Comprehensive assessment of lower limb edema and its association with quality of life among men with prostate cancer
Sandra Jensen, Andreas Røder, Sandi Hayes, Gitte Sone Larsen, Mikkel Fode, Peter Busch Østergren, Muhammad Munther Nasir Al-Hamadani, Christoffer Johansen, Bolette Skjødt Rafn

TL;DR
Lower limb edema is common in men with prostate cancer and negatively affects their quality of life, but it is often overlooked and under-discussed.
Contribution
This study is the first to comprehensively assess the prevalence and impact of lower limb edema in prostate cancer patients using bioimpedance and quality of life questionnaires.
Findings
Lower limb edema was found in 11% of prostate cancer patients.
Patients with LLE reported significantly lower quality of life scores and more symptoms.
Most patients with LLE wanted more information on managing their condition.
Abstract
Lower limb edema (LLE) is characterized by swelling due to fluid accumulation and is an under-recognized condition in men with prostate cancer. This study investigated the prevalence of LLE and explored its impact on daily living, depression, and health-related quality of life (HRQoL). This cross-sectional study included men with prostate cancer who attended follow-up at the Department of Urology, Rigshospitalet, Denmark, during a 3-month period. LLE was defined as an L-Dex ≥ 10, measured by using bioimpedance spectroscopy, combined with self-reported symptoms (≥ 2 of heaviness, swelling, or tightness) using items from European Organisation for Research and Treatment of Cancer Quality of Life (EORTC) QLQ-VU34. HRQoL, depression, and the impact of LLE on daily living were assessed using self-reported questionnaires. Among 401 patients, LLE was identified in 45 (11%) patients.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
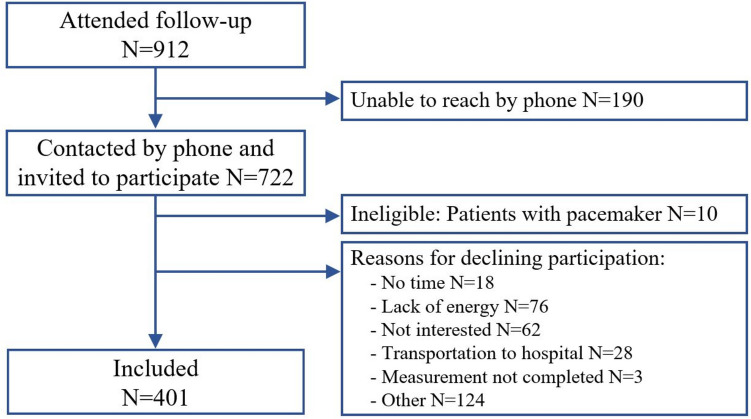 Figure 1
Figure 1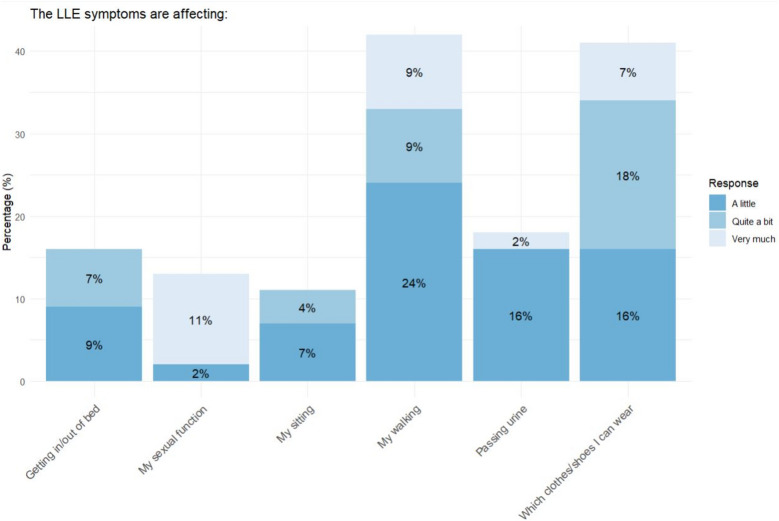 Figure 2
Figure 2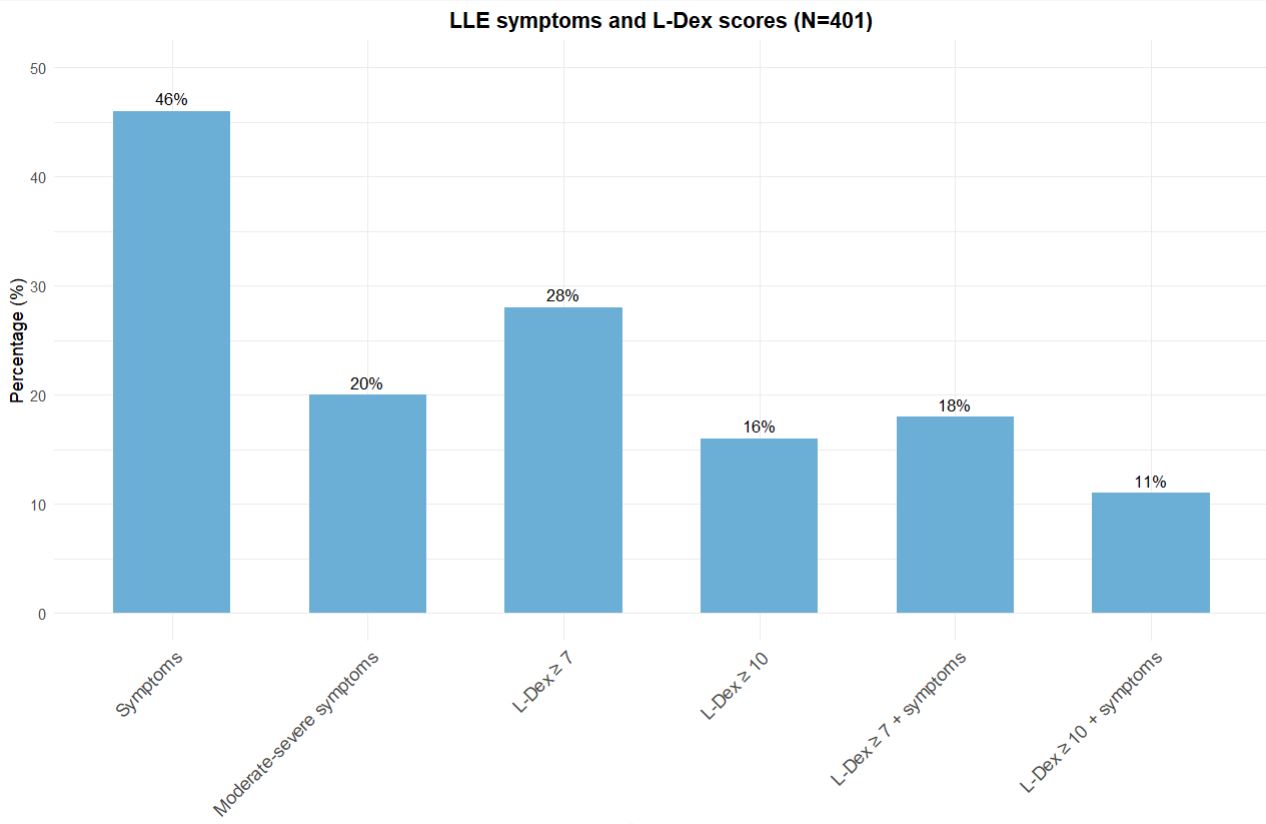 Figure 3
Figure 3- —National Hospital
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenital Health and Disease · Diagnosis and Treatment of Venous Diseases · Prostate Cancer Diagnosis and Treatment
