Eosinophilic angiocentric fibrosis: A case report and a review of the literature
Jood K. Alotaibi, Raghad A. Alkhaldi, Naif H. Alotaibi, R.M. Mumtaz, M. Anas Dababo

TL;DR
This paper reports a rare case of Eosinophilic Angiocentric Fibrosis (EAF) and reviews the literature to highlight diagnostic features and management challenges.
Contribution
The paper contributes a detailed case report of EAF involving multiple anatomical regions and emphasizes the importance of histopathological diagnosis.
Findings
EAF is diagnosed by the characteristic 'onion-skin' pattern of perivascular eosinophil-rich inflammation and fibrosis.
Medical and surgical interventions are used for EAF, but no standardized treatment guidelines exist.
A thorough diagnostic approach, including imaging and histopathology, is essential due to the condition's varied presentation.
Abstract
Eosinophilic Angiocentric Fibrosis (EAF) is a rare inflammatory condition affecting the upper respiratory and sinonasal tracts. This study aims to elaborate on the clinical and pathological features of a patient with extensive, rare EAF involving the sinonasal tract, subglottic region, and orbit. A fifty-five-year-old female patient with a known case of bronchial asthma, hypothyroidism, and IgG-4-related necrotizing blepharitis presented to our clinic with a 14-year history of bilateral nasal obstruction and post-nasal drip despite medical and surgical intervention. Rhinoscopy revealed fibrosis and adhesion of the nasal cavity and nasopharynx, along with grade I subglottic stenosis. Functional endoscopic sinus surgery was performed to relieve her symptoms and obtain a specimen confirming the diagnosis of EAF. Given the wide variety of differential diagnoses for bilateral nasal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
