A spicy twist: A rare case of anaphylaxis to banana pepper
Ishitha Jagadish, Phoebe Newell, Ricardo J. Estrada-Mendizabal, Saiyara S. Shama, Alexei Gonzalez-Estrada

TL;DR
A 30-year-old man experienced a severe allergic reaction to banana peppers, confirmed through skin testing.
Contribution
This is the first reported case of anaphylaxis caused specifically by banana peppers.
Findings
Anaphylaxis was confirmed via positive prick-to-prick testing with banana pepper.
The patient had a history of asthma and allergic rhinitis.
This case highlights the potential for rare allergens like banana peppers to cause severe reactions.
Abstract
This case report describes the first documented instance of banana pepper (Capsicum annuum)-induced anaphylaxis in a 30-year-old male with intermittent asthma and allergic rhinitis, confirmed through positive prick-to-prick testing.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
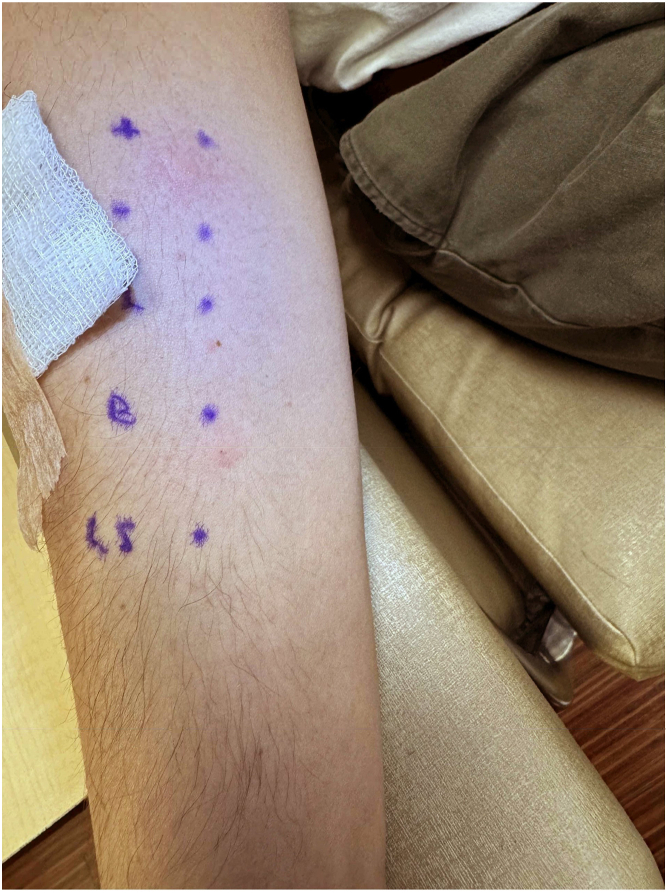 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransgenic Plants and Applications · Food Allergy and Anaphylaxis Research · Plant Virus Research Studies
Anaphylaxis is a severe, potentially life-threatening allergic reaction that can be triggered by various foods, medications, and environmental exposures. Although food-induced anaphylaxis is often attributed to common allergens such as peanuts, shellfish, and tree nuts, less common triggers can be easily overlooked. Capsicum cultivars, which include bell peppers, chili peppers, banana peppers, and more, are rare but potential causes of anaphylaxis. Reports of anaphylaxis in response to banana peppers (Capsicum annuum) are particularly sparse, making it a less-recognized allergen with unknown incidence or prevalence. This case report presents a rare instance of anaphylaxis in a 30-year-old male with asthma and allergic rhinitis following the consumption of a spiced lamb dish containing banana peppers. Given the exacerbation of asthma symptoms after anaphylaxis in this patient, the report further discusses the need for reassessment of asthma control and personalized patient education.
A 30-year-old male with asthma and allergic rhinitis had been effectively managing both conditions with as-needed albuterol and over-the-counter antihistamines without any recent changes to his medication regimen. Incidentally, he developed wheezing, dyspnea, hoarseness, pruritic lips without angioedema or urticaria, and abdominal pain within 10 minutes of consuming a spiced lamb takeout dish. At time of presentation to the emergency department, his vital signs were normal. He was treated with 1 dose of epinephrine, intravenous steroids, and histamine-1 and histamine-2 receptor blockers, leading to complete resolution of his symptoms within 3 hours. An allergist confirmed the contents of the dish with the restaurant owner. It included lamb, salt, ground red pepper, black pepper, onions, basmati rice, tomato, pita, basil, butter, and pepperoncini (a type of banana pepper). The patient had no history of anaphylaxis to food allergens and could not recall previous consumption of this specific variety of banana pepper. He actively avoided lamb and banana pepper ingredients following the index reaction. Skin and prick-to-prick testing revealed a negative result for fresh lamb but a positive result for banana pepper (Fig 1), confirming the diagnosis of anaphylaxis in response to the pepper. Additionally, banana pepper prick-to-prick testing was performed on 8 healthy controls, with 7 of those tested having negative results. Serum-specific C annuum IgE was not commercially available at our institution. The patient was advised to avoid all Capsicum cultivars and instructed on use of an epinephrine autoinjector. His asthma, which had previously been controlled with as-needed albuterol, was exacerbated by the allergic reaction, resulting in daily dyspnea for 1 week. He reported no asthma-related nighttime awakenings in the preceding month, nor did he have any acute asthma exacerbations or need for systemic steroids in the previous year. Given the likely association between the patient’s allergic reaction and now-uncontrolled intermittent asthma, a baseline serum tryptase level was ordered and determined to be 6.8 ng/mL. The patient was counseled on proper albuterol inhaler use. As of 6 months after the incident, the patient has been successfully avoiding consumption of or contact with Capsicum cultivars.Fig 1. Prick-to-prick testing results. The results of prick-to-prick testing were negative (wheal size, 0 mm; flare size, 0 mm flare) for fresh lamb (L) and positive (wheal size, 5 × 8 mm; flare size, 8 ×10 mm) for banana pepper (B).
