Dynamic mitral regurgitation unmasked by handgrip exercise is linked with outcomes in (non-) dilated cardiomyopathy
Fabian Voß, Niklas Guenther, Lucas Christian, Elric Zweck, Jafer Haschemi, Christian Schulze, Ralf Westenfeld, Patrick Horn, Malte Kelm, Amin Polzin, Maximilian Spieker

TL;DR
This study shows that handgrip exercise can reveal hidden severe mitral regurgitation in patients with non-severe resting regurgitation, which may influence treatment decisions.
Contribution
The study identifies dynamic mitral regurgitation during handgrip exercise as a prognostic marker in non-ischemic cardiomyopathy patients.
Findings
26% of patients with non-severe MR at rest developed severe MR during handgrip exercise.
Dynamic MR was associated with larger left ventricular volumes and increased mitral annular diameter.
Patients with dynamic MR were more likely to undergo mitral valve surgery or interventions.
Abstract
Recent studies suggest that secondary mitral regurgitation (MR) is a dynamic condition influenced by global and regional left ventricular (LV) remodeling as well as by mitral valvular deformation. Exercise testing is crucial in assessing the hemodynamic relevance of MR and is recommended by current guidelines. However, data are still lacking on the prevalence and prognostic impact of dynamic MR in patients with non-ischemic cardiomyopathy. We aimed to assess the prevalence, hemodynamic consequences, and prognostic impact of exercise-induced changes in patients with MR and hypokinetic non-dilated and dilated cardiomyopathy. Patients with hypokinetic non-dilated and dilated cardiomyopathy and at least mild MR who underwent handgrip echocardiography at the University Hospital Duesseldorf between January 2018 and September 2021 were enrolled. Follow-up was performed at one year.…
Click any figure to enlarge with its caption.
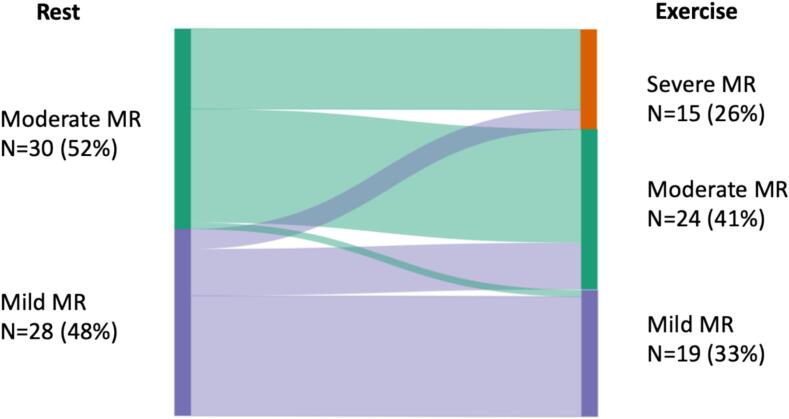 Figure 1
Figure 1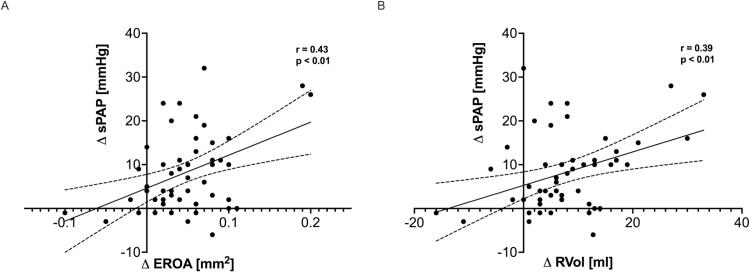 Figure 2
Figure 2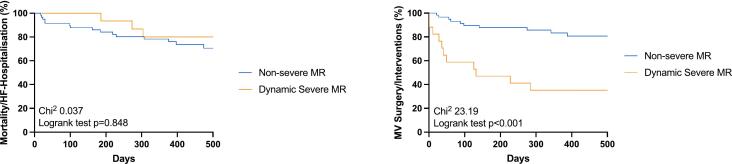 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair · Cardiovascular Function and Risk Factors
Introduction
1
Non-ischemic cardiomyopathy represents a complex and heterogeneous group of heart diseases characterized by structural and functional abnormalities of the myocardium, often leading to progressive heart failure. Dilated cardiomyopathy (DCM) and hypokinetic non-dilated cardiomyopathy (HNDCM) represent the most common etiologies. Among the various pathological mechanisms contributing to the deterioration of cardiac function in DCM and HNDCM, mitral regurgitation (MR) has emerged as a critical factor warranting clinical attention [1]. Conventionally, the assessment of MR severity has relied on resting echocardiography, which may not fully capture the dynamic and exercise-induced changes in MR contributing to patient reported symptoms and clinical outcomes. Previous studies have demonstrated the prognostic benefit of bicycle exercise testing in patients with primary and secondary MR [2,3]. Thus, current guidelines recommend exercise testing in various clinical scenarios in patients with valvular heart disease [4,5].