Introduction
Prostate cancer and its treatment can contribute to lower limb edema (LLE) [1]. LLE is an accumulation of excess fluid within the body’s tissues, commonly presenting as swelling in areas such as the legs, ankles, and feet [2]. LLE can arise from multiple factors, including cancer itself, cancer treatments, and other systemic health disorders [3, 4]. This condition typically presents with swelling, as well as sensations of heaviness and tightness in the limbs and genital area. While initially reversible, LLE can progress to a chronic condition over time, with permanent intradermal fibrosis and tissue inflammation [3, 4].
The risk of LLE for men with prostate cancer is explained through several mechanisms. Prostate cancer often spreads to lymph nodes in the pelvic area, and this lymphatic obstruction may cause lymphedema in the legs and genital area [4]. In addition, treatment-related factors may play a substantial role in the development of LLE. Hormone therapies for prostate cancer, such as abiraterone, GnRH agonists, GnRH antagonists, and enzalutamide, are associated with increased fluid retention or elevated blood pressure, which may lead to LLE [5–7]. Also, chemotherapy, e.g., docetaxel can contribute to LLE by increasing blood vessel permeability, leading to fluid leakage into the surrounding tissue, and disrupting fluid balance and lymphatic drainage [8–10]. Finally, surgery and radiation treatments targeting pelvic lymph nodes, while important for prognosis, may damage the lymphatic system, thereby exacerbating the risk of LLE [1].
Aside from the tumor topography and the treatment of prostate cancer, general health conditions that become more common by age, such as hypertension, high body mass index (BMI), chronic venous insufficiency, and heart failure, are also significant factors, which contribute as etiological agents for LLE. Together, these conditions increase the risk of LLE [11–14]. Men with prostate cancer are however often inadequately informed about LLE as a potential late effect of cancer and the treatment thereof [15].