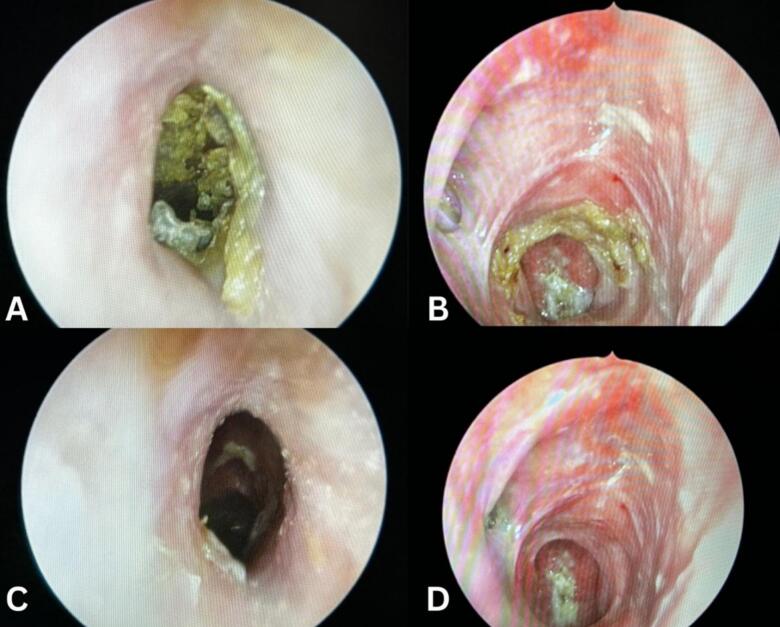 Figure 1
Figure 1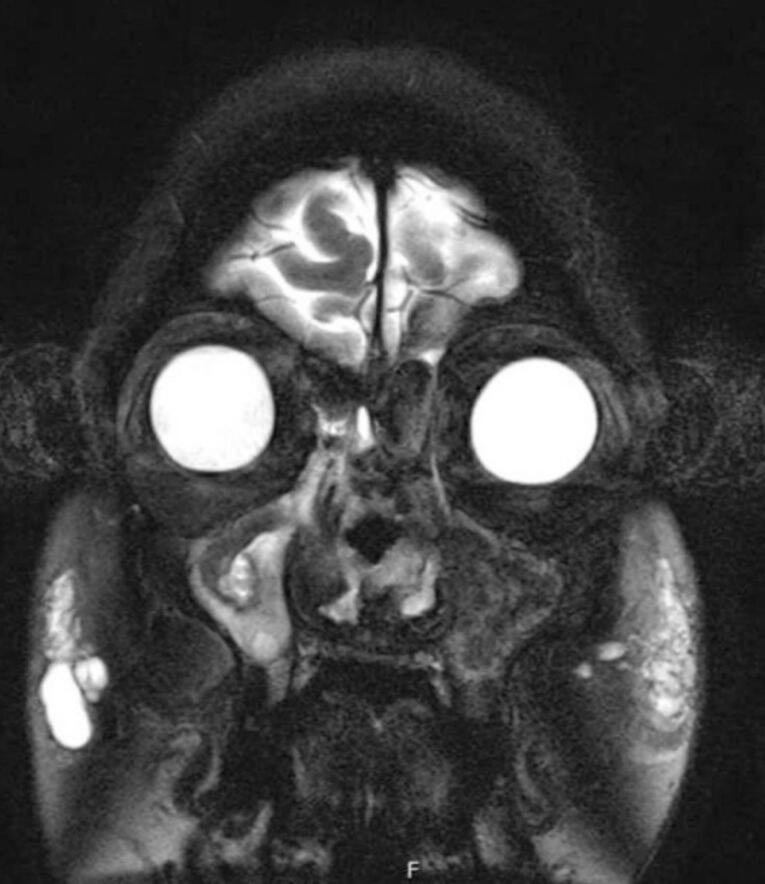 Figure 2
Figure 2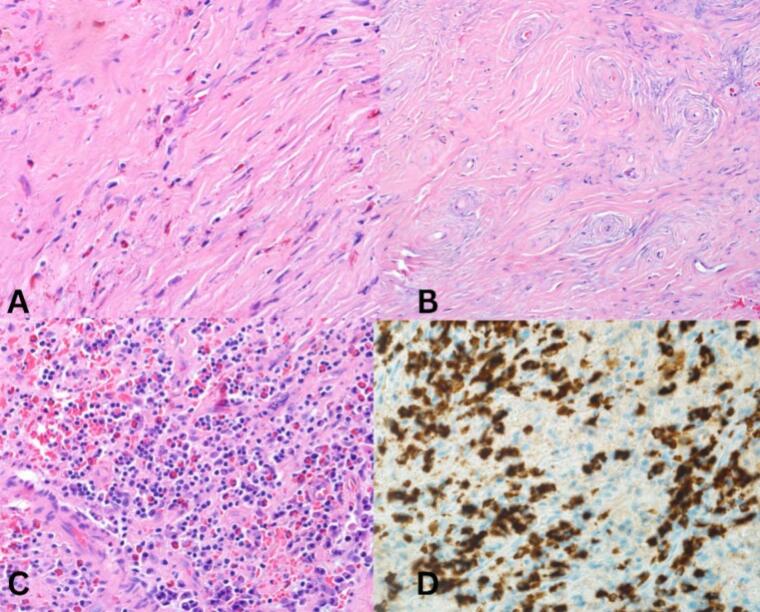 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders · Eosinophilic Disorders and Syndromes · Tuberous Sclerosis Complex Research
Introduction
1
Eosinophilic Angiocentric Fibrosis (EAF) is a rare fibrotic condition first described by Holmes and Panje in 1983 as “Intranasal granuloma faciale” [1]. The term was then redefined in 1985 by Robert and McCann, as a mucosal lesion accompanied by thickening of the submucosal connective tissue [2,3]. It is a benign disease of an unknown etiology that affects the upper respiratory tract, mainly the paranasal sinuses and nasal septum; rarely, it involves the subglottic region and orbit [2]. This condition requires a high clinical suspicion, supportive imaging modalities, and laboratory testing to establish the diagnosis. Most importantly, its definitive diagnosis is achieved by histopathological evaluation, which shows the pathognomonic onionskin pattern reflecting the perivascular eosinophils-rich inflammatory infiltration with subsequent concentric fibrosis [4]. Sinonasal EAF typically presents with prolonged nasal obstruction, epistaxis, nasal deformities, facial pain, and epiphor [1]. This paper presents a case with clinicopathological findings of EAF involving the sinonasal tract, subglottic region, and orbit. This paper has been reported following the updated consensus of the Surgical Case Report (SCARE) guidelines [5].
