Impact of policies restricting advertising, promotion, and sponsorship of sugar-sweetened beverages: A systematic review
Leila Guarnieri, Lucas Perelli, Marcos Clausen, Germán Guaresti, Natalia Espinola, Andrea Graciano, Andrea Alcaraz, Leila Guarnieri, Lucas Perelli, Marcos Clausen, Germán Guaresti, Natalia Espinola, Andrea Graciano, Andrea Alcaraz

TL;DR
This paper reviews how policies banning sugar-sweetened beverage advertising can reduce consumption and improve health outcomes, especially in children.
Contribution
The study provides a systematic review of policies restricting sugar-sweetened beverage advertising and their health and economic impacts.
Findings
Policies restricting sugar-sweetened beverage advertising were linked to reduced consumption and improved health outcomes.
Most studies showed decreased economic and clinical measures following the implementation of these policies.
Restrictions on TV, school, and point-of-sale advertising were associated with lower exposure and consumption.
Abstract
To summarize the evidence on the impact of the implementation of the ban on the advertising, promotion and sponsorship (APS) of sugar-sweetened beverages (SSBs) in terms of decreased consumption, advertising exposure and relevant clinical outcomes. Systematic review of articles published between 2001-2021 in the PubMed, Embase, Global Health, CINAHL and LILACS databases written in English, Portuguese or Spanish. We included experimental, observational and economic model studies. Risk of bias was assessed using RoB2, Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group and Consolidated Health Economic Evaluation Reporting Standards 2022. We carried out a descriptive synthesis of the studies. We selected 11 out of 1146 identified studies. Due to the heterogeneity of the outcomes,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
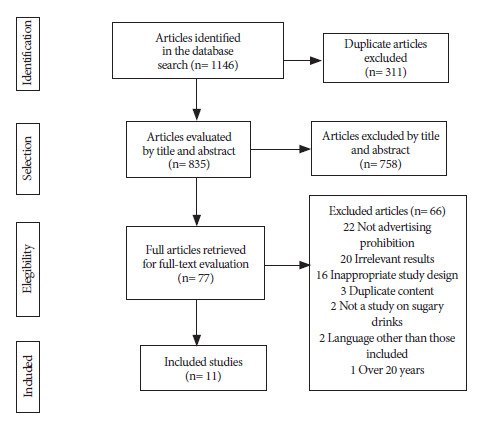 Figure 1
Figure 1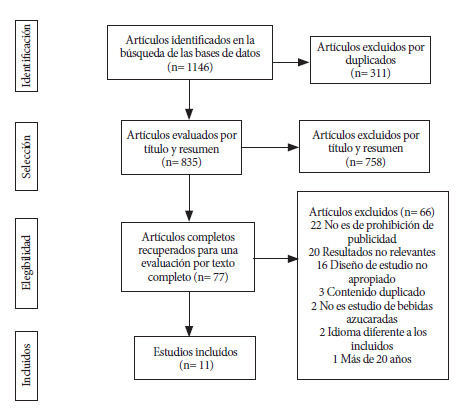 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvertising and Communication Studies · Agricultural and Food Production Studies
INTRODUCTION
Noncommunicable diseases (NCD), such as cardiovascular diseases, diabetes, and certain types of cancer, are the leading cause of death worldwide, affecting all age groups and all countries 1. The percentage of deaths attributable to NCDs increased from 60.8% in 2000 to 73.6% in 2019 worldwide and, particularly, from 77.2% to 81.3% in the Region of the Americas 2. NCDs also have a significant attributable cost to health systems and society in general, and this enormous disease and economic burden represents a significant barrier to achieving the Sustainable Development Goals (SDGs) 3.
Overweight and obesity are major risk factors for NCDs. Statistics are alarming for both adults and children and adolescents worldwide 4. The prevalence of obesity in children, girls and adolescents (BGaA) between the ages of 5 and 19 worldwide increased from 2.9% (95% CI: 2.6 to 3.2) in 2000 to 4.9% (95% CI: 4.6 to 5.3) in 2010, compared to 6.8% (95% CI: 6.1 to 7.6) in 2016. There have also been increases in the adult population regarding obesity rates in recent decades, reaching 13.1% (95% CI: 12.4 to 13.9) of this age group in 2016 2.