LLE can significantly impact quality of life, causing physical discomfort, psychological distress, and increased depressive and somatic symptoms [16, 17]. Despite these burdens, studies investigating LLE in men with prostate cancer are limited. Previous research has often focused on small cohorts or populations of women, with findings that may not be directly applicable to men [18–20]. Additionally, many studies have relied on inconsistent definitions and non-standardized assessment methods, leading to varying prevalence estimates from 0 to 9% after radiation therapy alone, 0–14% following radical prostatectomy with pelvic lymph node dissection (PLND), to 18–29% when both treatments are combined [1].
This study addresses these gaps by combining patient-reported outcomes and objective measurements, to provide a comprehensive assessment of LLE and to investigate its prevalence and impact on activities of daily living, depression, and health-related quality of life among men with prostate cancer.
Materials and methods
Design and participants
This cross-sectional study included men with prostate cancer attending follow-up visits at the Department of Urology, Rigshospitalet, Denmark, between November 1 st, 2022, and January 31 st, 2023. Inclusion criteria were a diagnosis of prostate cancer, age ≥ 18 years, ability to read and understand Danish to complete patient-reported outcomes. Patients were eligible if they had received any treatment modality for prostate cancer, both active (i.e., surgery or androgen deprivation therapy (ADT)) or passive (i.e., watchful waiting or active surveillance). Patients with pacemakers were excluded, as this is a contraindication for the measurement of LLE by bioimpedance spectroscopy (BIS). All patients were contacted by telephone and invited to one in-person visit to complete patient-reported outcomes and undergo measurements with BIS. Two attempts to reach each patient by telephone was conducted to offer participation.
Outcome measures
Socio-demographic and clinical characteristics
Socio-demographic characteristics and general comorbidities were self-reported. Clinical and treatment-related variables were extracted from the medical records. The Gleason score was obtained from prostatectomy specimens for patients who underwent surgery, and from biopsies for others. Body weight was measured at the in-person visit. All data were registered in the REDCap database [21].
Measurement of LLE
Each participant was assessed twice using the BIS device (SOZO® Digital Health Platform by ImpediMed), and the average lymphedema index (L-Dex) was recorded. The L-Dex score is calculated from the impedance ratio between limbs and provides a measure of extracellular fluid levels, with values of ≥ 10 indicating the presence of lymphedema [22]. Using the vulvar cancer-specific subscale of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ–VU34 items 39, 40, 41, 44, 45, and 46), participants were asked to rate presence of heaviness, swelling, or tightness in the legs, groin, or genital area within the past 2 weeks using a 4-point Likert scale, with response options of 1 = “not at all,” 2 = “a little,” 3 = “quite a bit,” and 4 = “very much” [23]. Swelling, tightness, and heaviness are commonly used to assess lymphedema-related symptoms; however, these aspects are not sufficiently covered in prostate cancer-specific tools, which is why the EORTC QLQ-VU34 items were chosen [24]. The presence of LLE was defined as L-Dex of ≥ 10 [25, 26] and at least one self-reported LLE-associated symptom (heaviness, swelling or tightness) of ≥ 2.
Patient-reported outcomes
Health-related quality of life
Health-related quality of life (HRQoL) was measured by EORTC QLQ-C30 which includes functional scales (physical, role, cognitive, emotional, and social functioning), symptom scales (fatigue, pain, and nausea/vomiting), a global health status/QoL scale, and single symptom items. Functional and symptom scales are rated on a 4-point Likert scale (1 = “not at all” to 4 = “very much”), while the global health status/QoL scale uses a 7-point scale (1 = “very poor” to 7 = “excellent”). Higher scores on the functional and global health scales indicate better functioning and HRQoL, whereas higher scores on symptom scales reflect greater severity [27, 28].
Prostate cancer-specific HRQoL
The EORTC QLQ-PR25 is a prostate cancer-specific subscale that includes symptom and functional domains: urinary symptoms, bowel symptoms, hormonal treatment-related symptoms, and sexual functioning. Higher scores on symptom domains indicate more severe symptoms, and higher scores on the sexual functioning domain represent better sexual functioning [29].
Depression
Depression was assessed using the Major Depression Inventory (MDI), which cover the frequency of 10 depressive symptoms within the last 2 weeks, each rated on a 6-point Likert scale (0 = “at no time” to 5 = “all the time”). The total score ranges from 0 to 50, with scores of ≤ 20 indicating no depression, 21–25 mild depression, 26–30 moderate depression, and ≥ 31 severe depression [30, 31].