Isometric handgrip exercise represents an alternative exercise modality that can be performed fast without the need of an ergometer [6,7]. Until now, there are no data on the prognostic impact of dynamic MR in patients with DCM and HNDCM. We hypothesized that handgrip exercise during echocardiography may unmask dynamic MR in a significant proportion of patients, which could potentially alter therapeutic decision-making. In this regard, we aim to assess the prevalence, hemodynamic consequences and prognostic impact of dynamic MR in patients with DCM and HNDCM.
Methods
2
Study population
2.1
Consecutive patients undergoing exercise echocardiography at the university hospital Duesseldorf, Germany were enrolled between 2018 and 2021. In all patients, echocardiography at rest and during standardized handgrip exercise was performed. Exercise echocardiography was performed in heart failure patients with DCM and HNDCM, when there was a discrepancy between symptoms and echocardiographic findings at rest, rising the suspicion of a dynamic component. Only patients with reduced left ventricular ejection fraction (LVEF) < 50 %, and at least mild MR at rest were included. In patients with concomitant coronary artery disease significant coronary stenosis was excluded by coronary angiography. Patients with prior coronary intervention or myocardial infarction were excluded. The study was approved by the ethics committee of the Heinrich-Heine University Duesseldorf (No. 2018-117_1) and executed in accordance with the Declaration of Helsinki.
Echocardiographic examinations
2.2
Echocardiographic examinations were performed using a GE Vivid E90 (Chicago, Illinois, United States). All echocardiographic data were obtained in digital form and stored on a workstation for offline analysis (IntelliSpace Cardiovascular, Version 3.2, Philips). Assessment of MR was performed according to current ESC guidelines [5]. An integrative approach using semi-quantitative and at least one quantitative parameter was used to assess the severity of MR, which was graded mild, moderate or severe. Non-ischemic MR was defined in patients with known DCM and HNDCM with the mitral valve itself remaining intact (Carpentier class I). DCM and HNDCM were defined according to the recent ESC recommendations [8]. Mitral annulus was measured at end-diastole in the parasternal long-axis view and in apical four chamber view and then averaged. Mitral valve (MV) tenting was measured using established MV tenting parameters (tenting area; tenting height) and assessed in the parasternal long axis view during mid-systole according to the recommendations of the American Society of Echocardiography [9].
Left and right ventricular volumes and function were assessed according to current recommendations. Systolic pulmonary artery pressure (SPAP) was estimated from the regurgitant jet of tricuspid regurgitation (TR) with peak systolic trans-tricuspid pressure gradient (TTPG) calculated by the modified Bernoulli equation.
Isometric handgrip testing
2.3
Following echocardiographic examination at rest, handgrip exercise was conducted according to a standardized protocol with a handgrip dynamometer (Jamar® Hydraulic Hand Dynamometer, Sammons Preston Inc.). The patient lays on his left side during the whole examination and pushes the handgrip dynamometer with one hand. To assess maximal handgrip strength, the patient was asked to push the dynamometer with maximum effort. Then handgrip exercise was carried out at 30 % force for three to five minutes while the patient laid on his left side [10]. Echocardiographic images were obtained after two minutes of exercise until peak exercise. Blood pressure and heart rate were recorded at rest and during peak exercise. Medical therapy (including ß-blockers) remained unchanged for the exercise test.
Follow-up
2.4
The clinical course of patients was assessed by follow-up examinations and phone calls to the referring cardiologists, primary physicians, or the patients themselves. We assessed a composite of all-cause mortality, HF-associated hospitalizations, MV surgery, transcatheter edge-to-edge repair (TEER), left ventricular assist device implantation and heart transplantation during follow-up as the combined endpoint.
