A Case of Emphysematous Gastritis Managed With Conservative Treatment
Ashwin Jagadish, Zain Alabdin Ibrahim, Stephen Bakeler, Usama Abu-Heija, Shahnawaz Notta, Noah Hall

TL;DR
A 67-year-old man with emphysematous gastritis was successfully treated with conservative methods, avoiding surgery.
Contribution
This case highlights the successful use of non-surgical treatment for a rare and severe gastric condition.
Findings
Emphysematous gastritis was diagnosed using CT imaging showing gastric wall inflammation and intramural gas.
Conservative treatment with antibiotics, fluids, and decompression led to symptom improvement and stable discharge.
The patient's encephalopathy and bradycardia resolved during inpatient care.
Abstract
Emphysematous gastritis is a rare condition associated with a high mortality rate. It is associated with various medications, chronic medical problems, and ingestions. Individuals can present with abdominal symptoms and even hemodynamic changes. Evaluating the patient with computed tomography (CT) imaging can show inflammation of the gastric wall and intramural gas. A conservative approach is often used to treat emphysematous gastritis, although surgical intervention may be necessary. Our case involves a 67-year-old male patient who presented with acute encephalopathy and bradycardia. He was noted to have epigastric tenderness, so non-contrast CT imaging of the abdomen and pelvis was performed. The imaging revealed emphysematous gastritis. Our patient was successfully managed with intravenous antibiotics, intravenous fluids, proton-pump inhibitors, and nasogastric decompression. His…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
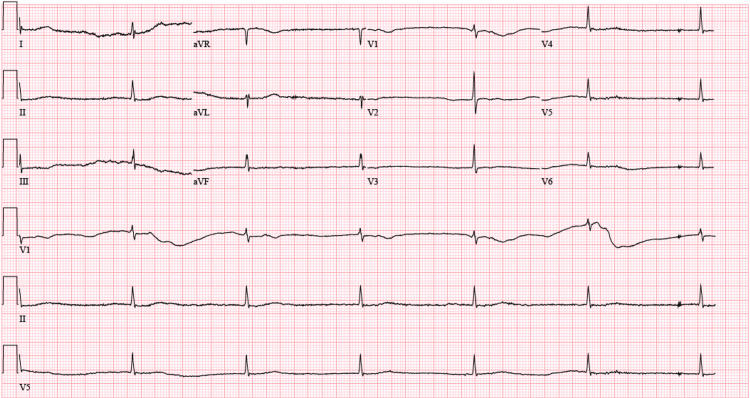 Figure 1
Figure 1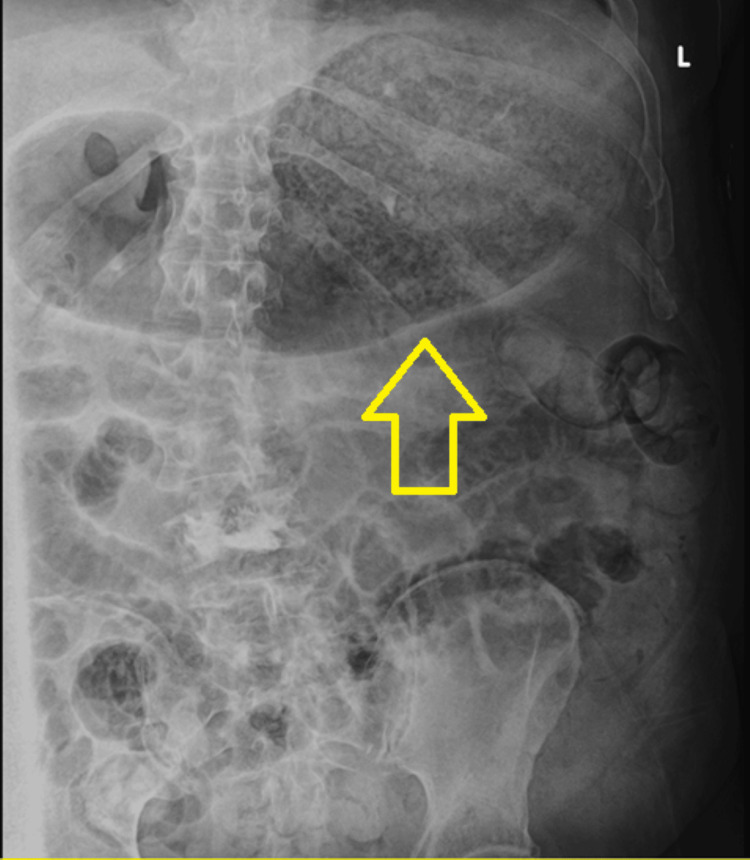 Figure 2
Figure 2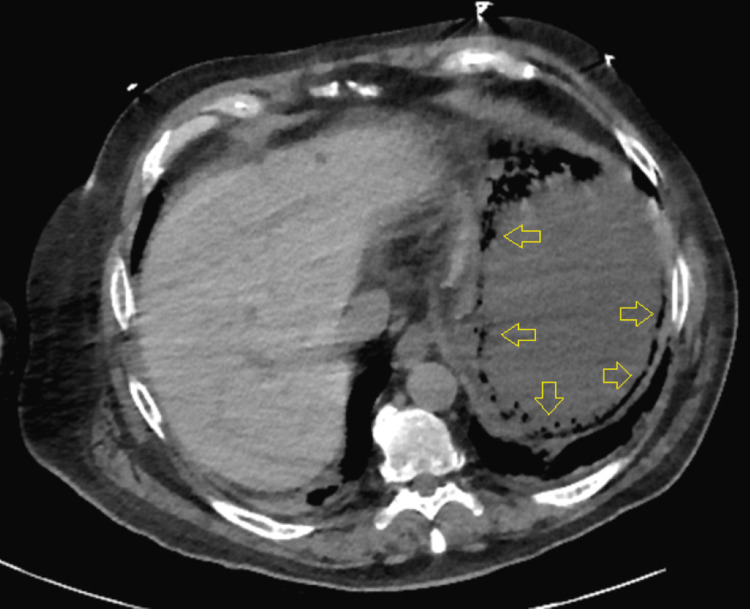 Figure 3
Figure 3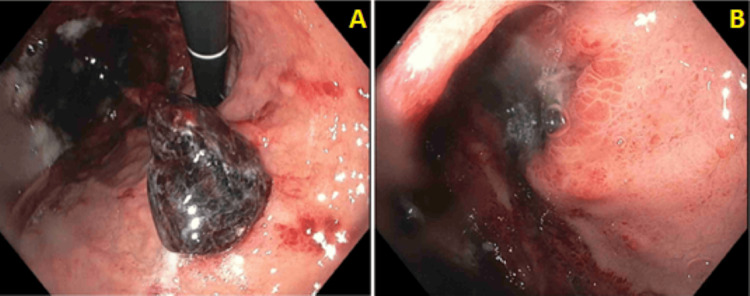 Figure 4
Figure 4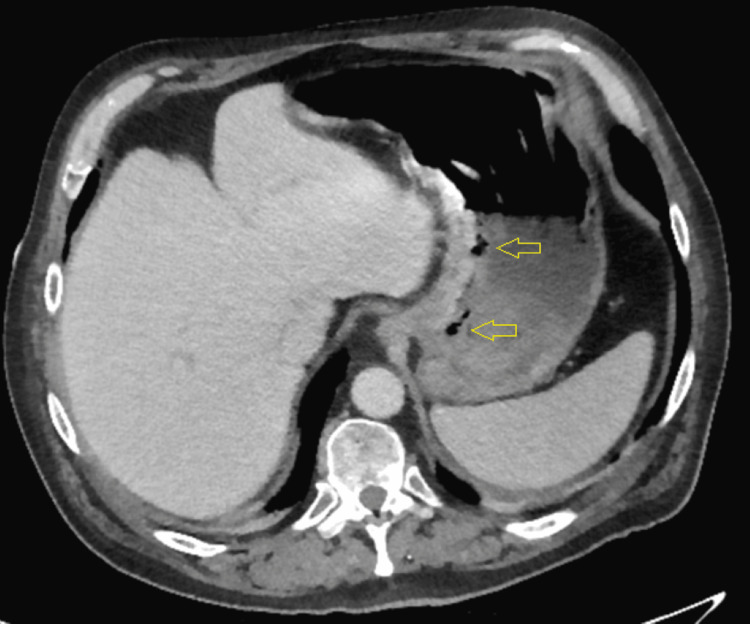 Figure 5
Figure 5| Parameters | Result | Reference Range |