Impact of LLE
Impact of LLE was administered to participants who reported LLE-associated symptom (heaviness, swelling or tightness) of ≥ 2 using The Lymphoedema Genito-Urinary Cancer Questionnaire (LGUCQ) tool, which accesses the impact on daily living. Items are rated on a Likert scale from 0 to 3, with 0 indicating “not at all” and 3 indicating “very much” [32].
Ethics
The Capital Region of Copenhagen Ethical Committee judged that ethical approval was not required (F-23004790) and The Danish Data Protection Agency (R-22071980) approved contacting patients by phone for participation. All patients were informed verbally and in writing about the study. Only men who provided written informed consent were included. The Helsinki Declaration was followed for all aspects of the study.
Statistical analysis
Descriptive statistics were used to summarize socio-demographic and clinicopathological characteristics, with categorical variables presented as frequencies, and continuous variables as mean ± standard deviation or median and 25 th percentile (Q1), 75 th percentile (Q3), depending on distribution. Welch’s t-test, χ^2^ tests, or Mann–Whitney U test was used to compare clinicopathological variables and depression between participants with and without LLE. LLE prevalence and severity of symptoms were presented descriptively, and LLE treatment variables were analyzed as binary outcomes. Stepwise backward regression using Akaike Information Criterion was applied to identify variables explaining LLE likelihood, followed by multivariate logistic regression to calculate odds ratios (ORs) with 95% confidence intervals (CIs) for the final model predictors. Differences in HRQoL were analyzed using Welch’s t-test and multiple linear regression, with results presented as mean differences with 95% CI across three models: (a) unadjusted; (b) adjusted for age, BMI, comorbidities associated with LLE, self-reported comorbidities, and pre-diagnosis swelling; and (c) further adjusted for time since diagnosis and treatment modalities, including radical prostatectomy, chemotherapy, radiation therapy, ADT, and lymph node removal. Participants and non-participants were compared on age using Welch’s t-test, as age was the only variable available for the non-participants.
Results
A total of 912 patients were scheduled for follow-up visits for prostate cancer at Rigshospitalet between November 2022 and January 2023. Of these, 722 patients could be reached by telephone and invited to the study. Subsequently, 401 (56%) agreed to participate in the study and completed both patient-reported outcomes and BIS measurements. Ten patients were excluded due to having a pacemaker and 311 patients declined participation. Most patients declined due to lack of energy, no interest, or other reasons (Fig. 1). Patients who declined to participate in the study were older than those who participated (74 years ± 9 vs. 72 years ± 8, p < 0.001).Fig. 1. Flowchart
The majority of participants were either overweight or obese (n = 265, 66% had BMI ≥ 25), were either former or current smokers (n = 224, 58%), and almost one-third lived alone (n = 108, 27%) (Table 1). On average, participants were 5 years (Q1: 2, Q3: 8) post prostate cancer diagnosis. Half of the participants had undergone radical prostatectomy (n = 203, 51%) with PLND in 36% of the cases (n = 146). On average 17 ± 5 nodes were removed, and 2 (Q1: 1, Q3: 3) showed metastases. Approximately one in two (n = 217, 54%) had or were receiving ADT, while 27% (n = 107) had received radiation therapy, and 15% (n = 59) were in watchful waiting or active surveillance. Table 1. Participant characteristicsAllN** = 401LLEN = 45No LLEN = 356Differencep-valueMean ± SDMedian (Q1, Q3)N (%)Mean ± SDMedian (Q1, Q3)N (%)Mean ± SDMedian (Q1, Q3)N (%)Mean or median difference (95% CI)Age72 ± 875 ± 771 ± 84 (2, 6)0.002BMI, kg/m**^2^ < 0.001 < 25 25–29.9 ≥ 30136 (34%)182 (45%)83 (21%)9 (20%)17 (38%)19 (42%)127 (36%)165 (46%)64 (18%)Highest level of education0.908 Primary or secondary school Vocational education Continued education (2–3 years) Continued education (3–4 years) Continued education (> 4 years) Other36 (9%)102 (25%)37 (9%)85 (21%)126 (31%)15 (4%)4 (9%)9 (20%)3 (7%)11 (24%)16 (36%)2 (4%)32 (9%)93 (26%)34 (10%)74 (21%)110 (31%)13 (4%)Annual household income, DKK0.611 100.000–250.000 250.000–400.000 400.000–700.000 ** > 700.00091 (23%)101 (25%)108 (27%)101 (25%)13 (29%)11 (24%)9 (20%)12 (27%)78 (22%)90 (2%)99 (28%)89 (25%)Living alone108 (27%)10 (22%)98 (28%)0.564Smoking0.515 Yes No Former smoker55 (14%)160 (42%)169 (44%)6 (13%)19 (42%)20 (44%)49 (14%)141 (40%)149 (42%)Years since