasion, or tumor budding was observed.
Endoscopic intermuscular dissection of the residual rectal lesion after chemoradiotherapy.Video 1
Endoscopic intermuscular dissection is widely used for the management of rectal lesions suspected of deep submucosal invasion. This technique allows for complete lesion excision and represents an emerging strategy in the treatment of rectal adenocarcinoma 1 .
This case underscores the relevance of endoscopic dissection in the management of colorectal lesions, including those under the watchful waiting approach. It could be used as a salvage method, potentially avoiding abdominoperineal amputation. The patient remains asymptomatic and under surveillance, with no evidence of recurrence at 20-month follow-up ( Fig. 2 ) 2 3 .
Surveillance rectosigmoidoscopies without recurrence.
Endoscopy_UCTN_Code_TTT_1AQ_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moons LMG Bastiaansen BAJ Richir MC Endoscopic intermuscular dissection for deep submucosal invasive cancer in the rectum: A new endoscopic approach Endoscopy 20225499399810.1055/a-1748-857335073588 · doi ↗ · pubmed ↗
- 2Klimkowski R Krzyzkowiak J Pilonis ND Endoscopic resection of residual rectal neoplasia after definitive chemoradiotherapy for rectal cancer Best Pract Res Clin Gastroenterol 20246810189610.1016/j.bpg.2024.10189638522889 · doi ↗ · pubmed ↗
- 3Leung G Nishimura M Hingorani N Technical feasibility of salvage endoscopic submucosal dissection after chemoradiation for locally advanced rectal adenocarcinoma Gastrointest Endosc 20229635936710.1016/j.gie.2022.02.01435183541 · doi ↗ · pubmed ↗