Late Pancreatic Metastasis From Papillary Thyroid Carcinoma Diagnosed by Endoscopic Ultrasound-Guided Tissue Acquisition
César Vivian Lopes, Júlia Fernanda Semmelmann Pereira-Lima, Marianna Lins de Souza Salerno, Felipe Luzzatto

TL;DR
A patient with papillary thyroid cancer developed a rare pancreatic metastasis 11 years after treatment, diagnosed via endoscopic ultrasound and managed with radiotherapy.
Contribution
This case highlights the rare occurrence of pancreatic metastasis from thyroid cancer and the diagnostic utility of endoscopic ultrasound-guided biopsy.
Findings
Pancreatic metastasis from papillary thyroid carcinoma was diagnosed 11 years after initial treatment.
Endoscopic ultrasound-guided biopsy confirmed metastasis using thyroglobulin and thyroid transcription factor 1 markers.
The patient was treated with stereotactic body radiotherapy due to non-iodine-avid tumor characteristics.
Abstract
Papillary thyroid carcinoma, the most common differentiated thyroid cancer, has an indolent clinical course and a good prognosis. Metastases to the gastrointestinal tract account for <1% of all distant metastases, and the pancreas is an extremely rare site for metastasis from thyroid cancer. We report the case of a patient who developed a pancreatic metastasis from a classic variant papillary thyroid carcinoma 11 years after total thyroidectomy, cervical lymphadenectomy, and radioactive iodine ablation. The patient experienced increased thyroglobulin levels, and abdominal computed tomography scan revealed a lesion in the uncinate process of the pancreas. Tissue samples obtained by endoscopic ultrasound-guided biopsy were positive for thyroglobulin and thyroid transcription factor 1. Because the patient was not a candidate for surgery, the metastatic lesion was not iodine-avid, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1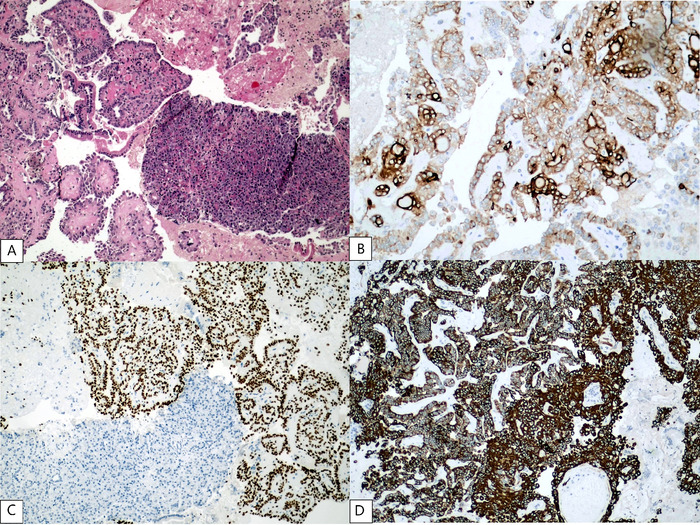 Figure 2
Figure 2 Figure 3
Figure 3| Study | Age, years | Sex | Histology | TNM Classification | Stage | Thyroidectomy | RAI | Locoregional Recurrence | Metastases Before Pancreatic Metastasis |
|---|---|---|---|---|---|---|---|---|---|
| Sugimura et al, 1991 | 32 | F | Classic | NR | NR | Total | NR | NR | NR |
| Jobran et al, 2000 | 52 | M | Tall cell | T4aN1M0 | I | Total | Yes | Yes | No |
| Meyer and Behrend, 2006 | 62 | M | Classic | T4aN0M0 | III | Total | Yes | Yes | Lung, adrenal |
| Siddiqui et al, 2006 | 62 | M | Tall cell | T4aN1bM0 | III | Total | Yes | No | Lung |
| Angeles-Angeles et al, 2009 | 72 | M | Classic | T4bNxM1 | IVB | None | Yes | No | No |
| Chen and Brainard, 2010 | 77 | M | Classic | T3N1M0 | II | Total | Yes | Yes | No |
| Borschitz et al, 2010 | 34 | F | Follicular | T3N1aM0 | I | Total | NR | Yes | No |
| 46 | M | Classic | T3N1M0 | I | Total | Yes | Yes | No | |
| Alzahrani et al, 2012 | 47 | M | Classic | T4aN1bM0 | I | Total | Yes | Yes | Lung |
| Olson et al, 2013 | 59 | F | Classic | NR | NR | NR | NR | NR | No |
| Tunio et al, 2013 | 60 | M | Follicular | T2N1M0 | II | Total | Yes | No | No |
| Li et al, 2014 | 55 | M | Classic | NR | NR | Partial | NR | Yes | No |
| Davidson et al, 2017 | 82 | F | Tall cell | T3N1bM0 | II | Total | Yes | Yes | No |
| Murakami et al, 2018 | 66 | F | Classic | T4aN1bM0 | III | Total | NR | Yes | No |
| Cho et al, 2019 | 71 | M | Classic | NR | NR | Total | Yes | Yes | Lung |