diagnosis5 (2, 8)6 (3, 10)5 (2, 8)1 (0, 2)0.149PSA score10 (7, 18)12 (8, 15)10 (7, 18)1 (− 1, 3)0.155Gleason score**0.179 6 7 (3 + 4) 7 (4 + 3) 8 9–1065 (16%)131 (33%)78 (20%)33 (8%)90 (24%)5 (12%)13 (30%)5 (12%)6 (14%)14 (33%)60 (17%)118 (33%)73 (21%)27 (8%)76 (22%)Stage0.293 I II III IV40 (10%)140 (35%)116 (28%)105 (26%)6 (13%)10 (22%)15 (33%)14 (31%)34 (10%)130 (37%)101 (28%)91 (26%)Reported swelling before diagnosis0.002 No swelling Swelling Missing223 (56%)52 (13%)136 (34%)19 (63%)11(37%)15 (33%)204 (87%)31 (13%)121 (34%)Self-reported comorbidities0.027 No comorbidities 1–2 comorbidities 3–5 comorbidities203 (51%)166 (41%)32 (8%)18 (40%)19 (42%)8 (18%)185 (52%)147 (41%)24 (7%)Comorbidities related to edema Heart failure Hypertension Valvular heart disease Venous thrombosis17 (4%)212 (53%)76 (19%)21 (5%)6 (13%)36 (80%)16 (36%)7 (16%)11 (3%)176 (49%)60 (17%)14 (4%)0.005 < 0.0010.0050.029Radical prostatectomy203 (51%)15 (33%)188 (53%)0.021Lymph node removal146 (36%)16 (36%)130 (37%)1.000No. of lymph nodes removed17 ± 518 ± 1117 ± 81 (−6, 8)0.758No. of lymph node metastases2 (1, 3)1 (1,2)2 (1, 3)1 (0, 1)0.351ADT217 (54%)32 (71%)185 (52%)0.023Radiation therapy107 (27%)12 (27%)95 (27%)1.000Chemotherapy treatment69 (17%)9 (20%)60 (17%)1.000WW or AS**59 (15%)8 (14%)51 (14%)0.695N* number, SD standard deviation, Q1 25 th percentile, Q3 75 th percentile, 95% CI 95% confidence interval, BMI body mass index, Annual income annual income before tax in DKK, ADT androgen deprivation therapy, WW watchful waiting, AS active surveillance. *This question was introduced after the study had commenced, which explains the substantial amount of missing data
LLE
LLE was identified in 11% (n = 45) of participants (Supplementary file 1). Of these, 34 (76%) had unilateral LLE, while 11 (24%) had bilateral LLE.
Presence of LLE was significantly associated with older age (mean difference of 4 years; 95% CI: 2 to 6), obesity (BMI ≥ 30; 42% vs. 18%), and a history of self-reported swelling at pre-diagnosis (37% vs. 13%) (Table 1). Additionally, participants with LLE were less likely to undergo radical prostatectomy (33% vs. 53%), more likely to receive or had received ADT (71% vs. 52%), reported more often to have 3–5 comorbidities (18% vs. 7%). Comorbidities like heart failure, valvular disease, hypertension, and venous thrombosis were also more common in participants with LLE (p < 0.05).
The variables most strongly associated with LLE were identified using stepwise backward regression based on Akaike Information Criterion. Multivariate logistic regression identified that “quite a bit” or “very much” swelling before diagnosis had the strongest association with LLE (OR: 47, 95% CI: 7 to 453). Higher odds were also observed for heart failure (OR: 16, 95% CI: 3 to 87), self-reported metabolic diseases (OR: 16, 95% CI: 1 to 202), BMI ≥ 30 (OR: 7, 95% CI: 2 to 28), and having received ADT (OR 4, 95% CI: 1 to 12) No significant associations were found for age, radiotherapy, COPD or chronic bronchitis, or valvular heart disease (Supplementary file 2 and Table 2). Further, having > 20 lymph nodes removed was not a significant predictor (OR: 1.47, 95% CI: 0.28 to 6.14). Table 2. Variables that most strongly explain LLEOR****95% CIp**-value**Age1.11.0, 1.10.080BMI kg/m**^2^ < 25- 25–29.90.60.2, 2.20.4 ≥ 307.12.1, 27.80.003Radiation therapy No-- Yes0.30.1, 1.00.053Swelling before diagnosis Not at all-- A little1.000.3, 3.4 > 0.9 Quite a bit or very much47.37.3, 453 < 0.001ADT No-- Yes3.61.2, 11.50.023Metabolic diseases No- Yes16.11.3, 2020.025COPD or chronic bronchitis No-- Yes0.10.00, 1.30.092Heart failure No-- Yes16.13.3, 86.5 < 0.001Valvular heart disease No-- Yes2.40.9, 6.50.079OR odds ratio, CI 95% confidence interval, BMI body mass index, ADT androgen deprivation therapy, COPD chronic obstructive pulmonary disease. Variables included in this multivariate logistic regression were selected through stepwise backward regression as those most strongly associated with the likelihood of LLE (step 15), see supplementary file 2
Prevalence of LLE based on specific treatments
When examining the specific treatment combinations, it was observed that the prevalence of LLE was highest among patients whose only treatment was ADT (n = 10, 26%), ADT with radical prostatectomy with PLND (n = 3, 27%), ADT, radical prostatectomy with PLND, radiation therapy, and chemotherapy (N = 7, 28%) (Supplementary file Cite ESM.3). By contrast, 14% (n = 8) of participants who received watchful waiting or active surveillance had LLE. Notably, these individuals were also obese (n = 7) and/or had hypertension (n = 6) which can lead to LLE.