Statistical analysis
2.5
Percentages were reported to describe categorical variables and median with interquartile range or mean ± standard deviation was reported for continuous variables. Normality distribution of continuous variables was assessed with the Kolmogorov-Smirnov Test. Comparison between two groups were performed using the chi-square test (or Fisher’s exact test if the expected count was less than five per cell) for categorical variables. Differences in continuous variables between two groups were compared for significance with a two-tailed paired t test. Kaplan-Meier analysis was used to evaluate the event-free rate. Cox regression analysis was used to test for correlations between continuous variables and outcomes. For all analyses, p-values of < 0.05 were considered to be statistically significant. All analyses were performed using Sigma Plot (Version 11.0; Systat Software Ltd. Inpixon GmbH, Duesseldorf, Germany) and GraphPad Prism (Version 7; Graphpad Software, San Diego, California, USA).
Results
3
Study population
3.1
We screened 539 patients that underwent echocardiography at rest and during handgrip exercise. After excluding 94 patients (because of image quality (n = 50); handgrip exercise physically not feasible (n = 22); severe aortic stenosis (n = 2); severe mitral stenosis (n = 1), previous mitral valve repair (n = 19)) the study cohort included 445 patients. Fifty-eight out of these patients had DCM or HNDCM with at least mild MR and were included in final analysis. Patient characteristics are presented in Table 1. Mean age was 73 (IQR 65–81) years, 41 % were female. Mean LVEF was 37 ± 9 %. In this regard, 43 patients (74 %) presented with HFmrEF, and 15 patients (26 %) presented with HFrEF. Twenty-six patients (45 %) had HNDCM and 32 patients (55 %) were diagnosed with DCM.Table 1. Baseline patient characteristics.DemographicsAll PatientsN = 58 (100.0)Sex female, n (%)24 (41.4)BMI (kg/m^2^)26.5 (23.1–29.4)Age (years)73 (65–81)Diabetes Mellitus, n (%)12 (20.1)Hypertension, n (%)34 (58.6)Smoking, n (%)12 (20.1)DCM, n (%)32 (55.2 %)HNDCM, n (%)26 (44.8 %)CAD, n (%)25 (43.0)History of MI, n (%)0 (0.0)History of PCI, n (%)0 (0.0)History of CABG, n (%)0 (0.0)History of VS, n (%)2 (3.5)Pacemaker, n (%)4 (6.9)ICD, n (%)12 (20.7)CRT, n (%)11 (19.0)NYHA 1, n (%)5 (8.6)NYHA 2, n (%)17 (29.3)NYHA 3, n (%)36 (62.1)Atrial Fibrillation, n (%)31 (53.5)Medicationß-Blocker, n (%)52 (89.7)ACE-I/AT-1 Blocker, n (%)33 (56.9)Aldosteron Antag., n (%)33 (56.9)Sacubitril/Valsartan, n (%)18 (31.0)Diuretic, n (%)59 (84.5)Laboratory MarkersSerum Creatinine (mg/dl)1.3 (1.0–1.5)eGFR (mg/dl/1.73 m^2^)53 (39–74)Hemoglobin (mg/dl)13.2 (11.7–14.8)NT-proBNP (ng/ml)4347 (1590–8549)Abbreviations: BMI = body mass index; CAD = coronary artery disease; MI = myocardial infarction; PCI = percutaneous coronary intervention; CAGB = coronary artery bypass grafting; VS = valve surgery; ICD = internal cardiac defibrillator; CRT = cardiac resynchronization therapy; eGFR = estimated glomerular filtration rate; NT-proBNP=N-terminal pro brain natriuretic peptide.