| Yang et al, 2019 | 48 | M | Classic | T4aN1M1 | II | Total | Yes | No | No |
| Tramontin et al, 2020 | 67 | M | Classic | T4aN1bM0 | III | Total | Yes | Yes | No |
| Ren et al, 2020 | 47 | M | Classic | T4aN0M1 | II | Total | Yes | No | No |
| Rossi et al, 2020 | 45 | M | Classic | NR | NR | NR | NR | Yes | Lung, brain |
| Uslar et al, 2020 | 80 | M | Tall cell | T4aN1M1 | IVB | Total | Yes | No | No |
| Yoon et al, 2020 | 71 | M | Classic | T3NxM0 | II | NR | NR | NR | NR |
| 61 | M | Classic | T3N1bM0 | II | NR | NR | NR | NR | |
| Stein et al, 2020 | 46 | M | Tall cell | T4aN1M0 | I | Total | Yes | Yes | No |
| Wong et al, 2021 | 68 | M | Classic | NR | NR | NR | Yes | NR | NR |
| Warda et al, 2022 | 46 | M | Tall cell | T4aN1M0 | I | Total | Yes | Yes | No |
| Song et al, 2023 | 51 | M | Classic | T3N1bM0 | I | Total | Yes | Yes | No |
| Ahmadian et al, 2024 | 66 | M | Classic | NR | NR | Total | Yes | NR | NR |
| Present case | 79 | F | Classic | T2N1M0 | II | Total | Yes | No | No |
| Study | Time After PTC Diagnosis, years | Clinical Features | Imaging | Iodine- Avid | Local | Size, cm | Solid/Cyst | Sampling | Other Metastases at Diagnosis of PM | Treatment | Follow-up, months | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sugimura et al, 1991 | 7 | Jaundice, itching | CT, US | NR | Head | 3 | NR | NR | No | Surgery (PD) | NR | NR |
| Jobran et al, 2000 | 1 | Abdominal pain | MRI | No | Head | 3.5/2.5 | Cyst | CT-FNA | Lung, vertebra | Surgery (PD), carboplatin and doxorubicin | 0.5 | Died |
| Meyer and Behrend, 2006 | 5 | Anemia, duodenal bleeding ulcer | CT | No | Head | NR | Cyst | Endoscopic biopsy of duodenal ulcer | Lung, liver, kidney | Surgery (DP) | 54 | Died |
| Siddiqui et al, 2006 | 7 | Abdominal pain | CT, PET | No | Head | 1.5 | Solid | EUS-TA | Lung | Surgery (PD) | 24 | Alive |
| Angeles-Angeles et al, 2009 | Synchronous | Abdominal pain | CT | NR | Tail | 8.5 | Solid | Upfront surgery | Brain, vertebra | Surgery (DP) | 8 | Alive |
| Chen and Brainard, 2010 | 5 | Pancreatitis | EUS | NR | Neck | 3 | Solid | EUS-TA | NR | NR | NR | NR |
| Borschitz et al, 2010 | 10 | NR | CT, PET, MRI | No | Head | 4 | Solid | Upfront surgery | No | Surgery (DP) | 7 | Alive |
| 15 | NR | CT, PET | No | Body | NR | Solid | Upfront surgery | Lung, bone, skin | Surgery (enucleation), RAI | 36 | Died | |
| Alzahrani et al, 2012 | 8 | Asymptomatic | PET, MRI | No | UP | 1.7 | Solid | EUS-TA | Lung, vertebra, liver, peritoneum | Sorafenib | 20 | Died |
| Olson et al, 2013 | Synchronous | NR | NR | NR | NR | NR | NR | EUS-TA | NR | NR | NR | NR |
| Tunio et al, 2013 | 7 | Abdominal pain | CT, MRI | No | Neck | 1.8 | Solid | CT-FNA | Lung | Surgery (PD), sorafenib | 36 | Alive |
| Li et al, 2014 | 11 | Asymptomatic | CT, PET | NR | Body/tail | 6.2 | Solid | Upfront surgery | No | Surgery (DP) | 5 | Died |
| Davidson et al, 2017 | 2 | Asymptomatic | CT, PET | NR | Body | 1.1 | Solid | EUS-TA | No | Surveillance | 6 | Alive |
| Murakami et al, 2018 | 14 | Asymptomatic | CT, PET, MRI | NR | Body | 3 | Solid | EUS-TA | Lung | Surgery (DP), paclitaxel | 11 | Died |
| Cho et al, 2019 | 10 | Asymptomatic | PET, MRI | NR | Body | 1.4 | Solid | EUS-TA | Lung | Surveillance | 1 | Alive |
| Yang et al, 2019 | Synchronous | Abdominal pain | US | NR | Body | 2.5 | Solid | Upfront surgery | Lung, liver, kidney, parotid, skin, skeletal muscle, bone | Surgery (DP), lenvatinib | 18 | Alive |
