Incidence of and risk factors for mortality in children with mushroom poisoning
Jie Cheng, Ya Liu, Shaojun Li, Kaibin Pu, Junming Huo, Liping Tan

TL;DR
This study finds that children with mushroom poisoning have a 24% mortality rate, and a higher pSOFA score is linked to increased risk of death.
Contribution
The study identifies the pSOFA score as a novel prognostic indicator for mortality in children with mushroom poisoning.
Findings
The mortality rate of children with mushroom poisoning was 23.88%.
A pSOFA score ≥ 2 is associated with significantly increased mortality risk.
The pSOFA score showed strong predictive value with an AUC of 0.84.
Abstract
We aimed to evaluate the incidence of and risk factors for mortality in children with mushroom poisoning. Sixty-seven children with mushroom poisoning who were hospitalized at the Children’s Hospital of Chongqing Medical University were retrospectively enrolled. The clinical characteristics of the children in the surviving and non-surviving groups were compared. Variables with a P value < 0.1 in the univariate logistic regression analysis were included in the multivariate logistic regression analysis. A receiver operating characteristic (ROC) curve was generated to determine the optimal cutoff point. The mortality rate of children with mushroom poisoning was 23.88% (16/67), and the incidence of death during hospitalization was 35.02 per 1,000 person-days. The median pediatric sequential organ failure assessment (pSOFA) score was 1.00 (interquartile range [IQR] 0.00–3.00). Logistic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
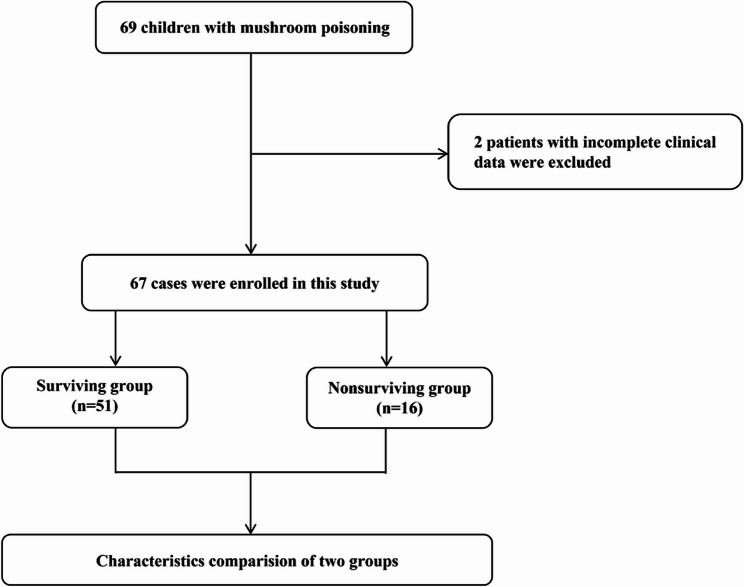 Figure 1
Figure 1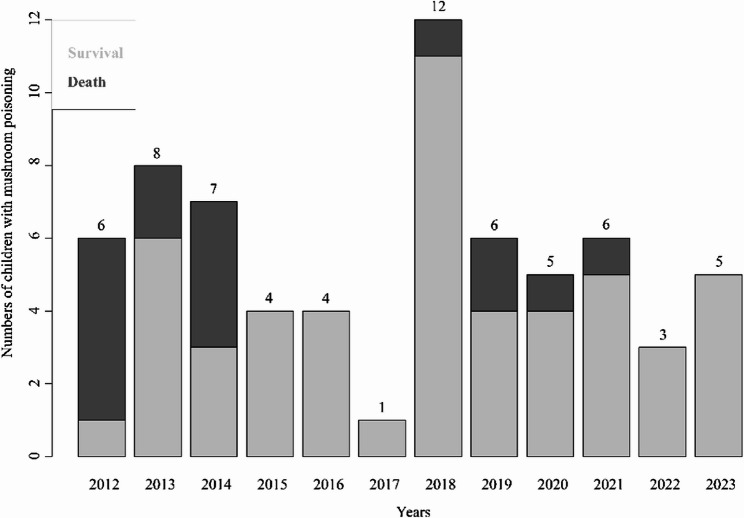 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoisoning and overdose treatments · Drug-Induced Hepatotoxicity and Protection · Silymarin and Mushroom Poisoning
Introduction
Wild mushroom is a widely eaten food worldwide because of its savory flavor [1], and it is estimated that approximately 100 people die from mushroom poisoning every year worldwide [2]. By the end of 2022, more than 500 poisonous mushrooms that have been discovered in China [3]. Mushroom poisoning mostly occurs in Southwest China in the summer and autumn and remains one of China’s most serious food safety problems [3]. Mushroom poisoning may induce damage to multiple organs [2]. From 2010 to 2022, the overall mortality rate of mushroom poisoning ranged from 2.10 to 7.85% [1, 3, 4]. With the increasing education on mushroom poisoning, the focus on identifying mushroom species, and the improvements in treatments, the mortality of mushroom poisoning significantly decreased between 2010 and 2022 [1, 3]. Mushroom poisoning is still an urgent food safety issue in China [3]. The type of mushroom a patient with mushroom poisoning has consumed is not always known [5]; however, knowing the specific type of mushroom a patient consumes is crucial for diagnosis and treatment. However, few