Echocardiographic parameters at rest and during exercise
3.2
Twenty-eight patients (48 %) presented with mild MR, and 30 patients (52 %) had moderate MR (41 %) at rest. Detailed data of mitral valve parameters were shown in Table 2. Forty-three percent of patients presented with concomitant moderate to severe TR. Mean SPAP was 41 ± 10 mmHg.Table 2. Echocardiographic parameters at rest and during handgrip exercise.VariableRestExercisep-ValueHeart Rate (bpm)78 ± 1495 ± 24**<0.001Systolic BP (mmHg)113 ± 23127 ± 24<0.001Diastolic BP (mmHg)67 ± 1777 ± 190.002RPP (mmHg*bpm)8766 ± 231112040 ± 3930<0.001LAVi (ml/m^2^)51 ± 1852 ± 210.899LVEDVi (ml/m^2^)90 ± 3892 ± 410.788LVESVi (ml/m^2^)59 ± 3561 ± 320.565LVSVi (ml/m^2^)30 ± 1230 ± 130.762LVEF (%)37 ± 936 ± 120.222LV Sphericity Index1.42 ± 0.231.49 ± 0.190.059LV Forward Flow Index (ml/m^2^)31 ± 1228 ± 100.302Cardiac Index (l/min/m^2^)2.3 ± 1.02.8 ± 1.40.048SVR (dynseccm^−2^)1530 ± 6481450 ± 5260.690RAVi (ml/m^2^)42 ± 1942 ± 190.783RVEDDi (mm/m^2^)22 ± 422 ± 40.243TAPSE (mm)19 ± 618 ± 60.262FAC (%)34 ± 1035 ± 120.972SPAP (mmHg)41 ± 1048 ± 12<0.001Mitral Regurgitation<0.001** Mild, n (%)28 (48.3)15 (32.8) Moderate, n (%)30 (51.7)24 (41.1) Severe, n (%)019 (25.9)Vena Contracta (mm)5.2 ± 1.46.0 ± 1.70.017MR EROA (mm^2^)16.0 ± 6.021.1 ± 8.8**<0.001MR Vol (ml)25 ± 933 ± 13<0.001Annulus Diameter (mm)39.3 ± 4.340.0 ± 4.50.372Tenting Height (mm)9.5 ± 2.310.3 ± 3.20.034Tenting Area (cm^2^)2.5 ± 0.92.8 ± 1.00.045**Tricuspid Regurgitation0.603 No TR, n (%)1910.5 Mild, n (%)37.942.1 Moderate, n (%)3136.8 Severe, n (%)12.110.5Abbreviations: BP = blood pressure; RPP = rate pressure product; LAVi = left atrial volume index; LVEDVi = left ventricular end-diastolic volume index; LVESVi = left ventricular end-systolic volume index; LVEF = left ventricular ejection fraction; LVSVi = left ventricular stroke volume index; RAVi = right atrial volume index; RVEDDi = right ventricular end-diastolic diameter index; TAPSE = tricuspid annular plane systolic excursion; FAC = fractional area change; SPAP = systolic pulmonary artery pressure; EROA = effective regurgitant orifice area; Vol = volume; IPM Distance = interpapillary muscle distance; TR = tricuspid regurgitation.
Isometric handgrip exercise led to a meaningful hemodynamic response: heart rate, systolic and diastolic blood pressure, and rate pressure product increased (all p < 0.05, Table 2). This was accompanied by a re-classification of MR severity in 22 patients (38 %) (Fig. 1). Fifteen patients (26 %) with non-severe MR at rest, developed dynamic severe MR during exercise (Fig. 1). Of these patients, six patients (40 %) had HNDCM and nine patients (60 %) had DCM. In the overall cohort, there was an increase in cardiac index (+0.5 ± 1.3 l/min/m^2^; p = 0.048) that was caused by an increase in heart rate (+17 ± 20/min; p < 0.001), and not by LV forward flow (−2 ± 12 ml/m^2^; p = 0.302), while RV volumes and function did not change. SPAP increased by 7 ± 12 mmHg from rest to exercise. Detailed changes of echocardiographic parameters from rest to exercise were shown in Table 2.Fig. 1. Distribution of MR severity at rest and during handgrip exercise. Abbreviations: MR = mitral regurgitation.
