When Teratoma Masquerades: A Rare Case of Intrapleural Mature Cystic Teratoma Mimicking Tuberculous Empyema
Nik Nuratiqah Nik Abeed, Ng Boon Hau, Nor Safiqah Sharil, Andrea Ban Yu Lin, Marfua'h Nik Ezzamudin, Hairulfaizi Haron

TL;DR
A rare case of a mature cystic teratoma in the pleura was mistaken for a recurring tuberculous empyema, highlighting the importance of accurate diagnosis.
Contribution
This paper presents a rare clinical case of intrapleural mature cystic teratoma mimicking tuberculous empyema.
Findings
The patient's pleural effusion was initially suspected to be tuberculous but was later diagnosed as a mature cystic teratoma.
Histopathological analysis confirmed the diagnosis after imaging and initial treatments failed to resolve the condition.
The case emphasizes the diagnostic challenges posed by rare teratomas masquerading as more common diseases.
Abstract
Teratomas are germ cell tumours generally gonadal in origin and very rare, arising from extra gonadal tissue. The most common extragonadal teratomas are mediastinal, and the majority are benign. We report a case of a 49‐year‐old lady with recurrent right complex pleural effusion occurring a month after the completion of treatment for tuberculous empyema. Imaging from ultrasound of the thorax and contrasted enhanced computed tomography (CECT) thorax revealed multiseptated and loculated effusion in the thorax without any mediastinal and lung involvement. Surprisingly, pleural fluids were negative for tuberculosis. Despite chest drainage and initial treatment for bacterial empyema without improvement, she underwent video assisted thoracoscopy and decortication of the right pleura, and histopathological analysis revealed a mature cystic teratoma. She was discharged in good health and under…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
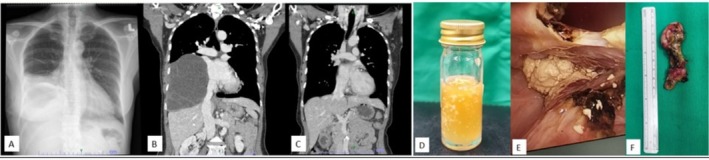 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTeratomas and Epidermoid Cysts · Testicular diseases and treatments · Myasthenia Gravis and Thymoma
Introduction
1
A benign cystic mature teratoma originating from the pleural space without mediastinal involvement is extremely rare. Most teratomas grow slowly, with patients typically remaining asymptomatic. However, in this case, the presence of a concurrent tuberculous infection exacerbated symptoms, prompting the patient to seek medical attention. Tuberculous empyema rarely recurs within a short period unless there is medication non‐compliance or misdiagnosis. This case underscores the importance of considering alternative diagnoses in cases of recurrent empyema or complex pleural effusion, especially when clinical responses are poor and no obvious primary lesion is identified.
Case Report
2
A 49‐year‐old woman, diagnosed with right tuberculous empyema, presented with fever, shortness of breath and a 2‐kg weight loss over 3 weeks. Clinically, she had right pleural effusion. A chest radiograph and bedside thoracic ultrasound confirmed loculated right pleural effusion. Blood tests showed leukocytosis with normal renal and liver function. A right chest drain was inserted, showing purulent exudative fluid. Mycobacterium tuberculosis Polymerase Chain Reaction (PCR) was positive, although results were negative for acid‐fast bacilli (AFB), mycobacterial culture and cytology.
Due to loculated empyema, she received fibrinolytic therapy with low‐dose intrapleural alteplase of 5 mg; however, this was complicated by bleeding at the chest drain site, preventing further cycles of fibrinolysis. She was started on a nine‐month course of anti‐tuberculous treatment with Akurit‐4 according to the body weight and showed clinical and radiological improvement by the end of therapy.
One month post completed treatment, she developed recurrent complex right pleural effusion. Imaging via thoracic ultrasound and contrast‐enhanced computed tomography (CECT) revealed a recurrent, multiseptated, loculated right pleural effusion. A chest drain was reinserted, and pleural fluid analysis showed straw‐coloured, exudative fluid with a high lactate dehydrogenase (LDH) level of 469 U/L, though bacterial culture and tuberculosis including Xpert Mycobacterium/Rifampicin (MTB/RIF) tests were negative. Blood parameters indicated an inflammatory response, with elevated white blood cells (13 × 10^9^/L) and C‐reactive protein (5.41 g/dL), but blood cultures were negative.