studies have reported on mushroom poisoning in children, and the development of an appropriate prognostic indicator is expected to help clinicians evaluate the prognosis. The pediatric sequential organ failure assessment (pSOFA) scoring system [6] consists of the evaluation of five systems (respiratory, coagulation, cardiovascular, neurologic, and renal). These child-specific parameters may help us accurately identify the risk of poisoning-related organ dysfunction and are in line with the pathological characteristics of multi-organ damage in children with mushroom poisoning [7–10].
In this study, we investigated the incidence of death and explored risk factors for mortality in children with mushroom poisoning.
Methods
Study designs and patients
This retrospective, observational, cohort study was conducted at the Children’s Hospital of Chongqing Medical University in Chongqing, a National Regional Children’s Medical Center, and National Clinical Research Center for Child Health and Disorders in China (website: https://www.chcmu.com/chcmuy/yygk/yyjj.htm). From January 2012 to December 2023, hospitalized children with mushroom poisoning were enrolled in our study. The inclusion criteria were as follows: (i) hospitalized children; (ii) children with mushroom poisoning. Children with incomplete clinical data were excluded. This study was approved by the Ethics Committee of Children’s Hospital of Chongqing Medical University. File No. 2023 (538). Informed consent was waived by the Ethics Committee of Children’s Hospital of Chongqing Medical University. The relevant guidelines and regulations performed all methods.
Data collection and definitions
We retrospectively collected demographic data (age, sex), admission patterns, medical records, laboratory tests, therapies, pSOFA scores, and outcomes. The pSFOA score was collected within 48 h of admission. Mushroom poisoning was diagnosed according to the description of the mushroom consumed and the symptoms and clinical findings of the patients [5]. All children who meet the indications for artificial liver treatment will start artificial liver treatment on the day of admission.
Statistical analysis
Continuous and categorical variables are medians (quartiles) and frequencies (%). Categorical variables were compared with the χ^2^ test or Fisher’s exact test, and continuous variables were compared with Student’s t test or the Mann − Whitney U test. Variables with a P value < 0.1 in the univariate logistic regression analysis were included in the multivariate logistic regression analysis. A receiver operating characteristic (ROC) curve was generated to determine the optimal cutoff point of the pSOFA score for predicting mortality in children with mushroom poisoning. An AUC between 0.7 and 0.9 indicated moderate predictive ability [11, 12]. All the statistical analyses were conducted in R software (version 4.3.0). A P value ≤ 0.05 was considered to indicate statistical significance.