Mechanisms and hemodynamic consequences of dynamic MR
3.3
Patients with dynamic severe MR had larger mitral annulus diameter at rest, while LA volume (LAVi) also tended to be larger (Table 3). In line with this, LV volumes (LVEDVi and LVESVi) at rest were numerically larger in patients with dynamic severe MR compared to those with non-severe MR (Table 3). There was no difference in pulmonary pressures (SPAP), right heart dimensions and function between the groups (Table 3).Table 3. Echocardiographic parameters at rest according to MR severity.VariableNon-severe MR(N = 43)Dynamic Severe MR (N = 15)p-ValueHeart Rate (bpm)79 ± 1575.2 ± 11.10.37Systolic BP (mmHg)112 ± 24.2117 ± 20.50.47Diastolic BP (mmHg)66.3 ± 13.770.4 ± 23.30.42RPP (mmHgmin^−1^)8763 ± 24328775 ± 20100.99LAVi (ml/m^2^)48.5 ± 16.857.9 ± 20.40.13LVEDVi (ml/m^2^)86.8 ± 39.1107 ± 42.80.08LVESVi (ml/m^2^)54.6 ± 33.672.3 ± 34.80.07LVSVi (ml/m^2^)29.6 ± 12.631 ± 10.30.71LVEF (%)37.6 ± 1025.9 ± 9.60.56Forward LVSVi ((ml/m^2^)30.4 ± 11.831.5 ± 140.91Cardiac Index (l/min/m^2^)2.4 ± 12.4 ± 1.10.97SVR (dynsec*cm^−5^)1576 ± 7041400 ± 4500.62RAVi (ml/m^2^)40.1 ± 2045.8 ± 17.60.34RVEDDi (mm/m^2^)21.4 ± 4.223 ± 60.27TAPSE (mm)18.6 ± 6.318.3 ± 4.90.9FAC (%)34.9 ± 10.231.2 ± 10.60.66SPAP (mmHg)40.6 ± 9.743.3 ± 10.30.39Mitral Regurgitation0.015Mild, n (%)26 (59.1)3 (20.0)Moderate, n (%)17 (40.9)12 (80.0)Severe, n (%)00MR Vena Contracta (mm)4.9 ± 1.46.2 ± 10.004MR EROA (mm^2^)0.14 ± 0.050.21 ± 0.06**< 0.001MR Vol (ml)21.9 ± 6.9734.3 ± 7.39< 0.001Annulus Diameter (mm)38.5 ± 4.441.6 ± 3.30.01**AML Length (mm)29.5 ± 5.630.3 ± 4.10.64PML Length (mm)17.2 ± 4.817.7 ± 2.90.7Leaflet-to-Annulus Index1.21 ± 0.211.16 ± 0.190.45Tenting Height (mm)9.3 ± 2.510.1 ± 1.30.23Tenting Area (cm^2^)2.38 ± 0.92.85 ± 0.80.1TR Grade (n)0.56No TR, n (%)23.36.7Mild, n (%)34.946.7Moderate, n (%)30.233.3Severe, n (%)11.613.3Abbreviations: Please see Table 2.
During exercise, LVEDVi (113 ± 51 ml/m^2^ vs. 81 ± 28 ml/m^2^; p = 0.005) and LVESVi (80 ± 28 ml/m^2^ vs. 54 ± 24 ml/m^2^; p = 0.006) were increased in patients with dynamic severe MR compared to those with non-severe MR. Similarly, mitral annulus diameter (42 ± 3.7 mm vs. 39.3 ± 4.6 mm; p = 0.076) as well as tenting area (3.3 ± 0.9 cm^2^ vs. 2.5 ± 0.9 cm^2^; p = 0.052) and tenting height (12.5 ± 2.9 mm vs. 9.2 ± 2.8 mm; p = 0.005) were larger in patients with dynamic severe MR.
There was no difference in LV forward flow and cardiac index between the groups during exercise. Patients with dynamic severe MR showed increased exercise SPAP compared to those without, while RV dimensions and function were similar between both groups. Furthermore, the increase in MR severity (by effective regurgitation orifice area (EROA) and regurgitation volume (RVol)) correlated with the change in SPAP (Fig. 2).Fig. 2. Association between changes from rest to exercise in MR severity (assessed by (A) EROA and (B) RVol) and pulmonary pressures (SPAP). Abbreviations: SPAP = systolic pulmonary artery pressure; EROA = effective regurgitant orifice area; RVol = regurgitation volume.
Clinical outcomes according to the presence of dynamic MR
3.4
One-year follow-up (median 442 (334–691) days) was completed in all patients (100 %). Thirty-eight patients (66 %) experienced the combined endpoint: three patients died (5 %), 14 patients (24 %) were re-admitted to hospital due to heart failure symptoms, 17 patients (29 %) underwent MV TEER, one patient (2 %) received MV surgery, two patients (3 %) underwent LVAD implantation, and one patient (2 %) underwent heart transplantation. There was no difference in the combined endpoint of all-cause mortality and heart-failure hospitalizations regarding patients with non-severe MR and patients with dynamic severe MR (Chi^2^ 0.037; log-rank test p = 0.85) (Fig. 3A). As expected, patients with dynamic severe MR more often underwent MV surgery/interventions compared to patients with non-severe MR (Chi^2^ 23.19; log-rank test p < 0.001) (Fig. 3B). Cox regression analysis was used to analyze the relationship between the change in EROA/RVol during exercise and clinical outcomes. The change in EROA/RVol was correlated with MV surgery/ interventions (ΔEROA: HR 1.145 (1.051–1.387), p < 0.001; ΔRVol: HR 1.098 (1.045–1.151), p < 0.001), but not with mortality and heart failure hospitalizations (ΔEROA: HR 1.022 (0.928–1.105), p = 0.631; ΔRVol: HR 1.016 (0.955–1.079), p = 0.612). As explorative analyses, the incidence of the combined endpoint was calculated and was less frequently observed in patients who underwent MV surgery/TEER compared to those who did not: three out of 18 patients (16.7 %) who underwent MV surgery/TEER experienced an adverse event compared to 11 out of 38 patients (29.0 %) of those patients who did not receive MV surgery/TEER (Chi^2^ 1.167; log-rank test p = 0.280).Fig. 3. Kaplan-Meier survival analysis regarding combined events (A), and MV surgery/interventions (B) in patients with and without dynamic severe MR. Abbreviations: MR = mitral regurgitation; MV = mitral valve.