The increase in overweight and obesity levels has been linked to changes in food consumption patterns, as a result of stimuli that favor the consumption of high-calorie, low-nutritional-value products 5. In food environments, marketing and advertising influence both preferences and food purchasing and consumption decisions, especially among children and adolescents 6^,^7. Advertising and other forms of food and beverage marketing aimed at children and adolescents are widespread and focus mainly on products with excessive fat, sugar, or sodium content, such as SD. Evidence shows that children up to the age of 11 are not mature enough to differentiate advertising content from other types of messages 9, which makes this population particularly vulnerable. For this reason, international organizations such as PAHO/WHO and UNICEF are calling on countries to take immediate and urgent action to address the many nuances of this issue, such as regulating the advertising, promotion, and sponsorship (APS) of unhealthy products 5^,^10^-^12.
The consumption of SD is an important source of calories, generally without providing any nutrients other than sugars, increasing the risk of obesity, diabetes, heart disease, cerebrovascular disease, musculoskeletal disease, kidney failure, dementia, asthma, various types of cancer, and tooth decay 13^,^14. In addition, both obesity and tooth decay can lead to other social problems such as discrimination or lack of job opportunities 15.
In this context, restricting APS for unhealthy food and beverage products, especially those targeting children and adolescents, aims to reduce consumption of such products and is a cost-effective, feasible measure that is generally accepted by governments, policymakers, and the public 7. Systematic evidence on the health impact of implementing such regulations is essential to promote effective policies. Given that there no studies that have focused specifically on measures to restrict advertising of SD, this study conducted a systematic search with the aim of summarizing the evidence on the impact of implementing a ban on APS of SD in terms of reduced consumption, advertising exposure, and relevant clinical outcomes.
KEY MESSAGESMotivation for the study. Restrictions on advertising, promotion, and sponsorship (APS) of unhealthy food and beverage products aim to reduce their consumption and protect public health. No reviews have yet evaluated the impact of restricting APS of sugary drinks (SD).Main findings. We found that comprehensive policies that include TV advertising restrictions, as well as restrictions at points of sale and in schools, can effectively reduce SD consumption, especially among children and adolescents, decrease obesity, cardiovascular disease, diabetes, and cancer, and generate economic benefits.Implications. Evidence on the health impact of such interventions is essential to promote effective measures.
MATERIALS AND METHODS
Study design
We conducted a systematic review of the published literature following the PRISMA guidelines 16. (Supplementary material, Appendix 1).
Search strategy
The search included studies conducted at the national, regional, and international levels indexed in the PubMed, Embase, Global Health, CINAHL, and LILACS (Latin American and Caribbean Health Science Literature) bibliographic databases. The complete search strategy can be found in the supplementary material (Appendix 2).
Selection criteria
We included studies published in the last 20 years (2001-2021) in English, Portuguese, or Spanish; describing policies regulating APS of SD, whether mandatory or voluntary, independently or complementary to other policies; studies measuring the impact on consumption, purchases, sales, purchase intention, exposure, and/or clinical outcomes (obesity, caries, cardiovascular disease, high blood pressure, dyslipidemia, insulin resistance, diabetes, cancer, and other related clinical outcomes); and studies with experimental designs, controlled before-and-after studies, uncontrolled before-and-after studies, quasi-experimental studies, cross-sectional studies, economic models, economic evaluations, and cost studies. Studies that did not meet the inclusion criteria and those that analyzed the impact of regulatory policies on APS for non-sugar-sweetened beverages were excluded.
Study selection and data collection
Each of the identified studies was evaluated by two reviewers from the research team assigned randomly at each stage of the process, who initially selected those that met the inclusion criteria based on the title and abstract, and subsequently by reading the full texts, using the COVIDENCE® computer program 17. When discrepancies arose between reviewers, they were discussed among the entire research team to reach a final consensus decision. Each of the selected studies was then randomly assigned to a researcher to identify and extract relevant information, with individual concerns that arose during the process being resolved as a group to reach a conclusion.