Results
Study population
From January 2012 to December 2023, 69 children with mushroom poisoning were admitted to the Children’s Hospital of Chongqing Medical University. Two patients with incomplete clinical data were excluded. Finally, sixty-seven children with mushroom poisoning were enrolled in our study (Fig. 1).
Fig. 1. Flow chart of the population
Clinical characteristics of 67 children with mushroom poisoning
The percentage of patients with mushroom poisoning did not significantly change from 2012 to 2023 (Fig. 2). The median age was 7.92 (interquartile range [IQR] 5.67–9.83) years, and 55.22% (37/67) of the patients were male. The median time from consuming mushrooms to admission was 3.00 (IQR 0.33–4.00) days, and the median length of stay was 3.75 (IQR 2.19–10.92) days. Approximately half (30/67, 44.78%) of the patients were admitted from the emergency department, and nearly one-third (22/67, 32.84%) of the patients were transferred to the wards of our hospital from other hospitals. Most patients experienced abdominal pain (35/67, 52.24%), vomiting or diarrhea (63/67, 94.03%), and more than 10% of patients experienced a coma (10/67, 14.93%) or had convulsions (9/67, 13.43%). More than 20% (16/67, 23.88%) of patients needed invasive mechanical ventilation, and approximately two-thirds (43/67, 64.18%) of patients received artificial liver support system therapy. The median pSOFA score was 1.00 (IQR 0.00–3.00). The overall mortality was 23.88% (16/67), and the incidence of death during hospitalization was 35.02 per 1,000 person-days. All the details are shown in Table 1.
Fig. 2. Number of children with mushroom poisoning in different years
Table 1. Characteristics of the 67 children with mushroom poisoningCharacteristicsTotal (n = 67)Demographic data Age (years) (median, IQR)7.92 (5.67–9.83) Sex (male) (n, %)37 (55.22%)Patterns of admission Admitted from the emergency department (n, %)30 (44.78%) Transferred to wards from other hospitals (n, %)22 (32.84%)Clinical manifestations Vomiting or diarrhea63 (94.03%) Abdomen pain35 (52.24%) Coma (n, %)10 (14.93%) Convulsions (n, %)9 (13.43%)Laboratory tests Coagulation function PT (s) (median, IQR)13.30 (11.70−56.75) APTT (s) (median, IQR)29.50 (26.00−56.30) Fibrinogen (g/L) (median, IQR)1.75 (1.07–2.30) Liver function TBIL (µmol/L) (median, IQR)18.00 (6.85–60.55) Albumin (g/L) (median, IQR)41.30 (31.65–45.60) ALT (U/L) (median, IQR)363.10 (25.85−4332.50) AST (U/L) (median, IQR)253.00 (29.80−2070.75) Kidney function BUN (mmol/L) (median, IQR)5.09 (3.77–6.51) Creatinine (µmol/L) (median, IQR)39.00 (31.25–50.10)Advanced life support Requiring for invasive mechanical ventilation (n, %)16 (23.88%) With artificial liver support system (n, %)43 (64.18%) The time from consuming the mushroom to admission (days)3.00 (0.33−4.00) Length of stay (days) (median, IQR)3.75 (2.19–10.92) pSOFA score (median, IQR)1.00 (0.00–3.00) Mortality (n, %)16 (23.88%)
Comparisons of the clinical characteristics between the surviving and non-surviving groups of 67 children with mushroom poisoning
The characteristics of the two groups are shown in Table 2. Patients in the survival group were much older than those in the non-survival group (8.25 years (IQR 6.58–10.92 years) vs. 5.63 years (IQR 2.86–7.27 years), P = 0.001). There were no significant differences between the survival and the non-survival groups for the patterns of admission, and there were more deceased patients who had experienced a coma than those who survived (37.50% vs. 7.84%, P = 0.009). Compared with the survival patients, the non-survival patients had remarkably higher levels of prothrombin time (PT), activated partial thromboplastin time (APTT), total bilirubin (TBIL), alanine transaminase (ALT), and aspartate aminotransferase (AST), and lower fibrinogen and albumin levels. (P < 0.001). The blood urea nitrogen (BUN) and creatinine levels were not different between the two groups. The non-surviving group had more patients who needed invasive mechanical ventilation and artificial liver support systems (68.75% vs. 9.80%, P < 0.001; 87.50% vs. 56.86%, P = 0.053, respectively). The amount of time between consuming mushroom and admission to the hospital was much longer in the non-surviving group than in the surviving group (4.00 days (IQR 3.00–5.00 days) vs. 2.00 days (IQR 0.31–3.00 days), P = 0.002). However, the length of stay differed between the non-surviving group and the surviving group (2.50 days (IQR 1.24–4.50 days) vs. 5.42 days (IQR 2.32–13.19 days), respectively, P = 0.044). The patients who died had notably higher pSOFA scores than those who survived (3.50 (IQR 2.00–6.00) vs. 0.00 (IQR 0.00–2.00), P < 0.001).