Discussion
4
In this study, we evaluated the role of exercise echocardiography for the assessment of dynamic MR in patients with DCM and HNDCM. We demonstrated 1.) that handgrip exercise unmasks dynamic severe MR in one out of four patients with non-severe MR at rest; 2.) that dynamic severe MR was associated with global and regional adverse LV remodeling during exercise; and 3.) that dynamic severe MR was associated with increased rates of MV surgery/interventions during follow-up compared to those with non-severe MR.
Prevalence of dynamic MR
4.1
Until now, studies investigating the role of exercise testing in patients with DCM and HNDCM for the assessment of dynamic MR remain scarce. D'Andrea et al. reported an increase in MR severity in 78 % of patients focusing on bicycle exercise testing [11]. Yamano et al. demonstrated an increase in MR severity in 23 of 32 patients with DCM. This is the first study yet, investigating the role of dynamic MR in patients with DCM and HNDCM using isometric handgrip exercise [12]. Here, we could demonstrate that 26 % of patients with non-severe MR at rest developed dynamic severe MR during exercise. Furthermore, in our study handgrip testing led to a re-classification of MR severity in 38 % of patients. Our results highlight the benefit of the addition of exercise echocardiography to echocardiography at rest in patients with DCM and HNDCM. Symptomatic patients with dynamic severe MR may benefit from intensified HF medication or early interventional strategies [13].
Mechanisms and hemodynamic consequences of dynamic MR
4.2
Predictors of exercise-induced increases in MR severity unmasked by dynamic bicycle exercise have been studied before [11,12]: an increase in EROA was associated with the enlargement of tenting area. Furthermore, the increase in LV dyssynchrony during exercise correlated with the increase in MR severity during exercise. This is the first study investigating the pathophysiological mechanisms of changes in MR provoked by isometric handgrip exercise in patients with DCM and HNDCM. While dynamic bicycle exercise leads to a decrease in afterload, an increase in contractility and venous return (increase in preload), that together may affect an increase in stroke volume, isometric handgrip exercise predominantly causes an increase in afterload. These different loading conditions may translate into different LV geometric changes during exercise, and precipitate exercise-induced changes in MR severity [6]. In the current study, mitral annular dimensions and LV volumes were associated with dynamic severe MR during exercise. Moreover, the change in MR severity was directly associated with the change in tenting area. Thus, both, regional and global LV remodeling seem to be responsible for worsening of MR during exercise. Future studies comparing both exercise modalities are necessary to further elucidate these findings. Isometric handgrip exercise causes an increased backward transmission and leads to a pressure load on the pulmonary circulation, that was more advanced in patients with dynamic severe MR (SPAP + 13 ± 10 mmHg) compared to those with non-severe MR (SPAP + 6 ± 8 mmHg) (Table 4). Moreover, there was a correlation between the change in MR severity from rest to exercise and the change in pulmonary pressures (Fig. 2). This may explain symptoms in patients with a discrepancy between symptoms and echocardiographic findings at rest.Table 4. Exercise changes in echocardiographic parameters according to MR severity.VariableNon-severe MR(N = 43)Dynamic Severe MR (N = 15)p-ValueΔHeart Rate (bpm)16.4 ± 22.517.1 ± 11.90.43Δ Systolic BP (mmHg)12.9 ± 