We constructed a descriptive summary of the main characteristics of the studies, considering the type of design, the interventions, their degree of implementation, and the outcomes. It was not possible to perform a meta-analysis given the high heterogeneity of the interventions, the target populations, and the outcomes evaluated in each study.
Assessment of risk of bias in included studies (quality)
Pairs of reviewers independently assessed the risk of bias (quality) of the included studies. In case of disagreement, it was resolved by group consensus. Due to the nature of the research question, a single tool was not considered applicable; instead, a combination of validated instruments was used according to the study designs. The RoB2 tool 18 was used for randomized clinical trials, the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies 19 was used for cross-sectional designs, the Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group 19 was used for controlled and uncontrolled before-after studies and for quasi-experimental studies; and the Consolidated Health Economic Evaluation Reporting Standards 2022 checklist 20 was used for economic models, developed with the main purpose of serving as a report guide.
RESULTS
Study selection
We identified 1,146 studies from the databases using the search strategy. After removing duplicates (n=311), the remaining 835 were analyzed using the inclusion criteria based on title and abstract. A total of 758 studies were excluded in this first stage, and the remaining 77 were identified as eligible for full-text analysis. Finally, 11 articles ^(21-31)^ were eligible for this systematic review (Table 1). The complete study selection process is shown in Figure 1.
Table 1. Description of the included studies.AuthorsYearCountryDesignEvaluated interventionAnalyzed variables
ObesityCardiovascular diseaseDiabetesCancerPurchaseSaleCost-effectivenessOther economic outcomesConsumptionExposureBrimblecombe *et al.*2020AustraliaRandomized clinical trialRestrictions on POS
x
Brown *et al.*2018AustraliaEconomic modelRestrictions on TV advertising aimed at BGaAx
x x Correa *et al.*2020ChileUncontrolled before and after studyRestrictions on TV advertising aimed at BGaA
xHuse *et al.*2020AustraliaModelPromotion restrictionsxxxx
xxx Magnus *et al.*2009AustraliaModelRestrictions on TV advertisingx
x
Miller *et al.*2016United States of AmericaCross-sectionalRestriction on promotions in schools
x Mytton *et al.*2020United KingdomModelRestrictions on TV advertisingx
xxxxPauzé & Potvin Kent2021CanadaQuasi-experimental studyRestriction of TV advertising aimed at BGaA (self-regulation)
xPolacsek *et al.*2012United States of AmericaCross-sectionalRestrictions on advertising in schools
xPotvin Kent & Wanless2014CanadaUncontrolled before and after studyRestriction of TV advertising aimed at BGaA (self-regulation)
xTaillie *et al.*2020ChileControlled before and after studyComprehensive policy ^a^
x
POS: Point of sale; BGaA: boys, girls and adolescents; TV: Television; ^a^ Includes front-of-pack labeling, restrictions on advertising aimed at BGaA, and restrictions on sales in schools.
Figure 1. Selection process for studies included in the review.
General characteristics
Regarding methodological designs, there was considerable heterogeneity among the studies, with most being economic impact models. In terms of interventions, of the eleven articles, six analyzed television advertising restrictions 22^,^23^,^25^,^27^,^28^,^30, two analyzed restrictions in schools ^(26, 29)^, one analyzed restrictions on promotions (defined as temporary price reductions and product offers) 24, one on point-of-sale restrictions 21, and one on comprehensive policy 31^)^ (Table 1). The supplementary material (Appendix 3) provides more details on the characteristics of each of the interventions evaluated in the studies.
Most studies evaluated exposure (n=5) 23^,^27^-^30, followed by obesity (n=4) 22^,^24^,^25^,^27, cost-effectiveness (n=4) 22^,^24^,^25^,^27, consumption (n=4) 22^,^24^,^26^,^27, other economic outcomes (n=2) 24^,^27, cardiovascular disease (n=1) 24, diabetes (n=1) 24, cancer (n=1) 24, purchase (n=1) 31, and sale (n=1) 21. No study evaluated the impact on caries, high blood pressure, dyslipidemia, or insulin resistance (Table 1).