Case presentation
2
We present a case of a fifty-five-year-old female patient known for controlled bronchial asthma, hypothyroidism, and IgG-4-related necrotizing blepharitis. The patient is a non-smoker, non-alcoholic, and retired from work. She was referred to our otolaryngology tertiary clinic due to her refractory nasal symptoms. She presented with a 14-year history of recurring bilateral nasal obstruction, mainly on the right side, associated with post-nasal drip, facial pressure, and hyposmia. However, she denies mucopurulent nasal discharge and visual disturbance, and her systemic review is unremarkable. Nonetheless, an allergic reaction was documented following her ingestion of hazelnuts and nonsteroidal anti-inflammatory drugs (NSAIDs). The patient reported that her symptoms were temporarily managed at another institution using intranasal steroid sprays. However, her condition reached a stage where more invasive intervention was needed, as she underwent three Functional Endoscopic Sinus Surgeries (FESS). Yet, her nasal symptoms were refractory. Upon physical examination, rhinoscopy revealed bilateral small nasal vestibules associated with fibrosis and adhesion of the nasal cavity and nasopharynx, nasal crusting (Fig. 1), and grade I subglottic stenosis evident by fiberoptic nasoendoscopy with an approximate luminal obstruction of 50 %, possibly attributed to the underlying EAF. However, a biopsy was not taken from this lesion. A Magnetic Resonance Imaging (MRI) of the paranasal sinuses showed an opacification within the bilateral nasal cavities, left maxillary, ethmoid, and sphenoid sinuses (Fig. 2).Fig. 1. Post-operative endoscopic findings of the nasal cavity, showing nasal mucosal crusting within the vestibule (A) and the nasopharynx (B), narrowed nasal vestibule (C), adhesions and fibrosis of the nasal cavity and nasopharynx (D).Fig. 1. Fig. 2Preoperative coronal T2-weighted MRI of the paranasal sinuses showing an opacification within the bilateral nasal cavities, left maxillary, ethmoid, and sphenoid sinuses.Fig. 2
Accordingly, a revision FESS was decided to improve the patient's symptoms and obtain a specimen from the left nasal mucosa and the frontal sinus cyst for histopathological evaluation. Specimens collected during the surgery revealed evidence of left nasal mucosal ulceration and purulent acute inflammation. Additionally, there was psudocystic formation involving the frontal sinus, which was lined by histiocytes in a background of dense fibrosis (Fig. 3). These findings, along with her clinical picture, supported a diagnosis of EAF. The patient had an uneventful postoperative course and was given a lifelong weekly follow-up appointment for her nasal crustations to be removed to improve her quality of life.Fig. 3: Histopathological findings of nasal mass biopsy, showing 40× dense fibrosis with eosinophils (A), 40× onion skin fibrosis around blood vessels (B), 20× showing many plasma cells and eosinophils (C), and IgG4 immunostaining shows numerous IgG4+ plasms cells over 100 in high power (D), Thus, confirms the diagnosis of EAF IgG4-related disease.Fig. 3
Discussion
3
EAF is an inflammatory process that develops slowly and progressively in its course, with a predilection for the upper respiratory and sinonasal tract. Rarely does it involve the subglottic region and orbit [6]. In our case, the patient was not only experiencing sinonasal involvement; rather, she had IgG-4-related necrotizing blepharitis and grade I subglottic stenosis. Histopathologically, EAF is characterized by the presence of multiple scattered eosinophils in a background of dense fibrosis [6]. The possible etiological theories of EAF include a past personal history of granuloma faciale, hypersensitivity to pollen, dust mites, animal dander, and certain foods due to high Immunoglobulin-E levels, and previous traumatic or iatrogenic injury to the sinonasal tract [1]. In 2011, Deshpande et al. suggested that EAF lies under the spectrum of immunoglobulin-G4-related disease, necessitating a modified approach to patients with this condition [6]. Nevertheless, not all cases of EAF fit the diagnostic criteria of immunoglobulinG4-related disease.