| Tramontin et al, 2020 | 6 | Jaundice, nausea, weight loss | PET | NR | Head | 3.5 | Solid | EUS-TA | No | Surgery (PD), sorafenib | 7 | Alive |
| Ren et al, 2020 | Synchronous | Abdominal pain | CT, US | NR | Body | 4 | Solid | Upfront surgery | Liver, diaphragm, parotid | Surgery (DP), RAI | 5 | Alive |
| Rossi et al, 2020 | 15 | Pancreatitis | CT, MRI | NR | Head | 2 | Solid | EUS-TA | No | Surgery (PD) | NR | NR |
| Uslar et al, 2020 | Synchronous | Jaundice | CT, PET, MRI, | NR | Head | 3.6 | Solid | EUS-TA | Lung, brain, skeletal muscle | RAI and RT | 12 | Alive |
| Yoon et al, 2020 | NR | NR | CT, PET | NR | Head | 6 | Solid | EUS-TA | Lung | Lenvatinib | 36 | Alive |
| NR | Asymptomatic | NR | NR | Body/tail | 7 | NR | CT-FNA | Lung, bone | Lenvatinib | 23 | Alive | |
| Stein et al, 2020 | 3 | NR | PET | No | Head | 3 | Solid | Upfront surgery | Vertebra | Surgery (PD), lenvatinib | 6 | Alive |
| Wong et al, 2021 | 7 | NR | PET | Yes | Body/tail | NR | Solid | NR | NR | RAI | NR | NR |
| Warda et al, 2022 | 3 | NR | PET | NR | Head | 3 | NR | Upfront surgery | No | Surgery (PD), lenvatinib | NR | Alive |
| Song et al, 2023 | 6 | Diabetes | CT, PET, MRI | NR | Tail | 5.6 | Cyst | Upfront surgery | No | Surgery (DP) | 36 | Alive |
| Ahmadian et al, 2024 | 5 | Asymptomatic | CT, PET | NR | Tail | NR | Solid | EUS-TA | Liver, adrenal, peritoneum | NR | NR | NR |
| Present case | 11 | Asymptomatic | CT, PET | No | UP | 4 | Cyst | EUS-TA | Liver, vertebra, retroperitoneal lymph node | RAI, RT | 23 | Died |
| Study | Thyroglobulin | Thyroid Transcription Factor 1 | BRAFV600E Mutation |
|---|---|---|---|
| Sugimura et al, 1991 | NR | NR | NR |
| Jobran et al, 2000 | Positive | NR | NR |
| Meyer and Behrend, 2006 | Positive | NR | NR |
| Siddiqui et al, 2006 | Positive | Positive | NR |
| Angeles-Angeles et al, 2009 | Positive | Positive | NR |
| Chen and Brainard, 2010 | Positive | NR | NR |
| Borschitz et al, 2010 | Positive | NR | Negative |
| Positive | NR | Positive | |
| Alzahrani et al, 2012 | Positive | Positive | Positive |
| Olson et al, 2013 | NR | NR | NR |
| Tunio et al, 2013 | NR | NR | Positive |
| Li et al, 2014 | Positive | Positive | NR |
| Davidson et al, 2017 | Positive | Positive | Positive |
| Murakami et al, 2018 | Positive | Positive | Positive |
| Cho et al, 2019 | NR | Positive | NR |
| Yang et al, 2019 | Positive | Positive | Positive |
| Tramontin et al, 2020 | NR | Positive | NR |
| Ren et al, 2020 | Positive | Positive | Positive |
| Rossi et al, 2020 | NR | Positive | NR |
| Uslar et al, 2020 | Positive | Positive | Positive |
| Yoon et al, 2020 | NR | NR | Negative |
| NR | NR | NR | |
| Stein et al, 2020 | Positive | Positive | NR |
| Wong et al, 2021 | NR | NR | NR |
| Warda et al, 2022 | Positive | Positive | Positive |
| Song et al, 2023 | Positive | Positive | Positive |
| Ahmadian et al, 2024 | NR | Positive | Negative |
| Present case | Positive | Positive | NR |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Thyroid Cancer Diagnosis and Treatment · Cancer Diagnosis and Treatment
INTRODUCTION