Relationship between LLE and HRQoL and depression
Patients with LLE were more likely to report lower scores in several HRQoL domains compared to those without LLE (Table 3), specifically in Global Health Status/QoL by − 12 (95% CI: − 19 to − 6), Physical Functioning − 13 (95% CI: − 20 to − 6), Role Functioning − 19 (95% CI: − 29 to − 9), and Social Functioning − 13 (95% CI: − 22 to − 4). Additionally, patients with LLE were more likely to report more severe bowel symptoms and hormonal treatment-related symptoms. These differences remained statistically significant after adjusting confounders. There was no difference in depression between the groups (Supplementary file 4). Table 3. Relationship between lower limb edema and health-related quality of lifeCrudep**-valueAdjusted model 1p-valueAdjusted model 2p-value****Difference of means (95% CI)**Difference of means (95% CI)**Difference of means (95% CI)EORTC-QLQ-C30 Global health status/QoL − 12 (− 19, − 6) < 0.001 − 10 (− 18, − 2)0.012 − 10 (− 18, − 2)0.018 Physical functioning − 13 (− 20, − 6) < 0.001 − 10 (− 17, − 4)0.007 − 10 (− 17, − 4)0.001 Role functioning − 19 (− 29, − 9) < 0.001 − 13 (− 22, − 4)0.001 − 12 (− 22, − 3)0.011 Social functioning − 13 (− 22, − 3.6) < 0.001 − 14 (− 22, − 5)0.002 − 13 (− 22, − 4)0.003 Cognitive functioning − 8 (− 15, − 1)0.034 − 7 (− 14, 1)0.072 − 6 (− 13, 1)0.102 Emotional functioning − 4 (− 11, 12)0.165 − 7 (− 13, − 1)0.027 − 6 (− 13, 0)0.041EORTC-QLQ-PR25 Urinary symptoms10 (3, 16)0.0064 (− 3, 11)0.2643 (− 4, 11)0.374 Incontinence5 (− 7, 17)0.3969 (− 2, 20)0.11212 (0, 23)0.056 Bowel symptoms6 (1, 12)0.0186 (2, 11)0.0097 (3, 12)0.002 Hormonal treatment-related symptoms10 (5, 15) < 0.0018 (3, 14)0.0057 (2, 13)0.010 Sexual activity − 6 (− 14, 3)0.1902 (− 10, 13)0.7954 (− 7, 15)0.501 Sexual functioning2 (− 8, 11)0.6826 (− 6, 19)0.3147 (− 6, 20)0.27495% CI 95% confidence intervalAdjusted Model I = linear regression adjusted for, age, body mass index (BMI), comorbidities associated with development of edema, self-reported comorbidities and swelling before diagnosisAdjusted Model II = linear regression adjusted for Adjusted model I + time since diagnosis, treatment (radical prostatectomy, chemotherapy, radiation therapy, androgen deprivation therapy (ADT), lymph node removal)
Impact of LLE on daily living
Of the 45 participants with LLE many reported that the LLE symptoms impacted essential daily activities (Fig. 2 and Supplementary file 5). This included their ability to get in and out of bed (n = 7, 16%), their sexual function (n = 6, 13%), sitting (n = 5, 11%), walking (n = 19, 42%), passing urine (n = 8, 18%), and choosing appropriate clothing or footwear (n = 18, 41%). Sixteen (36%) reported experiencing two or more of these challenges. Additionally, 9% (n = 4) of these participants required antibiotics for leg infections. Despite these challenges, 35 (78%) participants had not received advice or treatment for managing LLE symptoms, and 34 (76%) expressed a desire for more information on LLE.Fig. 2. The LLE symptoms are affecting
Discussion
This study represents the first investigation of the prevalence of LLE and its association with HRQoL, depression, and daily living among men with prostate cancer, using both BIS and patient-reported outcomes. We found an overall prevalence of 11% across various treatment modalities and stages of the disease. LLE was associated with lower HRQoL, increased treatment-related symptoms, and impairments to daily activities. However, no association between LLE and depression was observed. Moreover, presence of LLE was significantly associated with older age, higher BMI, more comorbidities, self-reported swelling in the lower limbs prior to diagnosis, and increased exposure to ADT.