She was treated for bacterial empyema with a 4‐week course of piperacillin‐tazobactam, but her condition did not improve. The patient was then referred to a cardiothoracic surgeon for decortication. During video‐assisted thoracoscopic surgery (VATS), surgeons found multiloculated thickened pleural cortex adherent to the pericardium and diaphragm, with Ghon complexes and 1 L of proteinaceous fluid (Figure 1) surprisingly, pleural fluid and tissue tested negative for tuberculosis, and pleural tissue histopathological examination showed macroscopically multiloculated cysts containing yellowish pasty contents. The cyst is composed of mature ectodermal, mesodermal and endodermal components such as keratinized stratified squamous epithelium, adnexa sweat glands, sheets of adipose tissue, smooth muscle bundles, gastric foveolar epithelium, ciliated respiratory and tubal epithelium, renal tubular epithelium and endocervical epithelium revealed mature cystic teratoma.
(A) Chest radiograph showed right moderate pleural effusion; (B) CECT coronal view showed right pleural effusion; (C) CECT surveillance post decortication showed resolving right pleural effusion; (D) Pleural fluid showed proteinaceous yellowish fluid; (E) Cheesy mass embedded in parietal pleural via video assisted thoracoscopy; (F) Pleural tissue with the tumour 8 cm length.
Postoperatively, the patient was discharged in good health and placed under annual surveillance with CECT thorax. After 3 years of follow‐up, she remains asymptomatic and radiologically stable.
Discussion
3
Mature cystic teratoma is a benign tumour originated from gonads. Tumour can occur in extragonadal regions, especially the mediastinum. However, intrapleural mature cystic teratoma without mediastinal involvement is extremely rare.
The patients are often asymptomatic and the tumour is discovered incidentally on chest radiographs obtained for other reasons. To our knowledge, this is the third case reported. The first case reported a young lady with acute chest pain and shortness of breath; and the CT showed a complex cystic mass within the left pleural cavity. The patient did thoracotomy with removal of the cystic mass, with confirmed mature cystic teratoma [1]. The second case was empirically treated as bacterial empyema given fibrinolytic therapy but poor response; hence, it did decortication, with intraoperative revealed hair‐like structures in the purulent fluid [2]. Otherwise, Katoto et al. reviewed 63 cases of mature teratoma presented with pleural effusion, with the origin of the teratoma being mediastinal [3].
Similar to other cases reported, the majority of the cases were misdiagnosed as tuberculous or bacterial empyema and remaining symptomatic warranted further investigation. This case is noteworthy in terms of atypical presentation, intrapleural in origin without mediastinal involvement and its misleading presentation due to the concurrent tuberculous empyema. The treatment of tuberculous empyema with fibrinolytic therapy and anti‐tuberculous therapy without recovery leading to decortication is the best option.
Author Contributions
Nik Nuratiqah Nik Abeed as author constructing the case. Ng Boon Hau and Nor Safiqah Sharil contribute to discussion alignment. Andrea Ban Yu Lin is involved in the idea of the discussion. Marfu'ah Nik Ezzamudin contributes to writing a follow‐up care and continuation of care as an oncologist. Hairulfaizi Haron contributes to providing the picture during surgical intervention.
Ethics Statement
The authors declare that written informed consent was obtained for the publication of this manuscript and accompanying images using the consent form provided by the Journal.
Conflicts of Interest
A.B.Y.L. is an Editorial Board member of Respirology Case Reports and a co‐author of this article. She was excluded from all editorial decision‐making related to the acceptance of this article for publication. The other authors have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Goizueta , R. Almadi , and J. Meharg , “Intrapleural Benign Mature Cystic Teratoma,” American Journal of Respiratory and Critical Care Medicine 193 (2016): A 3356.
- 2K. A. Jiun and T. Y. Sim , “A Rare Case of Intrapleural Teratoma–Mimicking as Empyema Thoracis,” Malaysian Journal of Medicine and Health Sciences 20, no. 1 (2024): 398–400.
- 3P. D. Katoto and L. N. Byamungu , “Mediastinal Cystic Teratoma Misdiagnosed as Pleural Tuberculosis: A Case Report and Review of 53 Cases Revealed by Pleural Effusion,” Clinical Case Reports 9, no. 6 (2021): e 04139.34136228 10.1002/ccr 3.4139 PMC 8190687 · doi ↗ · pubmed ↗