Assessment of evidence quality (risk of bias)
Five studies used evidence of high quality ^(22, 24, 25, 27, 31)^, three used moderate evidence ^(21, 23, 26)^, and three used low-quality evidence 28^-^30. (Table 2). The tables corresponding to the assessment of the quality of the studies according to each design are presented in the supplementary material (Appendix 4).
Table 2. Quality of studies included in the systematic review.Author and yearStudy designTool usedResultBrimblecombe et al, 2020Randomized clinical trialRoB2ModerateBrown et al, 2018Economic modelCHEERS 2022HighCorrea et al, 2020Uncontrolled before and after studyQuality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group (NIH)ModerateHuse et al, 2019ModelCHEERS 2022HighMagnus et al, 2009ModelCHEERS 2022HighMiller et al, 2016Cross-sectionalQuality Assessment Tool for Observational Cohort and Cross-Sectional Studies (NIH)ModerateMytton et al, 2020ModelCHEERS 2022HighPauzé & Potvin Kent, 2021Quasi-experimental studyQuality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group (NIH)LowPolacsek et al, 2012Cross-sectionalQuality Assessment Tool for Observational Cohort and Cross-Sectional Studies (NIH)LowPotvin Kent and Wanless, 2014Uncontrolled before and after studyQuality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group (NIH)LowTaillie et al, 2020Controlled before and after studyQuality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group (NIH)HighCHEERS: Consolidated Health Economic Evaluation Reporting Standards.
Results according to interventions
The study that analyzed the impact of a comprehensive policy 31 after 18 months of implementation in Chile, which includes the adoption of front-of-package warning labels, restrictions on advertising of labeled products to children and adolescents, and a ban on their sale and advertising in schools, reported a reduction in purchases of beverages labeled with the warnings of -23.7% (-23.8% to -23.7%).
With regard to television advertising restrictions, when evaluating exposure, several studies were inconclusive: while an economic impact model 27 and another study on the policy implemented in Chile 24 showed decreases, analyses of the voluntary measure taken by the Canadian food and beverage industry reported increases in one case 28 and increases and decreases in another 30. Regarding obesity, three studies, which evaluated changes in BMI 22^,^25 and in the number of children and adolescents with obesity 27, found decreases in these outcome measures. Similarly, three models 22^,^25^,^27 demonstrated that time restrictions on advertising unhealthy products would be cost-effective. Two of the studies ^(22, 27)^ found that advertising restrictions would lead to decreases in the daily energy intake of children and adolescents. One of the studies reported cost savings attributable to the implementation of restrictions 27.
Regarding restrictions on promotions, the same study 24 reported decreases in body weight and BMI in the population, as well as new cases prevented and years of life saved from cardiovascular disease, diabetes, and cancer as a result of eliminating all price promotions on SD. The same study 24 demonstrated that the intervention would be cost-effective, yield cost savings, and reduce daily energy intake.
Meanwhile, when analyzing restrictions at the point of sale, a randomized clinical trial 21 conducted over 12 weeks showed that following the implementation of a series of measures in retail stores in Australian towns, sales of free sugars in APSs fell by 6.8% (95% CI: -10.9% to -2.6%).
Finally, studies on restrictions in schools conducted in the United States showed, in one case 26, that school districts that apply restrictions on SDs have lower regular consumption of soft drinks; while another study showed that, despite a state ban on unhealthy product brands, there were still a large number of advertising strategies in the school environment, many of them involving SD 29.
None of the studies analyzed global APS restrictions that apply exclusively to SDs (Table 3, Annex 3).
Table 3. Impact identified according to types of interventions evaluated.Evaluated interventionOutcomeAuthors and yearMain resultsComprehensive policy ^a^PurchaseTaillie et al, 2020The average daily per capita volume (mL) of “high-sugar” beverages purchased decreased by 23.7% (from −23.8% to −23.7%).TV advertising restrictionsObesityBrown et al, 2018The average BMI in children aged 5 to 15 years (kg/m^2^) decreased by 0.352.
