The Early Experience of Synchrony in Ultra-Hypofractionation for Prostate Cancer: A Case Series
Piyapasara Toapichattrakul, Pooriwat Muangwong, Anupong Kongsa, Wannapha Nobnop, Anirut Watcharawipha, Ekkasit Tharavichitkul

TL;DR
This study shows that ultra-hypofractionated radiotherapy for prostate cancer using real-time tracking is technically feasible and has minimal toxicity.
Contribution
Demonstrates early clinical and technical outcomes of ultra-hypofractionated prostate radiotherapy using Synchrony real-time tracking.
Findings
PSA levels declined rapidly with a mean rate of -4.27 ng/mL/month.
Synchrony tracking achieved submillimeter accuracy with a median deviation of 1.04 mm.
Treatment duration increased by 13.9% due to automatic pauses for motion correction.
Abstract
Ultra-hypofractionated radiotherapy has emerged as an effective treatment for localized prostate cancer, offering comparable oncologic outcomes to conventional fractionation while significantly reducing treatment duration. However, the delivery of high doses per fraction demands exceptional precision to minimize toxicity risks, particularly in the context of intrafractional prostate motion. Real-time tracking systems, such as Synchrony (Accuray, Sunnyvale, CA, USA), aim to address this challenge by continuously monitoring and correcting for target displacement during beam delivery. This study evaluates the technical feasibility and early clinical outcomes of ultra-hypofractionated radiotherapy (36.25 Gy in five fractions) delivered with Synchrony real-time tracking, with specific analysis of prostate specific antigen (PSA) kinetics, treatment delivery parameters, and safety. Five…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
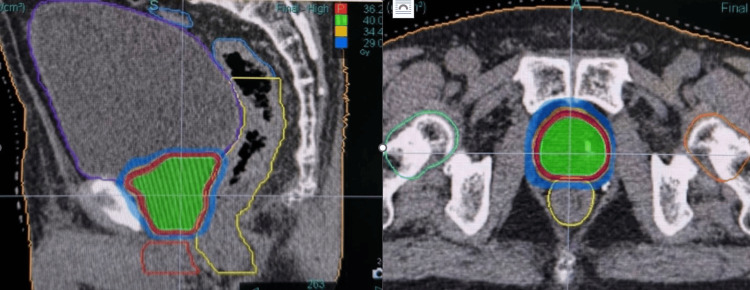 Figure 1
Figure 1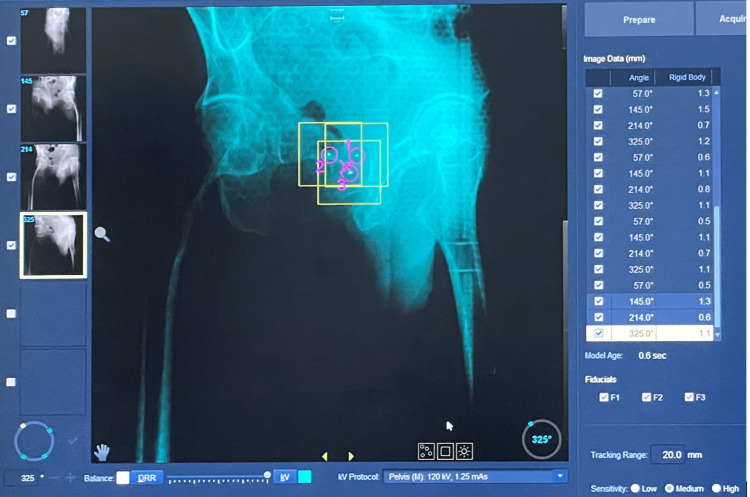 Figure 2
Figure 2| Structure | Dose Constraint | |
| PTV | V42.8Gy | < 2% |
| V36.25Gy | ≥ 95% | |
| V34.4Gy | ≥ 98% | |
| Bladder | V37Gy | < 5 cc. |
| V18Gy | < 40% | |
| Rectum | V36Gy | < 1 cc. |
| V18Gy | < 50% | |
| Right and Left femoral head | V14.5Gy | < 5% |
| Case | Age | PSA before RT | GS | T stage | N stage | M stage | Risk group | Type of ADT | Medications | PSA 2-mo post Tx | PSA Change/month |
| 1 | 77 | 7 | 3+4 | 2a | 0 | 0 | Favorable intermediate | E | None | 1.94 | -2.53 |