The majority of patients with EAF are females, presenting with non-specific signs and symptoms and usually delayed diagnosis [7]. These signs and symptoms include nasal obstruction, epistaxis, nasal deformity, facial pain, epiphora, and proptosis that collectively progress slowly over time [7]. Computed Tomography (CT) and MRI are non-specific diagnostic tools; however, the presence of an opacification involving the nasal cavity and paranasal sinuses aids in the diagnosis [1]. Thus, a definitive histopathological diagnosis is required to establish the diagnosis of EAF, which will show the pathognomonic onion-skin appearance of perivascular fibrosis that is associated with eosinophilic infiltration [7].
Based on our survey of the relevant scholarly literature, we have identified sixty-two cases of sinonasal EAF, aged twelve to eighty-one years. The median age among these patients was forty-nine years. The data revealed a relative female preponderance with a female: male ratio of 1.13: 1, equivalent to thirty-three female patients, while the remaining were male. The literature provides adequate evidence that the most frequently reported symptoms comprise nasal obstruction, Post-Nasal Drip (PND), mucosal crusting, and epistaxis. More overt manifestations, such as noticeable nasal deformity, are also commonly reported. Our patient experienced all these symptoms except for epistaxis (Table 1).Table 1. Summary of reported cases of eosinophilic angiocentric fibrosis.Table 1. ReferenceAgeGenderClinical PresentationTopographyManagementRoberts PF et al. [1]27 years-oldFemaleBilateral nasal obstructionNasal mucosaSystematic antihistamine, systematic and local steroids, and septoturbinoplasty.33 years-oldFemaleExertional shortness of breathSubglottic areaTracheostomy tube followed by laryngotracheoplasty.59 years-oldFemaleBilateral nasal obstructionNasal mucosa and skin of the noseAntihistamine and nose exploration.UrticariaPainful red patch over the nasal bridgeKarligkiotis et al. [1]46 years-oldMaleProptosis with lateral globe displacementRight orbit into anterior ethmoidEndoscopic diagnostic debulking.Right-sided nasal obstructionSupra-orbital headacheWJ Kim et al. [1]29 years-oldFemaleNasal obstructionPosterior wall of right maxillary sinusSystematic steroids, Fluticasone-salmeterol, docyfylline, mucolytics agents for 3 months followed by surgical resection.Productive coughDyspneaKeratli H et al. [1]30 years-oldFemaleMass under the right eye associated with epiphoraMedial orbit, extending to the anterior ethmoid sinuses and right middle turbinate.Debulking followed by systametic steroids and antihistamine.Leibovitch I et al. [1]61 years-oldMaleRight peri-orbital edemaRight medial orbital wallSystemic steroids and regular follow up.Right painful proptosisDeshpande V et al. [1]63 years-oldMaleOcular tearingNasal and lacrimal glandsSystemic steroids and surgical excision.Nasal congestionLung81 years-oldFemaleN/ALeft nasal mucosa31 years-oldFemaleN/AOrbitMaxillary and ethmoid sinusesNasal mucosa54 years-oldFemaleN/ARight lacrimal gland55 years-oldMaleN/AOrbitNguyen DB et al. [1]45 years-oldMaleBilateral nasal obstructionBilateral nasal bonesSurgical excisionNasal septumJain R et al. [1]31 years-oldFemaleRight epiphoraLeft maxillary and ethmoid sinusesSystemic steroids and surgical excisionLeft orbital massOrbit57 years-oldMaleNasal congestionBalateral lateral nasal wallsEpiphoraProptosisLacrimal glandHyposmia27 years-oldFemaleNasal obstructionBilateral lateral nasal walls51 years-oldFemaleNasal massRight lateral nasal wallsNasal obstructionEpiphoraLi Y et al. [1]27 years-oldFemaleNasal obstructionAnterior nasal cavityEndoscopic surgery and long-term intranasal topical corticosteroidsNasal dischargeEpistaxisFacial painChronic headache12 years-oldFemaleEpistaxisThe anterior septum of the right nasal cavityEndoscopic excisionNarayan J et al. [1]72 years-oldFemaleComplete stenosis of the left nostrilNasal septumMedical treatmentLeft lateral nasal wallNasal swellingPaun S et al. [1]37 years-oldFemaleEpistaxisLeft nasal cavitySurgical management, oral steroids, and azathioprineEpiphoraSymptoms of eustachian tube dysfunction68 years-oldMaleNasal obstructionNasal bridgeSurgical managementForehead57 years-oldFemaleNasal swellingInternal and external structure of the noseDapsone, hydroxychloroquine, azathioprine, and oral steroids58 