Mytton et al, 2020Following the intervention, the number of children aged 5 to 17 with obesity could decrease by 4.6% (95% CI: 1.4%-9.5%), equivalent to 40,000 fewer children with obesity.
Magnus et al, 2009The restrictions would result in a reduction in BMI (units) of 0.04 (95% CI: 0.01, 0.08). Cost-effectivenessMytton et al, 2020Restrictions on advertising foods and beverages high in fat, sugar, and salt would prevent 240,000 (95% CI: 65,000-530,000) DALYs, resulting in a monetary benefit of £7.4 billion (95% CI: £2 billion-£16 billion).
Magnus et al, 2009The cost-effectiveness of the intervention, measured as ICER, was AUD2.40-$7.70) per DALY. The intervention was considered “dominant” because it resulted in a benefit in health and a reduction in costs.
Brown et al, 2018The cost-effectiveness of the intervention, measured as ICER, showed a 100% probability of being “dominant,” resulting in 88,396 HALYs saved (95% CI: 54,559-123,199) and total cost savings of AUD369.8 million-AUD$1.2 billion) at the population level over a lifetime. Other economic outcomesMytton et al, 2020The intervention would result in: Healthcare cost savings (millions): £84 (£23-£190) Social care cost savings (millions): £210 (£56-£490) Net monetary health-related benefit (millions): £7,400 (£2,000-£16,000) ExposureMytton et al, 2020The intervention would result in an average reduction in exposure (number of advertisements for products high in sugar, fat, and/or sodium seen per day) in BGaA of 1.5.
Correa et al, 2020As a result of the policy implementation, there was a decrease in TV advertisements of: Number of appearances of “soft drinks”: 51% (p < 0.01) Number of appearances of “sports and energy drinks”: 23% (p < 0.01)
Pauzé & Potvin Kent, 2021BGaA exposure to sugary drink advertisements (measured as the number of advertisements viewed by BGaA) increased by 495% between May 2011 and May 2019.
Potvin Kent & Wanless, 2014Exposure, measured as the average number of advertisements for sugary drinks seen by children aged 2-11, showed differences between 2006 and 2009: juice advertisements decreased by 62.6% in Toronto and 51.6% in Vancouver; soft drink advertisements decreased by 37.8% in Toronto and increased by 11.1% in Vancouver. ConsumptionMytton et al, 2020In response to the restrictions, there would be a reduction in the average daily energy intake in BGaA of 9.1 kcal/day (95% CI: 0.5-17.7).
Brown et al, 2018The implementation of the restriction would result in an average decrease in energy intake in children and adolescents aged 5 to 15 years of 115 kJ/day (27.5 kcal).Promotion restrictionsObesityHuse et al, 2019The intervention resulted in a mean change in body weight in the population (kg) of −0.11 (95% CI: −0.14 to −0.08) and a mean change in BMI in the population (kg/m2) of −0.04 (95% CI: −0.05 to −0.03). Cardiovascular diseaseHuse et al, 2019As a result of the intervention, 3,609 (95% CI: 2,625-4,688) new cases of heart disease would be prevented, saving 11,941 (95% CI: 8,967-15,322) years of life. DiabetesHuse et al, 2019As a result of the intervention, 14,319 (95% CI: 10,198-19,282) new cases of diabetes would be prevented and, as a consequence, 5,041 (95% CI: 3,604-6,779) years of life would be saved. CancerHuse et al, 2019As a result of the intervention, 846 (95% CI: 395-1485) cases of colorectal, breast, endometrial, and kidney cancer would be prevented, saving 2,798 (95% CI: 1,822-4,067) years of life. Cost-effectivenessHuse et al, 2019The cost-effectiveness of the intervention, measured as ICER, was found to be dominant, with a total of 34,260 HALYs gained (24,922-45,504) and total cost savings of AUD260.1 million to −AUD$477.7 million). Other economic outcomesHuse et al, 2019The intervention would result in total cost savings of: −AUD376.0 million (95% CI: −AUD277.4 million to −AUD494.3 million) ConsumptionHuse et al, 2019The intervention resulted in an average change in daily energy intake of −12.52 kJ (95% CI: −15.91 to −9.58) per person.POS restrictionsSaleBrimblecombe et al, 2020The implementation of restrictions led to a statistically significant reduction in sales of free sugars in SD (g/total MJ): -6.8% (-10.9 to -2.6).Restrictions in schoolsConsumptionMiller et al, 2016Districts that apply restrictions on promotional products have 16% less regular consumption of soft drinks. ExposurePolacsek et al, 2012An average of 49 food and beverage posters and signs were found in different areas, 45% of vending machine advertising was for Coca-Cola® and PepsiCo®.BGaA: boys, girls and adolescents; DALYs: Disability-adjusted life years; ICER: Incremental cost-effectiveness ratio; HALYS: Total health-adjusted life years; POS: Point of sale; SB: Sugar-sweetened beverages; ^a^ Includes front-of-package labeling, restrictions on advertising aimed at children and adolescents, and restrictions on sales in schools. £: Pound.
DISCUSSION
The results of this study show that interventions restricting the APS of food and beverage products with excessive amounts of sugars, fats, and/or sodium, such as SDs, could be beneficial in terms of clinical, economic, consumption, and exposure outcomes. These results are consistent with those reported by Boyland et al. 32, who found that restrictions on the marketing of unhealthy products can help reduce their purchase, their negative health consequences, and also limit exposure to and/or the power of such marketing.
One of our main findings shows that, when implementing a comprehensive policy of front-of-package warning labels, restrictions on advertising labeled products to children and adolescents, and a ban on their sale and advertising in schools in Chile, the purchase of SD decreased, proving to be an effective measure for improving health 31. It should be noted that in Chile, beverages sweetened with non-caloric sweeteners are not covered by the restrictions, and decreases in SD purchases were accompanied by an increase in purchases of beverages with sweeteners 33. In this regard, it will be essential to monitor the impact of similar policies adopted in countries such as Mexico 34 and Argentina 35, where products with non-caloric sweeteners are covered.
Furthermore, it should be noted that, worldwide, most of the implemented policies correspond to restrictions on television advertising aimed at children and adolescents 36; accordingly, most of the studies included in this paper refer to television restrictions, and they particularly highlight the impact of these measures on exposure to advertising for unhealthy products. However, given the increasing exposure of children and adolescents to advertising in video games and social media such as YouTube, TikTok, and Instagram 37, international organizations recommend that regulations also include digital media 38. In this regard, although some countries, such as Argentina, Chile, and the United Kingdom, have adopted measures that incorporate this type of media 35^,^36, their monitoring and enforcement by governments is recognized as one of the main challenges to be overcome 38.
Another noteworthy finding is the ineffectiveness of voluntary initiatives by the food and beverage industry to reduce children and adolescents’ exposure to SD advertising. Contrary to their intended objective, two evaluations included in this study show that since their implementation, their indicators increased 28^,^30. These results are consistent with those reported by Théodore et al., who demonstrated that, despite the self-regulation initiative in Mexico, SD companies continued to implement advertising strategies aimed at children 39. In this regard, it is important to note that the World Health Organization recommends that policies aimed at restricting advertising of unhealthy foods and beverages to children and adolescents be mandatory 7.
Furthermore, this study shows that even when restrictions are targeted at the point of sale, including strategies such as no promotional activities and no discretionary foods and beverages available at the counter 21, results that contribute to improving health can be achieved. In this regard, the World Health Organization has recognized retailers as a central link in the food environment, highlighting the importance of interventions in these areas 40, so that point-of-sale restrictions tailored to each particular context could also be effective strategies.