| 2 | 63 | 4.2 | 3+4 | 2a | 0 | 0 | Favorable intermediate | None | None | 0.04 | -2.08 |
| 3 | 70 | 8.5 | 3+4 | 2a | 0 | 0 | Favorable intermediate | E | None | 0.07 | -4.21 |
| 4 | 73 | 14.5 | 3+3 | 2 | 0 | 1b | N/A | S | Abi | 0.061 | -7.21 |
| 5 | 77 | 11 | 3+4 | 2a | 0 | 0 | Unfavorable intermediate | E | None | 0.4 | -5.3 |
| Case | Vol of PTV | Vol of CTV | V34.4PTV (%) | V36.25PTV (%) | V42.8PTV (%) | V37B (cc.) | D50B (%) | V36R (cc.) | V18R (%) |
| 1 | 61.52cc | 25.08cc | 99.9% | 97.3% | 0% | 0.67 | 39.4 | 0.82 | 47.1 |
| 2 | 122.38cc | 66.32cc | 100% | 96.6% | 0% | 1.51 | 27.8 | 0.04 | 32.6 |
| 3 | 83.35cc | 42.14cc | 99.9% | 95.6% | 0% | 7.63 | 29.6 | 2.67 | 32 |
| 4 | 69.44cc | 45.95cc | 100% | 98.1% | 0% | 5.81 | 8.4 | 0.8 | 36.4 |
| 5 | 58.55cc | 33.72cc | 99.9% | 95.8% | 0% | 3.88 | 12 | 0.96 | 45 |
| Parameter | Median (mm) | Interquatile range (mm) |
| Potential Differentiation | 0.75 | 0.46 to 1.34 |
| Rigid Body | 1.04 | 0.74 to 1.39 |
| Target Offset X | 0.96 | -0.72 to 0.66 |
| Target Offset Y | -0.26 | -1.15 to 0.35 |
| Target Offset Z | -1.54 | -2.80 to -0.38 |
| Overall Target Offset (3D) | 2.52 | 1.53 to 3.30 |
| No | planned BOT (s) | 1st | 2nd | 3rd | 4th | 5th | Avg Tx time from 5 Fx (s) | % incresing time compare to planned BOT | |||||
| Tx time (s) | Number of Interruption (#) | Tx time (s) | Number of Interruption (#) | Tx time (s) | Number of Interruption (#) | Tx time (s) | Number of Interruption (#) | Tx time (s) | Number of Interruption (#) | ||||
| 1 | 529.7 | 1094 | 14 | 555 | 0 | 555 | 0 | 559 | 0 | 641 | 2 | 680.8 | 28.53% |
| 2 | 598.2 | 633 | 0 | 628 | 0 | 656 | 3 | 623 | 0 | 631 | 0 | 634.2 | 6.02% |
| 3 | 488.3 | 523 | 0 | 523 | 0 | 562 | 1 | 670 | 4 | 548 | 1 | 565.2 | 15.75% |
| 4 | 448.4 | 481 | 0 | 473 | 0 | 481 | 0 | 473 | 0 | 503 | 1 | 482.2 | 7.54% |
| 5 | 509.7 | 534 | 0 | 585 | 1 | 612 | 2 | 578 | 1 | 542 | 0 | 570.2 | 11.87% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Diagnosis and Treatment · Prostate Cancer Treatment and Research · Advanced Radiotherapy Techniques
Introduction
Ultra-hypofractionated radiotherapy is increasingly used for prostate cancer, aiming to deliver highly conformal doses in fewer fractions (more than 6 Gy per fraction). Randomized trials have demonstrated the non-inferior biochemical outcome and toxicity compared to dose-escalated conventional fractionation [1-7].