Differentiated thyroid cancers comprise the vast majority of thyroid malignancies, and the classic variant of papillary thyroid carcinoma is the most frequent type, with an indolent clinical course and good prognosis.^1^ Metastasis to distant organs occurs in <10% of patients, principally to lungs, bones, brain, and liver, but these metastases are a frequent cause of cancer-related mortality.^2^ Metastatic disease to the gastrointestinal tract is uncommon, accounting for <1% of all distant metastases.^3^ The pancreas is an extremely rare site for metastasis from thyroid cancer, with only 25 published case reports (involving 27 patients) in the English literature.^4-28^ Imaging alone cannot confirm the diagnosis; histopathologic analysis is critical for the definitive diagnosis of suspicious pancreatic lesions, especially in patients who have received previous treatment for other malignancies.^29^
We report the case of a patient who developed a pancreatic metastasis from a papillary thyroid carcinoma 11 years after undergoing total thyroidectomy and cervical lymphadenectomy for the primary thyroid cancer.
CASE REPORT
A 68-year-old female with a 3.8-cm classic variant papillary thyroid carcinoma in the left lobe underwent total thyroidectomy with bilateral cervical lymphadenectomy in June 2011. The lesion invaded the parathyroid tissue, the resection margins were disease-free, and 2 of 5 regional lymph nodes were metastatic (pT2N1aM0) (American Joint Committee on Cancer tumor-node-metastasis [TNM] system),^30^ configuring the disease as stage II. Postoperatively, the patient received 150 mCi of iodine-131 radioactive iodine. Whole-body iodine scintigraphy demonstrated no uptake following radioactive iodine ablation, and stimulated thyroglobulin was 2.5 ng/mL (reference value, <2 ng/mL). The patient was monitored regularly, was asymptomatic, and had thyroglobulin levels <2 ng/mL for 9 years.
From October 2020 to March 2022, the patient's thyroglobulin levels progressively increased, with levels ranging from 2.5 to 51.7 ng/mL, but a metastasis screening with whole-body iodine scintigraphy showed no uptake in November 2020. In August 2021, cervical ultrasound showed no recurrence. In March 2022, bone scintigraphy showed abnormal uptake in the seventh thoracic vertebra, abdominal computed tomography (CT) scan revealed a 2.9 × 2.3-cm lesion in the uncinate process of the pancreas, and cervical ultrasound showed a 0.9 × 0.4-cm nodule close to the trachea. The patient's serum level of carbohydrate antigen 19-9 was normal (36.3 U/mL; reference range, 0-37 U/mL), but her thyroglobulin level was elevated at 35.7 ng/mL.
The patient was referred for endoscopic ultrasound evaluation and biopsy of the pancreatic lesion. A well-circumscribed cystic lesion (4.0 × 2.8 cm) with a mural nodule (2.6 × 2.2 cm) in the lumen was identified in the uncinate process (Figure 1). A neoplastic thrombus was next to the lesion, partially obstructing the superior mesenteric vein. Endoscopic ultrasound-guided biopsy was performed via the transduodenal approach. The tissue samples were processed as cell blocks for histologic and immunohistochemistry evaluation.
(A) Endoscopic ultrasound showed a well-circumscribed cystic lesion measuring 4.0 × 2.8 cm in the uncinate process and a mural nodule (asterisk) measuring 2.6 × 2.2 cm. (B) A neoplastic thrombus (arrow) was partially obstructing the superior mesenteric vein. (C) The mural nodule was punctured by endoscopic ultrasound-guided biopsy (arrowhead).