Table 2. Comparisons of the clinical characteristics between the surviving and non-surviving groups of 67 children with mushroom poisoningCharacteristicsSurvival (n = 51)Non-survival (n = 16)P-valueDemographic data Age (years) (median, IQR)8.25 (6.58–10.92)5.63 (2.86–7.27)0.001* Sex (male) (n, %)26 (50.98%)11 (68.75%)0.338Patterns of admission Admitted from the emergency department (n, %)22 (43.14%)8 (50.00%)0.847 Transferred to wards from other hospitals (n, %)16 (31.37%)6 (37.50%)0.881Clinical manifestations Vomiting or diarrhea48 (94.12%)15 (93.75%)1.000 Abdomen pain28 (54.90%)7 (43.75%)0.622 Coma (n, %)4 (7.84%)6 (37.50%)0.009* Convulsions (n, %)6 (11.76%)3 (18.75%)0.437Laboratory tests Coagulation function PT (s) (median, IQR)12.20 (11.45−16.00)141.70 (55.35–180.00)< 0.001* APTT (s) (median, IQR)28.40 (25.35–30.85)88.80 (56.50−119.60)< 0.001* Fibrinogen (g/L) (median, IQR)1.95 (1.54–2.43)0.77 (0.62–1.04)< 0.001* Liver function TBIL (µmol/L) (median, IQR)12.90 (6.20–30.40)79.50 (64.35–95.18)< 0.001* Albumin (g/L) (median, IQR)43.00 (39.10−46.55)29.30 (25.15–32.90)< 0.001* ALT (U/L) (median, IQR)47.00 (24.55−2071.10)5408.85 (2781.23−7562.73)< 0.001* AST (U/L) (median, IQR)39.20 (27.90−677.80)2130.45 (1537.40−7605.50)< 0.001* Kidney function BUN (mmol/L) (median, IQR)5.27 (4.09–6.39)4.55 (3.48–6.69)0.374 Creatinine (µmol/L) (median, IQR)39.30 (33.45–50.10)34.45 (29.38–48.85)0.293Advanced life support Requiring for invasive mechanical ventilation (n, %)5 (9.80%)11 (68.75%)< 0.001* With artificial liver support system (n, %)29 (56.86%)14 (87.50%)0.053 The time from consuming the mushroom to admission (days)2.00 (0.31−3.00)4.00 (3.00–5.00)0.002* Length of stay (days) (median, IQR)5.42 (2.32–13.19)2.50 (1.24–4.50)0.044* pSOFA score (median, IQR)0.00 (0.00–2.00)3.50 (2.00–6.00)< 0.001******With statistical significance, P < 0.05
Risk factors for mortality in 67 children with mushroom poisoning
According to the univariate logistic regression analysis, the serum albumin concentration, age, and fibrinogen level were protective factors against mortality in children with mushroom poisoning (P < 0.05). Furthermore, there was a positive correlation between mortality and a longer time from consuming the mushroom to admission, the need for invasive mechanical ventilation, the use of an artificial liver support system, coma, a higher TBIL, a higher PT, a higher APTT, a higher ALT level, a higher AST level and a higher pSOFA score (P < 0.05). According to the multivariate regression analysis, only the pSOFA score was independently associated with mortality (odds ratio [OR] 4.92, 95% confidence interval [CI] 1.59–62.21; P = 0.040). All the details are shown in Table 3.