However, the precision required for safe dose delivery in ultra-hypofractionated radiotherapy faces a significant challenge: intrafraction prostate motion. Studies have shown that prostate displacement exceeding 5 mm occurs in more than 75% of treatment fractions, primarily due to bladder filling and bowel movement [8,9]. Such motion patterns risk both target underdosing and increased dose to adjacent organs at risk, particularly concerning when delivering these higher doses per fraction.
Several motion management systems exist for prostate ultra-hypofractionation, each with distinct technical approaches. These include magnetic resonance (MR)-guided linear accelerators (MR-LINAC), electromagnetic tracking systems (Calypso; Varian Medical Systems, Palo Alto, CA, USA), and robotic arm-mounted LINACs (CyberKnife; Accuray, Sunnyvale, CA, USA). MR-guided systems, in particular, allow direct visualization of the prostate and can detect both translational and rotational shifts, contributing to a more detailed understanding of prostate motion during treatment [10]. However, clinical implementation is often constrained by platform availability, with many centers limited to conventional LINAC-based solutions. The Synchrony system on the Radixact platform (Accuray) offers a fiducial-based tracking alternative for facilities without access to these specialized technologies. While this technology theoretically improves treatment accuracy, its practical implementation in ultra-fractionation radiotherapy remains limited [11,12].
This case series investigates the early real-world performance of Synchrony motion tracking during ultra-hypofractionated prostate radiotherapy, with particular focus on motion and characterizing treatment interruptions and their operational impact. Through comprehensive analysis of delivery parameters and motion compensation events, this study aims to evaluate the system’s clinical feasibility and identify potential optimization opportunities for prostate radiotherapy workflows.
Case presentation
Five patients with localized prostate cancer were enrolled in this study. All suitable candidates for ultra-hypofractionated radiotherapy and were treated at Chiang Mai University Hospital.
Radiotherapy planning and preparation
Prior to CT simulation, each patient underwent transperineal implantation of three gold fiducial markers under transrectal ultrasound guidance and local anesthesia. This procedure was performed by a specialized urologist to ensure accurate placement for optimal target tracking. The image set of a Computed Tomography (CT) with 1 mm of slice thickness was acquired from the Computed Tomography simulator (SOMATOM Definition AS, Siemens Healthineers, Erlangen, Germany).
For treatment planning, the clinical target volume (CTV) was defined as the entire prostate gland. To account for setup uncertainties, a uniform 3-mm isotropic expansion was applied to the CTV to generate the planning target volume (PTV). Organs at risk (OARs), including the bladder, rectum, and urethra, were contoured, and appropriate dose constraints were applied to minimize toxicity. For planning we used the VOLO ultra (Accuray, Inc., Madison, WI, USA) for dose calculation system, with a prescription of 36.25 Gy in five fractions of 7.25 Gy to the prostate PTV. OAR constraints were defined for the bladder, rectum, penile bulb, and femoral heads. Treatment plans were evaluated using adapted criteria from the PACE-B trial with strict dosimetric criteria as follows (Table 1, Figure 1) [3].
Ultra-hypofractionation in prostate cancer – Dose distribution of case #3
Treatment was delivered using the Synchrony system on the Radixact platform (Accuray, Inc.) with daily helical kV CT (ClearRT) for initial patient setup via fiducial marker matching. Intrafractional motion was monitored by acquiring 2D kV radiographic images (six times per gantry rotation), enabling real-time fiducial tracking. The Synchrony stereotactic body radiation therapy (SBRT) delivery adhered to predefined motion thresholds: potential difference (3D distance error): ≤ 2 mm, target offset (predicted displacement from planning CT): ≤30 mm, and rigid body constraint (fiducial pair distance deviation): ≤ 1.5 mm. If any threshold was exceeded, radiation delivery was automatically paused, and a corrective intrafraction kV CT was acquired at predefined gantry angles (35°, 145°, 215°, 325°) to reposition the target. The Synchrony tracking system (Figure 2) enabled continuous real-time monitoring during treatment delivery. Comprehensive dosimetric and motion parameters were recorded for quality assurance, including PTV coverage, OAR doses, fiducial marker displacement, and the frequency of treatment interruptions per fraction.