Hematoxylin and eosin–stained sections demonstrated a hypercellular tumor consisting of cuboidal cells with irregular membrane, vacuolated cytoplasm, nuclear grooves, oval nuclei with granular chromatin, and no mitotic activity. The background was a papillary arrangement with complex randomly oriented papillae and fibrovascular cores, with pseudoinclusions in the pancreatic tissue. Immunohistochemical stains were positive for thyroglobulin, thyroid transcription factor 1, and cytokeratin 7. The histopathologic features and immunohistochemical profile confirmed a pancreatic metastasis from the classic variant papillary thyroid carcinoma (Figure 2). Our patient was not tested for the BRAF^V600E^ mutation.
(A) Histologic findings of pancreatic metastasis from papillary thyroid carcinoma demonstrated a tumor consisting of cuboidal cells with irregular membrane, vacuolated cytoplasm, nuclear grooves, oval nuclei with granular chromatin, and no mitotic activity. A papillary arrangement and fibrovascular cores with pseudoinclusions were detected in the pancreatic tissue (hematoxylin and eosin stain, magnification ×400). Neoplastic cells showed intense immunoreactivity for (B) thyroglobulin (magnification ×200), (C) thyroid transcription factor 1 (magnification ×100), and (D) cytokeratin 7 (magnification ×100). Thyroglobulin and cytokeratin 7 were positive for membranous and cytoplasmic immunoreactivity. Thyroid transcription factor 1 indicates nuclear positivity.
In July 2022, whole-body 18-fluorodeoxyglucose positron emission tomography/computed tomography (^18^F-FDG-PET/CT) showed intense uptake in the pancreatic lesion, in 1 retroperitoneal lymph node, and in the seventh thoracic vertebra. Abdominal CT showed a retroperitoneal lymph node (1.1 × 1.1 cm) and an increase in the size of the pancreatic lesion (4.9 × 3.5 × 2.8 cm) (Figure 3). The patient's thyroglobulin level was 35.7 ng/mL.
Contrast-enhanced axial abdominal computed tomography scan showed a 4.9 × 3.5 × 2.8-cm pancreatic cystic lesion in the uncinate process with a mural nodule in the cystic lumen (arrow).
Pancreatic resection was not considered because of multiorgan metastases. The patient was treated with 20 Gy of stereotactic body radiotherapy. Specifically for bone metastasis, the patient received a single dose of 18 Gy of external beam radiotherapy and denosumab 120 mg, 1 ampoule subcutaneously per month from September 2022 to September 2023. In September 2022, the patient received a second round of radioactive iodine ablation with 150 mCi of iodine-131. Whole-body iodine scintigraphy following radioactive iodine ablation showed no iodine-avid metastases. The patient's serum thyroglobulin level decreased to 23.2 ng/mL.
In March 2023, a repeat whole-body ^18^F-FDG-PET/CT revealed stability of the intense uptake in the pancreatic lesion, progression of the size and uptake in the retroperitoneal lymph node, and partial decrease of the uptake in the seventh thoracic vertebra. Abdominal CT showed the pancreatic lesion was stable in size and confirmed the enlargement of the retroperitoneal lymph node (3.0 × 2.0 cm). For the lymph node, the patient received a total of 35 Gy of stereotactic body radiotherapy.
In September 2023, abdominal CT showed several liver metastases, but the sizes of the pancreatic lesion (4.6 × 4.2 cm) and the retroperitoneal lymph node (3.1 × 3.0 cm) were stable. Until December 2023, despite the radiologic findings, the patient was asymptomatic and clinically doing very well.
However, in January 2024, the patient was hospitalized with abdominal pain, high fever, jaundice, and cholangitis as a result of progression of liver metastases and bile duct obstruction. Endoscopic retrograde cholangiopancreatography was performed for prosthesis placement and relief of the obstruction. Abdominal CT showed an increased number of liver lesions (the largest measured 3.0 cm), the pancreatic lesion had enlarged (5.3 × 4.5 cm), and the retroperitoneal lymph node was stable.
In February 2024, the patient's clinical condition notably worsened. Tyrosine kinase inhibitors could not be administered because of the patient's multiple tumor-related symptoms. Only supportive care could be offered. The patient's last thyroglobulin level was 139 ng/mL, and she died 23 months after the diagnosis of metastatic papillary thyroid carcinoma to the pancreas, which was 13 years after total thyroidectomy for the primary cancer.