Table 3. Logistic regression analysis of risk factors for mortality among 67 children with mushroom poisoningVariablesUnivariate analysisMultivariate analysisOR95% CI P OR95% CI P pSOFA1.891.39–2.79< 0.0014.921.59–62.210.040Requiring for invasive mechanical ventilation20.245.35–91.68< 0.001Coma7.051.71–21.320.008With artificial liver support system5.311.30–36.090.039The time from consuming the mushroom to admission (days)1.541.14–2.180.008APTT (s)1.041.02–1.07< 0.001TBIL (µmol/L)1.031.02–1.05< 0.001PT (s)1.021.01–1.04< 0.001ALT (U/L)1.000031.00001–1.00005< 0.001AST (U/L)1.000021.00001–1.00004< 0.001Albumin (g/L)0.810.72–0.89< 0.001Age (years)0.730.58–0.890.004Fibrinogen (g/L)0.050.01–0.19< 0.001*****With statistical significance, P < 0.05
The prognostic value of the pSOFA score for predicting mortality in 67 children with mushroom poisoning
The optimal cutoff point of the pSOFA score for the prediction of mortality was 2.00, with an area under the curve (AUC) of 0.84 (95% CI 0.71–0.88, 87.50% sensitivity and 70.59% specificity, P < 0.001), which indicates moderate predictive efficacy [13]. The details of the ROC curve are shown in Supplemental Fig. 1. The Kaplan–Meier survival curve showed that patients with a pSOFA score < 2 had a significantly greater survival probability than patients with a pSOFA score ≥ 2 during hospitalization. The details are presented in Supplemental Fig. 2.
Discussion
Mushroom poisoning is one of China’s most serious food safety problems [3]. However, few studies have reported on mushroom poisoning in children, and identifying a good and convenient prognostic tool for predicting mortality due to mushroom poisoning is urgently needed. In this study, we investigated the gaps in the knowledge regarding mushroom poisoning in children. Mushroom poisoning mostly occurs in Southwest China [3]. Our study was conducted at the Children’s Hospital of Chongqing Medical University, a National Clinical Research Center for Child Health and Disorders, which treats patients throughout Southwest China (website: https://www.chcmu.com/chcmuy/yygk/yyjj.htm), and this may strengthen the universality of the results of our study.
Only 67 children with mushroom poisoning were enrolled in our study from 2012 to July 2023; the mortality rate reached 23.88% (16/67), and the incidence of death during hospitalization was 35.02 per 1,000 person-days. In recent decades, the reported overall mortality of mushroom poisoning in China has ranged from 2.10 to 7.85% [1, 3, 4], much lower than our study’s mortality. This might indicate that children with mushroom poisoning have more serious adverse outcomes than adult patients. Furthermore, as a National Regional Children’s Medical Center and National Clinical Medicine Research Center (website: https://www.chcmu.com/chcmuy/yygk/yyjj.htm), our center treats critically ill children in the region. More than 30% (22/67, 32.85%) of the cases included in this study were difficult/critically ill children transferred from other hospitals. This explains, to a certain extent, the difference in mortality rates between this study and previous studies of mushroom poisoning patients. On the other hand, the inclusion of such cases not only reflects the core role of our center in complex case management, but also ensures that the research cohort is widely representative in terms of disease severity, providing important support for the universality of the conclusions.