Synchrony platform in monitor
Results
The study consisted of five patients with localized prostate cancer who underwent ultra-hypofractionated radiotherapy. Detailed patient characteristics, including demographics, disease staging, and treatment parameters, are presented in Table 2. The mean CTV was 42.65 cc (range: 25.08-66.32 cc.) (Table 3). All patients met target coverage constraints. While most OAR doses remained within protocol limits, two cases had higher than constraints: Case 3 exceeded rectal V36Gy (1.1 cc vs. <1 cc constraint) and bladder V37Gy (6.7 cc vs. <5 cc), while Case 4 showed elevated bladder V37Gy (6.5 cc). All other OAR parameters across the cohort were maintained below constraints.
Treatment delivery
The Synchrony tracking data from five patients demonstrates systematic motion patterns with clinical relevance. The system showed acceptable overall tracking accuracy, as shown in Table 4. Notably, there was a pronounced posterior shift in the Z-axis with a median displacement of -1.54 mm (IQR: -2.80 to -0.38 mm) and a substantial composite 3D variability with a median of 2.52 mm (IQR: 1.53 to 3.30 mm). The overall target offset is calculated by sqrt(𝑋^2^ + 𝑌^2^ + 𝑍^2^).
The mean value of planning beam-on time and actual beam-on time were 514.9 and 586.5 seconds, respectively. The average percentage of additional time was 13.9%. For the details of pausing, all pauses during treatment of these patients are shown in Table 5.
The treatment was well-tolerated, with only one patient (20%) developing acute grade 1 gastrointestinal toxicity (diarrhea) according to Common Terminology Criteria for Adverse Events (CTCAE) v5.0 criteria. This resolved completely with supportive care.
Discussion
This case series demonstrates the successful implementation of ultra-hypofractionated prostate radiotherapy using the Synchrony real-time motion tracking system, with acceptable dosimetric outcomes and no acute high-grade toxicities. Our findings contribute to the growing evidence supporting ultra-hypofractionation RT for localized prostate cancer, while highlighting the unique advantages of continuous intrafraction tracking compared to daily image-guided radiotherapy [1-7].
In our initial experience with ultra-hypofractionated radiotherapy (36.25 Gy in five fractions), we observed a remarkably rapid PSA decline averaging -4.27 ng/mL per month. This substantially exceeds the previously reported decline rates of -0.47 to -0.09 ng/mL per month in the first year post-treatment, reinforcing existing evidence that ultra-hypofractionation induces faster biochemical response kinetics compared to conventional fractionation regimens [13]. However, interpretation requires caution: 80% of our cohort received concurrent ADT (castration: 4/5; abiraterone: 1/5), which likely augmented the early PSA dynamics. While these results align with the hypothesis that ultra-hypofractionation may enhance tumor control, the confounding effects of systemic therapy preclude definitive attribution of biochemical response solely to radiation.
For the toxicity report, with a median follow-up of two months, revealed only one case of acute Grade 1 GI/GU toxicity - a notably lower incidence compared to the 53-57% rate reported in the PACE-B trial at 12 weeks [3-6]. This discrepancy may stem from several factors, including the use of real-time tumor tracking via Synchrony, which enhances precision in dose delivery, as well as our more conservative CTV-to-PTV expansion (3 mm vs. PACE-B’s 5-7 mm). Additionally, our prescribed dose did not include escalation to 40 Gy for the CTV, unlike PACE-B, where select patients received higher doses to dominant lesions. However, the shorter follow-up duration in our study limits the assessment of late toxicities, which typically emerge beyond six months. While these early results suggest that advanced motion management and tighter margins may reduce acute toxicity, longer-term data will be essential to fully evaluate the safety profile of our approach compared to established protocols.