DISCUSSION
Including our case, only 26 reports (involving 28 patients with a total of 29 lesions) of primary papillary thyroid carcinomas with pancreatic metastasis have been reported to date (Tables 1 and 2).^4-28^
Among the 28 patients, there was a preponderance of males (22 cases), and the median age of patients at diagnosis of pancreatic metastasis was 66 years (range, 39-84 years). Papillary thyroid carcinoma staging was available for 21 cases, 15 of which were stages I (n=7) and II (n=8) and 6 of which were stages III (n=4) and IVB (n=2). In most of the cases, papillary thyroid carcinoma was treated with thyroidectomy and radioactive iodine ablation. After surgery, locoregional recurrence occurred in 15 of 22 (68.2%) patients. Only 4 recurrent cases presented distant metastases prior to the pancreatic metastases, with the lungs affected in all 4 cases. Another case reported by Siddiqui et al involved a patient who presented with lung metastasis before the occurrence of pancreatic metastasis, but this case did not represent locoregional recurrence of thyroid cancer.^7^ With the exclusion of 5 synchronous lesions (ie, pancreatic metastasis detected at papillary thyroid carcinoma presentation), the median latency for pancreatic metastasis was 7 years, ranging from 1 to 15 years after papillary thyroid carcinoma treatment. The latency period was >5 years for 66.7% (14/21) of patients, with a median of 9 years.
Pancreatic metastases were detected by CT and/or PET scan in 17 cases. Both imaging modalities were used in 11 patients, with 4 patients also receiving magnetic resonance imaging (MRI). PET scan and CT scan were the single imaging procedure for 4 and 2 patients, respectively. Eight patients received CT and/or PET with MRI. Two patients received CT and ultrasound. The median size of the pancreatic metastases was 3 cm (range, 1.1-8.5 cm), and the median size of the pancreatic metastases for symptomatic and asymptomatic patients was the same (3 cm). The lesions of symptomatic patients were principally in the pancreatic head (7/13, 53.8%), while the lesions of asymptomatic patients were primarily in the body and tail (6/8, 75%). All pancreatic metastases were solitary lesions, except for a single patient with 2 lesions in the pancreatic head.^5^
Twenty metastases were solid with well-defined borders, and only 3 previously reported lesions presented a cystic area,^5,6,27^ as in our case. The uncinate process, head, and neck were involved in 15 cases, the body and/or tail in 12 cases, and the location was not reported for 1 case. Clinical features were reported for 21 patients. Of these patients, 13 were symptomatic: 8 had abdominal pain, and 2 of these patients had pancreatitis. Seventeen patients had other distant metastases at the diagnosis of pancreatic metastasis. Pulmonary metastases were the most common distant metastases (occurring in 12 cases), and bone metastases affected 8 patients, with 5 cases compromising vertebrae. Both lung and bone metastases were concurrent in 5 cases.
In 3 of 5 synchronous lesions, pancreatic metastases were detected before the primary papillary thyroid carcinoma.^8,19,20^ These lesions were located in the body or tail, and the leading complaint was abdominal pain. These 3 patients underwent surgery, and other distant metastases were found shortly before or after resection. After surgery, these patients were alive after a median follow-up of 8 months (range, 5-18 months).
After total thyroidectomy with or without radioactive iodine ablation, patients with papillary thyroid carcinoma may present with elevated thyroglobulin levels, revealing the presence of thyroid tissue in the body that indicates either residual tissue or locoregional/distant metastases.^31^ Metastatic lesions can be iodine-avid or not. A patient may have elevated thyroglobulin levels even in the presence of non-iodine–avid metastases. These lesions will not be identified by whole-body iodine scintigraphy because they do not demonstrate any iodine uptake.^32^
Because pancreatic imaging alone cannot ensure the detection of pancreatic metastasis, histopathologic evaluation of any pancreatic lesion in patients with previous malignancy is mandatory for definitive diagnosis.^29^ Samples for histopathology were obtained before surgery in 17 of the reported cases, 13 of them, including our case, by endoscopic ultrasound-guided tissue acquisition.^7,9,11,12,15-18,21-23,28^ Nine other patients underwent surgery with no previous biopsy.^8,10,14,19,20,24,26,27^
Metastatic thyroid cancer is immunohistochemically defined by a positive finding for thyroglobulin and thyroid transcription factor 1.^33^ Including our case, immunohistochemical studies were positive for thyroglobulin in 18 cases^5-11,14,16,17,19,20,22,24,26,27^ and for thyroid transcription factor 1 in 17 cases.^7,8,11,14-22,24,26-28^ Thirteen cases were positive for both markers.^7,8,11,14,16,17,19,20,22,24,26,27^ Information on both markers was not reported in 6 cases (Table 3).