years-oldFemaleN/ALateral nasal wallSurgical managementNigar E et al. [1]67 years-oldFemaleNasal obstructionRight noseMedical managementPurple discoloration of the overlying skinPareira EM et al. [1]52 years-oldMaleNasal obstructionNasal mucosa and septumSurgical managementLeft -sided tinnitus and hearing lossFacial sinus bonesNasal pruritusSneezingSlovik Y et al. [1]45 years-oldMaleNasal obstructionNasal bones, septum, and skinVasoconstrictive nasal drops as neededHyponasal speechCosmotic deformityRight maxillary and ethmoid sinusesLoane J et al. [1]42 years-oldMaleNasal obstructionNasal mucosaSurgical and medical managementPost-nasal dripYung A et al. [1]66 years-oldFemaleRecurrent epistaxisNasal mucosaMedical managementRight preauricular skin lesion45 years-oldFemaleNasal obstructionNasal mucosa and skinRecurrent epistaxisClauser L et al. [1]31 years-oldMaleNasal obstructionNasal cavity and septumSurgical managementNasal painEpistaxisKosarac et al. [1,9]19 years-oldFemaleNasal congestionRight maxillary sinusSurgical excisionFacial pain31 years-oldFemaleNasal obstructionRight nasal cavity49 years-oldMaleNasal obstructionNasal septumMatai V et al. [1]51 years-oldMaleNasal obstructionNasal septum mucosaMedical and surgical managementSnoringThompson LD et al. [1]28 years-oldMaleNasal obstructionLeft maxillary sinus and nasal septumSurgical excision and systemic corticosteroidsEpistaxis49 years-oldFemaleNasal obstructionNasal septumSeptoturbinoplasty and systemic corticosteroids64 years-oldFemaleNasal obstructionRight maxillary sinus and nasal septumSurgical excision and systemic corticosteroidsYavuzer R et al. [1]65 years-oldFemaleChronic sinusitisNasal mucosa and septumSurgical managementGoldman NC et al. [1]50 years-oldFemaleNasal obstructionNasal mucosaSurgical and medical managementHolme et al. [1]72 years-oldFemaleNasal obstructionNasal mucosaPulsed dye laser, dapsone and clofazimineOnder S et al. [14]45 years-oldMaleNasal obstructionNasal septumSurgical and medical managementChinelli PA et al. [1]31 years-oldFemaleNasal obstructionNasal mucosaMedical managementOwa AO et al. [1]41 years-oldMaleNasal obstructionNasal septumSurgical and medical managementSunde J et al. [1]63 years-oldMaleNasal obstructionNasal septumMedical managementHyposmiaTabaee A et el. [1]79 years-oldMaleNasal congestionNasal septum and lateral wallSurgical managementNasal tip tendernessNasal swellingYang BT et al. [1]26 years-oldFemaleNasal obstructionNasal septumSurgical and medical managementEpistaxisEyelid swellingProptosis16 years-oldMaleNasal septum62 years-oldFemaleRight lateral nasal wall28 years-oldMaleNasal septum24 years-oldFemaleNasal septum73 years-oldMaleLeft lateral nasal wallBurns BV et al. [1]38 years-oldMaleNasal obstructionRight nasal mucosaSurgical and medical managementNasal swellingHolmes DK et al. [1]49 years-oldMaleNasal obstructionRight nasal mucosaMedical managementValenzuela AA et al. [1]43 years-oldMaleNasal obstructionNasal cavityRegular follow-upsBilateral epiphoraWatanabe N et al. [1]51 years-oldMaleNasal obstructionNasal septumSurgical managementEthmoid boneGorostis et al. [3]61 years-oldMaleHeadacheRight ethmoido-orbital regionSurgical and medical managementNasal obstructionExophthalmosBlindnessJavadirad et al. [2]60 years-oldFemaleNasal obstructionNasal septumSurgical managementPost-nasal dripSazgar AA et al. [4]45 years-oldMaleNasal obstructionAnterior nasal cavitySurgical managementNasal dischargeRight maxillary alveolar ridgeEpistaxisPost-nasal dripFarina J et al. [15]76 years-oldMaleN/ANasal mucosaSurgical managementSaenz Ibarra B et al. [16]37 years-oldFemaleFacial painNasal mucosaSurgical and medical managementChronic sinusitisAllergic rhinitisNasal obstructionLegare et al. [17]58 years-oldMaleLeft eyelid swellingNasal cavityMedical managementEpistaxisLungsMedial periorbital soft tissue
Despite extensive documentation of this rare condition, the treatment guidelines for EAF remain unclear [9,10]. Previous cases have reported various management options, including surgical excision, FESS, and the use of intranasal or systemic corticosteroids [2]. Surgical excision is typically performed in advanced cases but is associated with a high recurrence rate. The use of intranasal or oral steroids has shown limited improvement [2]. Rituximab may benefit patients with refractory symptoms in both medical and surgical treatment [8].