The Synchrony system demonstrated clinically excellent motion tracking performance, with all directional displacements (X, Y, and Z axes) maintaining means and standard deviations below 5 mm - similar to the previously reported values for alternative tracking systems [9,14]. Notably, the observed posterior moved showed in the Z-axis represented the most significant directional variation, though still within clinically acceptable thresholds [15,16]. These motion patterns triggered automatic safety pauses primarily during initial fractions, with setup variations being the most frequent cause. The system's efficient correction mechanism limited the total treatment time increase to under 15% compared to planned duration, while ensuring continuous positional accuracy. Though these findings are based on a five-patient cohort, they suggest Synchrony offers superior motion management for prostate SBRT compared to existing technologies, warranting further investigation in larger studies.
Conclusions
Synchrony successfully enhances ultra-hypofractionated prostate radiotherapy by providing dynamic motion management throughout treatment delivery. The system's automatic correction mechanism maintains treatment precision through controlled pauses when needed, while its consistent tracking performance ensures reliable target localization. This operational approach supports both therapeutic effectiveness - as evidenced by rapid biochemical response - and an excellent safety profile, confirming its value in optimizing prostate ultra-hypofractionation delivery. However, as these findings are based on a small cohort of five patients, further studies with larger sample sizes are needed to validate these results.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial Lancet Widmark A Gunnlaugsson A Beckman L 38539539420193122737310.1016/S 0140-6736(19)31131-6 · doi ↗ · pubmed ↗
- 2Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer (HYPO-RT-PC): patient-reported quality-of-life outcomes of a randomised, controlled, non-inferiority, phase 3 trial Lancet Oncol Fransson P Nilsson P Gunnlaugsson A 2352452220213344452910.1016/S 1470-2045(20)30581-7 · doi ↗ · pubmed ↗
- 3Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial Lancet Oncol Brand DH Tree AC Ostler P 153115432020193154079110.1016/S 1470-2045(19)30569-8PMC 6838670 · doi ↗ · pubmed ↗
- 4Intensity-modulated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): 2-year toxicity results from an open-label, randomised, phase 3, non-inferiority trial Lancet Oncol Tree AC Ostler P van der Voet H 130813202320223611349810.1016/S 1470-2045(22)00517-4 · doi ↗ · pubmed ↗
- 5Phase 3 trial of stereotactic body radiotherapy in localized prostate cancer N Engl J Med van As N Griffin C Tree A 1413142539120243941337710.1056/nejmoa 2403365 PMC 7616714 · doi ↗ · pubmed ↗
- 6Dosimetric comparison of Cyber Knife and conventional LINAC prostate stereotactic body radiation therapy plans: analysis of the PACE-B study Int J Radiat Oncol Biol Phys Ratnakumaran R Sasitharan A Khan A 202510.1016/j.ijrobp.2025.01.01439862896 · doi ↗ · pubmed ↗
- 7Acute toxicity of ultrahypofractionation compared with moderate hypofractionation in prostate cancer treatment: a randomized trial Int J Radiat Oncol Biol Phys Kwan W Bahl G Kim D Ye A Gagne I Alexander A 1036104311320223541776310.1016/j.ijrobp.2022.04.006 · doi ↗ · pubmed ↗
- 8Multi-institutional clinical experience with the Calypso System in localization and continuous, real-time monitoring of the prostate gland during external radiotherapy Int J Radiat Oncol Biol Phys Kupelian P Willoughby T Mahadevan A 108810986720071718794010.1016/j.ijrobp.2006.10.026 · doi ↗ · pubmed ↗