| White Blood Cells (cells/µL) | 7,600 | 4,800–10,500 |
| Red Blood Cells (cells/µL) | 4,300,000 | 4,400,000–5,600,000 |
| Hemoglobin (g/dL) | 12.9 | 13.6–17.3 |
| Hematocrit (%) | 39.4 | 39.5–51.7 |
| Mean Corpuscular Volume (fL) | 92.3 | 83.5–96.8 |
| Mean Corpuscular Hemoglobin (pg) | 30.2 | 27.3–33.3 |
| Mean Corpuscular Hemoglobin Concentration (g/dL) | 32.7 | 32.9–34.6 |
| Red Blood Cell Distribution Width (%) | 14.1 | 11.6–14.1 |
| Platelets (cells/µL) | 160,000 | 166,000–383,000 |
| Mean Platelet Volume (fL) | 10.7 | 6.5–10.5 |
| Sodium (mEq/L) | 134 | 137–145 |
| Potassium (mEq/L) | 4.7 | 3.6–5.2 |
| Chloride (mEq/L) | 94 | 98–107 |
| Bicarbonate (mEq/L) | 29 | 22–29 |
| Glucose (mg/dL) | 180 | 70–99 |
| Blood Urea Nitrogen (mg/dL) | 40 | 5.0–25.0 |
| Creatinine (mg/dL) | 2.5 | 0.7–1.3 |
| Protein, Total (g/dL) | 7.5 | 6.3–8.2 |
| Albumin (g/dL) | 4.3 | 3.5–5.0 |
| Calcium (mg/dL) | 9.7 | 8.4–10.4 |
| Total Bilirubin (mg/dL) | 0.5 | 0.2–1.3 |
| Alkaline Phosphatase (U/L) | 121 | 40–150 |
| Aspartate Aminotransferase (U/L) | 41 | 5–34 |
| Alanine Aminotransferase (U/L) | 55 | 0–55 |
| Thyroid Stimulating Hormone (µIU/mL) | 0.843 | 0.35–4.94 |
| Ammonia (µmol/L) | 21 | 18–72 |
| Creatine Phosphokinase (U/L) | 34 | 30–200 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Biliary and Gastrointestinal Fistulas · Diverticular Disease and Complications
Introduction
Emphysematous gastritis is a rare condition characterized by diffuse inflammation of the gastric wall and intramural gas [1]. There are less than 200 documented cases of emphysematous gastritis [2]. The condition can have a mortality rate of up to 60% [3]. There are many risk factors associated with emphysematous gastritis [1]. Prior to the year 2000, surgical intervention was the main treatment approach; however, there has been a trend toward conservative management since then [4]. We present a case of emphysematous gastritis that was successfully managed with conservative treatment.