One of the main limitations of this study is that a significant proportion of the included studies correspond to economic impact models 22^,^24^,^25^,^27, which means that the actual impact of implementing the interventions analyzed may differ from what was reported. In addition, several studies were of low quality ^(28-30)^, and their results should therefore be interpreted with caution. In turn, the quasi-experimental study 28^)^ and the uncontrolled before-and-after studies 23^,^30^)^ could have biases, particularly regarding sample selection regarding the analyzed periods. Furthermore, due to the heterogeneity of the results found in the many studies, it was not possible to group them, making comparison difficult.
On the other hand, a notable limitation is the lack of evidence on policies implemented to restrict APSs in SD. It is also worth noting the scarcity of studies that report on the impact in relation to clinical outcomes, such as diabetes and cardiovascular disease. Despite this, the economic impact models included in this review provide evidence of the potential effectiveness of these measures, helping to fill these gaps. In addition, some studies 22^,^27 report outcomes from APS restrictions on products high in sugar, fat, and salt, without focusing exclusively on SD. In any case, given that SD are among the main ultra-processed products advertised 41 and that they provide half of the sugars in the diet 42, a large part of the impact of measures restricting the APS of products high in critical nutrients in general could be attributed to restrictions on SD.
The main strength of this study lies in the fact that it is one of the few systematic reviews available on the impact of APS restrictions on unhealthy food and beverage products, such as SDs. Our results demonstrate the effectiveness of different interventions across different variables and could be used to support the promotion of effective policies that contribute to improving people’s health, with a special emphasis on children and adolescents.
In conclusion, this study shows that policies that include restrictions on the APS of SD could be effective in reducing their consumption, which could lead to health benefits, especially for children and adolescents. However, it is necessary to continue working on medium- and long-term impact assessments of the measures that are beginning to be implemented in different countries around the world in order to obtain information about their effectiveness on consumption and clinical indicators such as obesity, cardiovascular disease, diabetes, and cancer. In addition, further research is needed to demonstrate the impact of the APS of SD restriction policies that extend to digital media, as well as the application of methodologies to help monitor them adequately
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1OMS Enfermedades no transmisibles Internet Organización Mundial de la Salud 2023 https://www.who.int/es/news-room/fact-sheets/detail/noncommunicable-diseases
- 2World Health Organization World health statistics 2022: monitoring health for the SD Gs, sustainable development goals 2022 Geneva WHO 22 de abril de 2024 Disponible en: https://cdn.who.int/media/docs/default-source/gho-documents/world-health-statistic-reports/worldhealthstatistics_2022.pdf?sfvrsn=6fbb 4d 17_3
- 3World Health Organization GLOBAL STATUS REPORT on noncommunicable diseases 2014 Internet Geneva WHO 22 de abril de 2024 Disponible en: https://iris.who.int/bitstream/handle/10665/148114/9789241564854_eng.pdf?sequence=1&is Allowed=y
- 4Organización Mundial de la Salud Obesidad y sobrepeso Internet 2024 https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight
- 5UNICEF Obesidad: una cuestión de derechos de niños, niñas y adolescentes. Recomendaciones de políticas para su protección Internet Buenos Aires 22 de abril de 2024 Disponible en: https://www.unicef.org/argentina/media/4996/file/Obesidad,%20una%20cuesti%C 3%B 3n%20de%20derechos.pdf
- 6Smith R Kelly B Yeatman H Boyland E Food Marketing Influences Children's Attitudes, Preferences and Consumption: A Systematic Critical Review Nutrients 201911410.3390/nu 11040875 PMC 652095231003489 · doi ↗ · pubmed ↗
- 7World Health Organization Policies to protect children from the harmful impact of food marketing: WHO guideline World Health Organization Internet 2023 https://iris.who.int/bitstream/handle/10665/370113/9789240075412-eng.pdf?sequence=1&is Allowed=y 37440677 · pubmed ↗
- 8Organización Panamericana de la Salud Consumo de productos alimentarios ultraprocesados y procesados con exceso de nutrientes asociados a las enfermedades crónicas no transmisibles y a la alimentación insalubre en las Américas Internet Organización Panamericana de la Salud 2022 https://iris.paho.org/handle/10665.2/55547