Our study revealed that the pSOFA score was positively associated with mortality in children with mushroom poisoning. The possible explanations are as follows. The pSOFA scoring system is used to evaluate the severity of organ dysfunction in sepsis patients [6] and may also serve as a convenient prognostic tool [14]. Wild mushrooms may be toxic because they induce cellular death in the human body’s cells [15], and the intestines, liver, and kidneys are affected the most [16]. Liver function deterioration always occurs after the gastrointestinal symptoms [17]. Apoptotic hepatocytes cannot remove toxic metabolites, and these apoptotic hepatocytes also cannot synthesize coagulation factors, complement, and lipoproteins [18]. As a result, multiple organ dysfunction syndrome may occur, which can be diagnosed using the pSOFA score. In this study, we also found that children with mushroom poisoning who had a pSOFA score ≥ 2 had a significantly increased risk of mortality.
In this study, most children with mushroom poisoning had gastrointestinal symptoms (abdomen pain, vomiting, or diarrhea), which was in accordance with the findings of Sabeel et al. [17]. Compared with surviving patients, patients who died had lower levels of albumin and fibrinogen, and higher levels of TBIL, ALT, AST, PT, and APTT. A possible explanation is as follows. Liver failure always occurs in patients with critical mushroom poisoning and may present as abnormalities in liver function or coagulation function. Hepatocytes that fail to perform their function may induce multiple organ dysfunction syndrome [18], which indicates poor outcomes. Furthermore, patients in the non-surviving group had a longer time from consuming mushrooms to admission than did surviving patients, which may suggest that timely treatment improves the health of children with mushroom poisoning. Mushroom poisoning can lead to acute liver failure [8], and artificial liver support therapy is critical for children with mushroom poisoning [18]. Yang et al. [19] stated that after continuous artificial liver treatment, liver function-related indicators (e.g., ALT and TBIL) of children with mushroom poisoning have significantly improved, and receiving it may reduce the risk of death. Regarding the timing of treatment, all children in our study who met the indications for artificial liver treatment received artificial liver treatment on the day of admission. The “Chinese Clinical Guideline for the Diagnosis and Treatment of Mushroom Poisoning” [20] recommends that patients with fatal mushroom poisoning should undergo blood purification treatment as soon as possible. Therefore, once a child has mushroom poisoning, artificial liver support treatment should be carried out as soon as possible to grasp the timing of treatment, which is extremely important for improving the prognosis of children and reducing mortality.
There were several limitations in our study. First, this was a single-center, retrospective study with a small sample size, and a multi-center, prospective study with a large sample size was expected. Second, another limitation of our study was that different wild mushroom species may induce different adverse outcomes [3], and our study did not discuss the difficulties in reminiscing or identifying the specific types of eaten mushrooms. However, this study may promote education regarding the safety of consuming mushrooms and improve the screening techniques for poisonous substances. Third, given the significant differences in clinical symptoms and severity among different mushroom poisoning patients, we believe that the toxicity levels vary significantly among different patients. However, in clinical treatment, clinicians focus on mushroom type, intake, symptom changes, and dynamic organ damage indicators and do not perform toxicity level testing. Finally, we did not discuss the influence of specific types of artificial liver support system therapy on prognosis. The advantages and disadvantages of different artificial liver support systems remain unknown, and there is no uniform artificial liver support system therapy available for children with mushroom poisoning [18]. Additional studies on artificial liver support systems for mushroom poisoning are expected.
Conclusions
In this study, the incidence of death among children with mushroom poisoning was retrospectively evaluated. The pSOFA score may serve as a good prognostic indicator in children with mushroom poisoning, and children with a pSOFA score ≥ 2 had a significantly increased risk of mortality.
Supplementary Information
Supplementary Material 1: Supplemental Figure 1. ROC curve of the ability of the pSOFA score to predict mortality in 67 children with mushroom poisoning. Supplemental Figure 2. Comparison of the survival probability of patients with different pSOFA scores.
The reference list from the paper itself. Each links out to its DOI / PubMed record.