The ideal therapeutic approach for treating pancreatic metastasis from papillary thyroid carcinoma is unknown. Surgical resection was the most frequent treatment in the reported cases (17 patients), including 8 pancreati-coduodenectomies,^4,5,7,13,18,21,24,26^ 8 distal pancreatecto-mies,^6,8,10,14,17,19,20,27^ and 1 enucleation.^10^ Ten patients with other concurrent metastases underwent surgery.^5-8,10,13,17,19,20,24^ Among these patients, 7 had pulmonary metastases, 5 patients had bone metastases, and 3 patients had concomitant lung and bone metastases.
In the presence of iodine-avid metastases, radioactive iodine ablation followed by thyroid-stimulating hormone suppression with thyroxine is the mainstay of metastatic disease treatment.^31^ Simões-Pereira et al investigated the differences in radioactive iodine avidity and outcome among specific histotypes of metastatic differentiated thyroid cancer and reported that iodine avidity in metastases occurred in 21.4% of patients with classic variant papillary thyroid carcinoma.^32^ The outcome of iodine-avid metastases from classic variant papillary thyroid carcinoma after radioactive iodine ablation was stable disease or partial/complete response in 55.6% of patients, with a progression-free survival of 32 months. For patients with classic variant papillary thyroid carcinoma, 5- and 10-year disease-specific survival was 69.2% and 53.3%, respectively. In their analysis of the outcomes of non-iodine–avid patients, Simões-Pereira et al found that 72.7% of patients with classic variant papillary thyroid carcinoma had evidence of progressive metastatic disease after radioactive iodine treatment.^32^ Our patient had a non-iodine–avid pancreatic metastasis, and whole-body iodine scintigraphy demonstrated no pancreatic uptake following a second round of radioactive iodine ablation with 150 mCi of iodine-131. Including our case, 5 patients in the reported cases were treated with radioactive iodine ablation,^10,20,22,25^ with a single patient receiving radioactive iodine ablation as the only treatment.^25^
When whole-body iodine scintigraphy shows no uptake in metastatic sites, tyrosine kinase inhibitors are an option for treatment of radioiodine-refractory metastases. In their systematic review and meta-analysis, Yu et al showed that the use of tyrosine kinase inhibitors significantly improved progression-free survival, and some tyrosine kinase inhibitors increased overall survival, although with a high incidence of side effects.^34^ A meta-analysis by Thomas et al that included 219 patients treated with sorafenib for metastatic thyroid cancer reported a partial response in 20.9%, stable disease in 58.3%, and progressive disease in 20.9% of patients with differentiated thyroid cancer.^35^ No study reported complete responses. In our review, 8 patients received tyrosine kinase inhibitors, either sorafenib or lenvatinib. Among the patients treated with sorafenib,^11,13,18^ 2 of 3 patients^13,18^ received the drug after surgery and had stable disease. The patient who received sorafenib as the sole treatment had progressive disease.^11^
Lenvatinib results have been more favorable. In the experience reported by Masaki et al with 42 patients, partial response was observed in 26 (62%) patients, stable disease in 10 (24%) patients, and progressive disease in 6 (14%) patients treated with lenvatinib.^36^ The overall survival of all treated patients was 51% at 3 years.^36^ In 4 cases reporting 5 pancreatic metastases from papillary thyroid carcinoma that were treated with lenvatinib,^19,23,24,26^ 2 patients who did not undergo resection had a partial response to treatment,^23^ and 3 patients who underwent resection did not develop recurrence or new pancreatic metastases.^19,24,26^ The presence of tumor-related symptoms prior to tyrosine kinase inhibitor use or symptom occurrence during treatment is an independent predictor of poor clinical benefit and poor survival.^37^ For this reason, our patient could not receive treatment with tyrosine kinase inhibitors.