13.515.5 ± 10.10.38Δ Diastolic BP (mmHg)8.8 ± 14.88.7 ± 7.90.6Δ RPP (mmHgmin^−1^)3177 ± 31683407 ± 23200.51Δ LAVi (ml/m^2^)0.65 ± 16.80.47 ± 11.60.97Δ LVEDVi (ml/m^2^)−2.35 ± 19.45.59 ± 25.80.58Δ LVESVi (ml/m^2^)2.46 ± 17.37.44 ± 19.30.99Δ LVSVi (ml/m^2^)−1.94 ± 11.73.48 ± 18.90.21Δ LVEF (%)−1.17 ± 11− 3.35 ± 9.10.52Δ Forward LVSVi ((ml/m^2^)−4.97 ± 7.76−1.2 ± 9.750.24Δ Cardiac Index (l/min/m^2^)0.29 ± 1.20.37 ± 0.620.46Δ SVR (dynsec*cm^−5^)140 ± 522−117 ± 3370.2Δ RAVi (ml/m^2^)1.2 ± 14.3−3.7 ± 9.50.22Δ RVEDDi (mm/m^2^)0.49 ± 30.61 ± 5.80.38Δ TAPSE (mm)−0.22 ± 4.470.36 ± 3.540.67Δ FAC (%)0.46 ± 10.72 ± 8.850.7Δ SPAP (mmHg)6.3 ± 7.612.9 ± 10.10.02ΔΔ MR Vena Contracta (mm)0.69 ± 1.330.9 ± 1.470.66Δ MR EROA (mm^2^)0.038 ± 0.050.087 ± 0.048**<0.001Δ MR Vol (ml)5.55 ± 7.0414.5 ± 10.2<0.001Δ Annulus Diameter (mm)0.8 ± 2.760.09 ± 3.570.98Δ Tenting Height (mm)−0.06 ± 1.832.35 ± 2.10.009**Δ Tenting Area (cm^2^)0.14 ± 0.590.51 ± 0.730.16Abbreviations: Please see Table 2.
Impact of exercise echocardiography on outcomes
4.3
In our cohort, there was no difference in clinical outcomes regarding the combined endpoint in patients with non-severe MR and patients with dynamic severe MR. However, exercise echocardiography unmasks a substantial proportion of patients (26 %) with non-severe MR at rest and dynamic severe MR during exercise. The recently published RESHAPE HF II trial showed improved outcomes after TEER in moderate to severe MR. [14] In contrast, former trials suggested only patients with severe (disproportionate) MR to benefit from MV interventions [15,16]. Dynamic MR maybe a partial explanation to these results, and therefore, exercise testing, may help to clarify this controversial issue in future randomized trials. As expected, MV surgery/intervention occurred more frequently during follow-up in patients with dynamic severe MR compared to the other group (Fig. 3b). Importantly, surgeons and interventionalists were not blinded to the results of exercise testing. Nevertheless, all patients were discussed within the local heart team and, therefore, all aspects of echocardiographic results, hemodynamics and patients’ symptoms were considered. Interestingly, patients who underwent MV surgery/intervention exhibited improved clinical outcomes compared to patients who did not. Although, randomized trials are needed to confirm this assumption, these results are in line with previous findings from Li et al. who investigated 112 patients with non-ischemic cardiomyopathy and significant MR [17]. They found that MV surgery/interventions were associated with better survival rates and lower HF hospitalizations compared to patients that were treated conservatively. In another study by Takeda et al., MV surgery led to LV reverse remodeling and the extent of reverse remodeling was related to mid-term mortality [18]. Together, there are only a few data on the prognostic importance of MV surgery/interventions in patients with DCM and HNDCM. This is the first study that demonstrated an incremental diagnostic value of isometric handgrip testing over echocardiography at rest in patients with DCM and HNDCM. However, since outcomes of patients with and without dynamic severe MR did not differ in our cohort, the prognostic impact of dynamic severe MR cannot be proven from this analysis alone, also the prognostic impact may have been diminished by early interventions among symptomatic patients. Further studies are warranted that randomize patients to additional exercise testing to further elucidate the role of exercise echocardiography in this patient cohort, before a widespread use of exercise testing can be recommended.