Our findings align with results from other studies. A prospective observational study defining edema as self-reported swelling in the legs or ankles found that high BMI (> 30), a higher Charlson Comorbidity Index, and ADT significantly increased LLE risk after radiation therapy in 302 men with prostate cancer. However, only high BMI remaining significant in multivariate analysis [33]. Similarly, in our study, obesity was associated with a higher prevalence of LLE, with 80% of affected men classified as overweight or obese and 71% having ADT exposure. ADT can induce metabolic changes, including weight gain, which may further contribute to LLE risk [34, 35]. These findings underscore the importance of identifying potential underlying causes of LLE, including metabolic changes and weight gain, for which targeted interventions like exercise and diet programs are effective [36]. Moreover, we found that patients with LLE were less likely to undergo radical prostatectomy. Patients undergoing surgery are often in better overall health, while those with, e.g., metabolic disorders or comorbidities face higher surgical risks [37]. In our study, patients with LLE had more comorbidities, possibly explaining their ineligibility for surgery. However, further research is needed to confirm this.
When comparing prevalence for LLE across treatment modalities, substantial variability emerges. The highest prevalence in our study (26%) was observed among patients receiving ADT, a treatment typically reserved for older individuals with advanced or metastatic disease, who are at greater risk of developing edema [38]. A prospective observational study found a prevalence of 23% for self-reported moderate to severe lymphedema symptoms at a median of 15 months post-treatment among men receiving radiotherapy and ADT [33]. In comparison, we found a prevalence of LLE of 13% among patients who underwent radiotherapy and ADT.
Among a small subset of patients undergoing radical prostatectomy with PLND, we found a prevalence of LLE of 4%, which aligns with prevalence of 0–14% reported by a 2022 systematic review of 18 studies and 9223 men [1]. However, for patients treated with multiple therapies, including radical prostatectomy with PLND, radiation therapy, and ADT, the prevalence of LLE in our study was also 4%. This is substantially lower than the 18–29% prevalence reported in the systematic review for cases combining prostatectomy with radiotherapy [1]. However, the findings from our study are based on a small subset of patients receiving these treatments, and differences in methods for assessing may explain the difference. Notably, the systematic review highlights a significant limitation, as most included studies lacked definitions or description of how lymphedema was identified, with only one study using a standardized questionnaire for patient-reported symptoms [1]. In contrast, a cross-sectional study used both circumferential limb measurements and International Society of Lymphology staging criteria to define LLE among men treated with postoperative radiotherapy following radical prostatectomy ± PLND [39] and reported a prevalence of 13.9%. Interestingly, the study identified diabetes mellitus, low physical activity, and shorter time between surgery and radiotherapy as significant predictors of LLE [39]. While our study did not collect data on exercise habits or time between treatments, we similarly found strong associations between LLE and metabolic comorbidities such as heart failure and obesity. Moreover, both studies observed that the number of lymph nodes removed was not a significant predictor in multivariate models, suggesting that comorbidity burden and systemic effects of treatment may be more important than surgical extent alone.
These discrepancies illustrate the challenges of comparing LLE rates across studies, as variations in treatment regimens, disease stages, and assessment methods can all influence prevalence estimates. While patient-reported outcomes, clinical evaluations, and objective measurements provide valuable insights, they will yield varied results depending on the criteria and tools used.
Our analysis revealed that the presence of LLE was associated with lower HRQoL. Similarly, a survey-based study including 54 men with lymphedema following radical prostatectomy with PLND found that men with persistent lymphedema experienced significantly greater burdens in daily living compared to men whose lymphedema had resolved [17]. Likewise, a case–control study from Portugal including 12 men and 68 women found that individuals with lymphedema exhibited significantly higher levels of depressive symptoms, compared to controls, highlighting its psychological burden [16]. In contrast, our study found no difference in depression scores between patients with and without LLE. This discrepancy may be explained by the often higher prevalence of depression among women, as suggested by other studies [40]. However, these results highlight the relationship between LLE and physical and emotional burden, emphasizing the need for patient support.