In our case, the patient experienced symptomatic relief following revision FESS and three doses of Rituximab. However, she requires ongoing suctioning to manage nasal mucosal crusting. This ambiguous treatment approach presents a clinical dilemma regarding the optimal management of EAF patients, especially in patients like ours with rare extensive involvement in her sinonasal tract, subglottic region, and orbit.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent form is available for review by the editor-in-chief of this journal upon request.
Ethical approval
The ethical committee has approved this case report.
Guarantor
Jood K. Alotaibi.
Funding
This paper has not received any funding.
Author contribution
Jood K. Alotaibi, Raghad Alkhaldi, and Ramiz Muhammed Mumtaz have constructed and write the introduction, reviewed the literature for similar and studies, as well as the conclusion.
Naif Alotaibi contributed to the paper by writing the case itself, providing the supplementary imaging.
Anas Dababo provided the histopathological slides, and reported the histopathological evaluation of the patient.
Declaration of competing interest
There is nothing to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fang C.H.Mady L.J.Mirani N.Baredes S.Eloy J.A.Sinonasal eosinophilic angiocentric fibrosis: a systematic review Int. Forum Allergy Rhinol.49201474575210.1002/alr.2134725065665 · doi ↗ · pubmed ↗
- 2Javadirad E.Roozbahani N.E.Sadafi S.Eosinophilic angiocentric fibrosis of the sinonasal tract: a case report and review of the literature J. Int. Med. Res.509202203000605221126010.1177/03000605221126039 PMC 952802636172997 · doi ↗ · pubmed ↗
- 3Gorostis S.Bacha M.M.Gravier S.Raguin T.Right ethmoid eosinophilic angiocentric fibrosis with orbital extension Eur. Ann. Otorhinolaryngol. Head Neck Dis.1345201735135410.1016/j.anorl.2017.02.01228359733 · doi ↗ · pubmed ↗
- 4Sazgar A.A.Kia S.Akbari A.Nasal framework reconstruction in patient with eosinophilic angiocentric fibrosis Indian J. Otolaryngol. Head Neck Surg.71S 320182031203510.1007/s 12070-018-1453-x 31763288 PMC 6848623 · doi ↗ · pubmed ↗
- 5Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg.10952023 May 1113611403701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗
- 6Chew E.J.C.Lee M.H.Chung H.W.Tang P.H.Eosinophilic angiocentric fibrosis and immunoglobulin 4-related disease revisited Histopathology 812202214915810.1111/his.1464635312191 · doi ↗ · pubmed ↗
- 7Jain R.Robblee J.O’Sullivan-Mejia E.Lea J.Heller A.J.Faquin W.C.Powers C.N.Sinonasal eosinophilic angiocentric fibrosis: a report of four cases and review of literature Head Neck Pathol.24200830931510.1007/s 12105-008-0077-y 20614301 PMC 2807588 · doi ↗ · pubmed ↗
- 8Kim W.J.Kim Y.Kim J.Choi Y.H.Cho H.Choi Y.D.Seon H.Yoon S.Unexplained persistent dyspnea in a young woman with eosinophilic angiocentric fibrosis Respir. Care 5952013 e 72e 7610.4187/respcare.0264524149671 · doi ↗ · pubmed ↗