Limitations
4.4
Main limitation of the current study is that patients were not randomized to exercise testing. Thus, there might be a selection bias for patients undergoing MV surgery/interventions. In addition, exercise echocardiography was performed in patients with suspicion of a dynamic component that may have led to a selection bias since there was concern for dynamic MR that led to the exercise test being ordered and inclusion in the study. Cardiologists and cardiac surgeons were not blinded to the results of the exercise tests, thus, the decision for surgery/intervention might be by part influenced by the results of exercise echocardiography. Whether MV surgery/intervention among these patients has impact on patients’ outcomes in this specific cohort needs further investigation in randomized trials. That is why analyses of the combined endpoint after MV surgery/intervention can only be seen explorative and hypothesis-generating. Due to the relatively small sample size in our cohort, the prognostic value of isolated dynamic severe MR needs further validation e.g. in randomized trials or at least sensitivity analyses, which are of questionable value in this context since multiple – in part unknown factors – may influence patients‘ outcomes in this cohort.
Conclusions
5
Our results demonstrate that exercise echocardiography unmasks dynamic severe MR in a substantial proportion of DCM and HNDCM patients with non-severe MR at rest. MR severity during exercise was associated with MV surgery/interventions during follow-up. In addition, our results suggest the hypothesis that MV surgery/interventions are associated with improved clinical outcomes in patients with dynamic severe MR compared to those who are treated conservatively, but randomized clinical trials are needed to confirm this hypothesis. Thus, handgrip exercise might be a useful tool in symptomatic patients with suspicion of dynamic severe MR to help guiding further therapeutic decision making.
CRediT authorship contribution statement
Fabian Voß: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Niklas Guenther: Writing – review & editing, Visualization, Validation, Methodology, Formal analysis, Data curation, Conceptualization. Lucas Christian: Writing – review & editing, Visualization, Methodology, Formal analysis, Data curation. Elric Zweck: Writing – review & editing, Visualization, Validation, Supervision, Conceptualization. Jafer Haschemi: Writing – review & editing, Supervision, Resources, Project administration, Investigation, Formal analysis, Conceptualization. Christian Schulze: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Conceptualization. Ralf Westenfeld: Writing – review & editing, Writing – original draft, Validation, Supervision, Project administration, Investigation, Formal analysis, Conceptualization. Patrick Horn: Writing – review & editing, Visualization, Validation, Supervision, Resources, Methodology, Investigation, Conceptualization. Malte Kelm: Writing – review & editing, Writing – original draft, Visualization, Validation, Funding acquisition, Conceptualization. Amin Polzin: Writing – review & editing, Writing – original draft, Validation, Supervision, Project administration, Methodology, Funding acquisition, Data curation, Conceptualization. Maximilian Spieker: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Japp A.G.Gulati A.Cook S.A.Cowie M.R.Prasad S.K.The diagnosis and evaluation of dilated cardiomyopathy J. Am. Coll. Cardiol.6720162996301010.1016/j.jacc.2016.03.59027339497 · doi ↗ · pubmed ↗
- 2Bertrand P.B.Schwammenthal E.Levine R.A.Vandervoort P.M.Exercise dynamics in secondary mitral regurgitation: pathophysiology and therapeutic implications Circulation 135201729731410.1161/CIRCULATIONAHA.116.02526028093494 PMC 5245732 · doi ↗ · pubmed ↗
- 3Coisne A.Aghezzaf S.Galli E.Prognostic values of exercise echocardiography and cardiopulmonary exercise testing in patients with primary mitral regurgitation Eur. Heart J. Cardiovasc. Imaging 2320221552156110.1093/ehjci/jeab 23134751769 · doi ↗ · pubmed ↗
- 4Otto C.M.Nishimura R.A.Bonow R.O.2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines Circulation 1432021 e 35e 7110.1161/CIR.000000000000093233332149 · doi ↗ · pubmed ↗
- 5Vahanian A.Beyersdorf F.Praz F.2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Rev Esp Cardiol (Engl Ed)75202252410.1016/j.rec.2022.05.00635636831 · doi ↗ · pubmed ↗
- 6Kagiyama N.Toki M.Yuri T.Physiological and prognostic differences between types of exercise stress echocardiography for functional mitral regurgitation Open Heart 8202110.1136/openhrt-2021-001583 PMC 807086733888592 · doi ↗ · pubmed ↗
- 7Spieker M.Sidabras J.Lagarden H.Prevalence and prognostic impact of dynamic atrial functional mitral regurgitation assessed by isometric handgrip exercise Eur. Heart J. Cardiovasc. Imaging 25202458959810.1093/ehjci/jead 33638066677 · doi ↗ · pubmed ↗
- 8Pinto Y.M.Elliott P.M.Arbustini E.Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC working group on myocardial and pericardial diseases Eur. Heart J.3720161850185810.1093/eurheartj/ehv 72726792875 · doi ↗ · pubmed ↗