Notwithstanding the recognized burden of LLE, our study revealed that 78% of participants with LLE had not received advice or treatment for managing their symptoms, and 76% expressed a need for more information. While we cannot ascertain whether participants received advice on managing underlying factors, such as lifestyle interventions to reduce the risk of metabolic syndrome, it remains crucial to address potential underlying causes of LLE to enable targeted and effective treatment. However, our findings indicate a substantial gap in patient education, leaving many to cope with the challenges of LLE without adequate guidance. Similarly, other studies have identified a lack of structured support for LLE management, where the condition is often described as the “forgotten vascular disease” or labeled as “under-recognized and under-treated” [1, 15, 41, 42]. This trend highlights a need for greater awareness, management, and support for LLE for men with prostate cancer.
In this study, we defined LLE prevalence as the presence of both self-reported symptoms and an L-Dex score > 10 using BIS. BIS is a widely used tool for detecting lymphedema, particularly in breast cancer care [43]. The L-Dex threshold of > 10 indicates LLE which is based on the normal distribution of L-Dex in a healthy population (mean + 3 SD) [44]. By including self-reported symptoms alongside objective measure, we ensured that the swelling was both clinically detectable and noticeable to participants. If we had relied solely on self-reported symptoms, the prevalence would have ranged from 17% to 46% potentially overestimating true prevalence, as swelling perception may be influenced by factors beyond physical changes in LLE [45]. While self-reported symptoms are moderately reliable, prior studies indicate that they are best complemented by highly reliable measurements like BIS [45]. Therefore, combining self-reports with BIS enhances overall accuracy and comprehensiveness of LLE assessment.
Strengths and limitations
The most important strength of this study is the large sample who underwent both objective and subjective assessments for a comprehensive evaluation of LLE. Yet, a key limitation is its cross-sectional design, which limits causal inference. Additionally, the absence of a control group without prostate cancer restricts differentiation between treatment-related and population-level risk factors. Although the analyses were adjusted for several variables, some confounders may not have been accounted for.
Conclusion
Among 401 men with prostate cancer, we found a prevalence of 11% for LLE. LLE was associated with lower HRQoL and impairment in daily living. Moreover, presence of LLE was significantly associated with older age, higher BMI, more comorbidities, self-reported swelling prior to diagnosis, and increased ADT exposure. Most participants expressed a desire for more information on how to manage their LLE symptoms. These findings highlight the importance of raising awareness, addressing treatable causes and providing support to improve HRQoL and functional outcomes. Well-designed prospective studies with baseline measurements before cancer treatment are needed to clarify how specific treatments affect LLE and to identify those at greatest risk.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1(JPG 53.3 KB)ESM 2(DOCX 23.9 KB)ESM 3(DOCX 14.8 KB)ESM 4(DOCX 13.7 KB)ESM 5(DOCX 15.5 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mortimer PS. The pathophysiology of lymphedema. Cancer. 1998 Dec 15;83(12 Suppl American):2798–802.10.1002/(sici)1097-0142(19981215)83:12b+<2798::aid-cncr 28>3.3.co;2-59874400 · doi ↗ · pubmed ↗
- 2Abassi Z, Khoury EE, Karram T, Aronson D. Edema formation in congestive heart failure and the underlying mechanisms. Front Cardiovasc Med [Internet]. 2022 Sep 27 [cited 2024 Nov 3];9. Available from: https://www.frontiersin.org/journals/cardiovascularmedicine/articles/10.3389/fcvm.2022.933215/full 10.3389/fcvm.2022.933215 PMC 955300736237903 · doi ↗ · pubmed ↗
- 3Meiklejohn JA, Heesch KC, Janda M, Hayes SC. How people construct their experience of living with secondary lymphoedema in the context of their everyday lives in Australia. Support Care Cancer. 20120718 th ed. 2013 Feb;21(2):459–66.10.1007/s 00520-012-1534-423010957 · doi ↗ · pubmed ↗
- 4Di Sipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 20130327 th ed. 2013 May;14(6):500–15.10.1016/S 1470-2045(13)70076-723540561 · doi ↗ · pubmed ↗
- 5Dylke ES, Schembri GP, Bailey DL, Bailey E, Ward LC, Refshauge K, et al. Diagnosis of upper limb lymphedema: development of an evidence-based approach. Acta Oncol. 20160622 nd ed. 2016 Dec;55(12):1477–83.10.1080/0284186 X.2016.119166827333213 · doi ↗ · pubmed ↗
- 6Jensen K, Bonde Jensen A, Grau C. A cross sectional quality of life study of 116 recurrence free head and neck cancer patients. The first use of EORTC H&N 35 in Danish. Acta Oncol. 2006 Jan 1;45(1):28–37.10.1080/0284186050041753616464793 · doi ↗ · pubmed ↗