Although Capsicum cultivars are widely consumed, reports of anaphylaxis in response to them are rare. A PubMed search using the key term Capsicum anaphylaxis yielded only 8 articles published since 1998, most of which were case reports involving bell pepper, pickled chili pepper, paprika, or Capsicum spray.1, 2, 3, 4, 5, 6, 7, 8 The remaining 2 studies analyzed sensitization profiles in response to bell pepper and immunoreactive proteins in Capsicum-based spices.7^,^8 To the best of our knowledge, this case report presents the first documented instance of anaphylaxis triggered by banana pepper, contributing to the limited literature on Capsicum-induced allergic reactions.
The identification of banana pepper as the allergen in this case was achieved through a meticulous review of the patient's dietary history and verification of culprit dish’s ingredients with the restaurant owner. Such investigations are crucial for achieving accurate diagnosis and identification of possible trigger(s). Patient education on avoidance of Capsicum cultivars and proper use of epinephrine autoinjectors was essential for future prevention. If the patient wished to reintroduce Capsicum plants into his diet, an expanded skin prick testing panel could be considered. However, not much is known about potential cross-reactivity among different Capsicum species; hence, desensitization strategies have not been officially established.8 Additionally, the post-anaphylactic exacerbation of asthma symptoms in this patient emphasizes the need for reassessment of asthma control and counseling on the appropriate use of rescue medications.
The scarcity of literature regarding Capsicum-induced allergic reactions underscores the need for awareness among health care providers about the potential of less common food allergens to provoke severe reactions in sensitized individuals. More extensive epidemiologic studies are warranted to determine the prevalence and incidence of anaphylaxis to Capsicum species. Given the presumed rarity of such occurrences, future research should focus on identifying and characterizing the allergic proteins within various Capsicum plants to help investigate cross-reactivity, diagnostic strategies, and management options such as desensitization and/or allergen immunotherapy. Because of the potential variability of allergens among Capsicum cultivars, there may be a need to develop expanded standardized testing panels for skin prick testing and specific IgE testing to improve diagnostic accuracy. Following anaphylactic reactions, allergists should assess and manage any coexacerbations of chronic conditions, such as asthma, to ensure comprehensive care. Patients should be advised on how to avoid triggers, when and how to use epinephrine autoinjectors, and when to seek urgent evaluation. Long-term follow-up is crucial to evaluate the effectiveness of avoidance strategies and their impact on the patient’s quality of life.
Disclosure statement
Disclosure of potential conflict of interest: The authors declare that they have no relevant conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Galleani C.Valdelvira R.Carmen Diéguez M.Crespo J.F.Cabanillas B.Anaphylaxis to pickled chili pepper (Capsicum frutescens): role of pickling processing in the allergic reactivity Ann Allergy Asthma Immunol 13020233693703653897110.1016/j.anai.2022.12.020 · doi ↗ · pubmed ↗
- 2Niemcunowicz-Janica A.Ptaszyńska-Sarosiek I.Wardaszka Z.Zgon po uzyciu aerozolowego miotacza pieprzu [Sudden death caused by an oleoresin capsicum spray]Arch Med Sadowej Kryminol 59200925225420441089 · pubmed ↗
- 3García-Menaya J.M.Cordobés-Durán C.Bobadilla-González P.Ledesma A.Perez-Rangel I.Sanchez-Vega S.Zambonino M.A.Anaphylactic reaction to bell pepper (Capsicum annuum) in a patient with a latex-fruit syndrome Allergol Immunopathol (Madr)4220142632652353759110.1016/j.aller.2012.12.006 · doi ↗ · pubmed ↗
- 4Callero A.Perez E.Ledesma A.Martinez-Tadeo J.A.Hernandez G.Rodriguz-Plata E.A case report of bell pepper anaphylaxis: could 1, 3-β-glucanase be the culprit allergen?Ann Allergy Asthma Immunol 10920124744752317689410.1016/j.anai.2012.10.004 · doi ↗ · pubmed ↗
- 5Vega de la Osada F.Esteve Krauel P.Alonso Lebrero E.Ibáñez Sandín M.D.Muñoz Martínez M.C.Laso Borrego M.T.Sensibilización al pimentón: anafilaxia por ingestión y rinoconjuntivitis tras contacto por vía aérea [Sensitization to paprika: anaphylaxis after intake and rhinoconjunctivitis after contact through airways]Med Clin (Barc)11119982632669789242 · pubmed ↗
- 6Rüger R.D.Wagner S.Simon J.C.Treudler R.Schwere Soforttypallergie nach Verzehr roher Paprika [Severe type 1 allergy to raw bell pepper]Hautarzt 61201033934210.1007/s 00105-009-1776-319475361 · doi ↗ · pubmed ↗
- 7Callero A.Cabrera-Hernandez V.Perez-Rodríguez E.Jimeno-Nogales L.Martinez-Tadeo J.A.Plata-Rodriguez E.Bell Pepper allergy: different sensitization profiles J Investig Allergol Clin Immunol 28201834034210.18176/jiaci.027830350789 · doi ↗ · pubmed ↗
- 8Wróblewska B.Ogrodowczyk A.Wasilewska E.Immunoreactive proteins of Capsicum-based spices as a threat to human health: mass spectrometry analysis and in silico mapping Sci Rep 1320231772310.1038/s 41598-023-44775-3PMC 1058483937853105 · doi ↗ · pubmed ↗