In our review, the overall median follow-up for patients with pancreatic metastases from papillary thyroid carcinoma was 12 months. Patients who did not undergo surgery had a longer median follow-up period compared to patients who underwent surgery (20 months vs 9.5 months, respectively). Overall mortality was 31.8%, and the mortality rate was similar for patients who underwent surgery vs patients who did not undergo surgery (33.3% vs 28.6%, respectively). These findings must be interpreted cautiously because we only evaluated case reports, most of which involved a single patient, and several case reports were missing data.
Some mutations occur frequently in papillary thyroid carcinoma. BRAF^V600E^ is the most common oncogene in papillary thyroid carcinoma, with an average prevalence between 25% to 89.2%.^38,39^ Compared with wild-type BRAF, the BRAF^V600E^ mutation is associated with more aggressive features, including extrathyroidal invasion, lymph node metastasis, advanced TNM stage, recurrence, and decreased survival.^39^ Although the association between the BRAF^V600E^ mutation and distant metastases is still controversial,^38,39^ positive BRAF^V600E^ metastases are frequently non-iodine–avid lesions with higher ^18^F-FDG avidity.^40,41^ In our review, the status of the BRAF^V600E^ mutation was evaluated in 13 cases, and the mutation was present in 10 (76.9%) patients (Table 3). In the patients presenting with the mutation, papillary thyroid carcinoma stage was I (4) and II (4) for 8 cases, and locoregional recurrence occurred in 6/10 (60%) cases. The median size of pancreatic metastases was 3 cm, 5 of 8 (62.5%) cases were symptomatic, and 7/10 (70%) cases had concurrent metastases. Mortality was 30% (3/10). Because the BRAF^V600E^ mutation was analyzed in fewer than half the cases in our review, we cannot draw definitive conclusions about the importance of the mutation on the prognosis of these patients.
CONCLUSION
Our patient developed a pancreatic metastasis from a classic variant papillary thyroid carcinoma more than a decade after thyroidectomy. Although rare, pancreatic metastasis must be considered and requires imaging procedures other than whole-body iodine scintigraphy during regular follow-up of patients with prior malignancies. If a lesion is detected, histopathologic evaluation is mandatory. Because best management for these cases has not yet been defined, radioactive iodine ablation should be considered for iodine-avid lesions, and surgery or tyrosine kinase inhibitor therapy are promising for non-iodine–avid metastases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H, Ferlay J, Siegel RL, Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. doi: 10.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Durante C, Haddy N, Baudin E, Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: benefits and limits of radioiodine therapy. J Clin Endocrinol Metab. 2006;91(8):2892-2899. doi: 10.1210/jc.2005-283816684830 · doi ↗ · pubmed ↗
- 3Klubo-Gwiezdzinska J, Morowitz D, Van Nostrand D, Metastases of well-differentiated thyroid cancer to the gastrointestinal system. Thyroid. 2010;20(4):381-387. doi: 10.1089/thy.2009.028020210670 · doi ↗ · pubmed ↗
- 4Sugimura H, Tamura S, Kodama T, Kakitsubata Y, Asada K, Watanabe K. Metastatic pancreas cancer from the thyroid; clinical imaging mimicking non functioning islet cell tumor. Radiat Med. 1991;9(5):167-169.1771245 · pubmed ↗
- 5Jobran R, Baloch ZW, Aviles V, Rosato EF, Schwartz S, Li Volsi VA. Tall cell papillary carcinoma of the thyroid: metastatic to the pancreas. Thyroid. 2000;10(2):185-187. doi: 10.1089/thy.2000.10.18510718557 · doi ↗ · pubmed ↗
- 6Meyer A, Behrend M. Is pancreatic resection justified for metastasis of papillary thyroid cancer? Anticancer Res. 2006;26(3B):2269-2273.16821600 · pubmed ↗
- 7Siddiqui AA, Olansky L, Sawh RN, Tierney WM. Pancreatic metastasis of tall cell variant of papillary thyroid carcinoma: diagnosis by endoscopic ultrasound-guided fine needle aspiration. JOP. 2006;7(4):417-422.16832140 · pubmed ↗
- 8Angeles-Angeles A, Chable-Montero F, Martinez-Benitez B, Albores-Saavedra J. Unusual metastases of papillary thyroid carcinoma: report of 2 cases. Ann Diagn Pathol. 2009;13(3):189-196. doi: 10.1016/j.anndiagpath.2008.02.01019433299 · doi ↗ · pubmed ↗