Case presentation
A 67-year-old male patient with a history of coronary artery disease, non-insulin-dependent type 2 diabetes mellitus, hypertension, hyperlipidemia, atrial fibrillation on apixaban, and cirrhosis due to alcohol presented to the emergency department due to acute encephalopathy and multiple ground-level falls. He was somnolent and was unable to provide a complete history. Per his spouse, the patient's encephalopathy started the previous night and was progressively worsening. He also had multiple ground-level falls that were triggered by positional changes. There was no recent consumption of alcohol, corticosteroids, or non-steroidal anti-inflammatory drugs.
On presentation, his blood pressure was 99/57 mmHg, his heart rate was bradycardic at 37 beats per minute, and his respirations were 18 breaths per minute. His electrocardiogram showed junctional bradycardia (Figure 1). His physical examination was notable for dry mucous membranes, diminished breath sounds at the bases, bradycardia, and altered mentation. His abdomen was soft, nontender, and nondistended; bowel sounds were present in all quadrants. Additionally, asterixis was absent. His initial laboratory results are presented in Table 1. His initial chest radiograph did not reveal any acute cardiopulmonary process. His heart rate did not improve adequately with atropine and 2 L of normal saline, so a dopamine infusion was initially required.
ElectrocardiogramElectrocardiogram showing bradycardia.
The following day, abdominal tenderness was observed during the physical examination. The initial abdominal radiograph revealed gastric distention (Figure 2). Subsequent computed tomography (CT) evaluation of the chest, abdomen, and pelvis without contrast revealed emphysematous gastritis (Figure 3). He was started on 3.375 g of intravenous piperacillin-tazobactam every six hours. He was also started on 40 mg of pantoprazole twice daily. A nasogastric (NG) tube was placed, and more than 1 L of fluid was removed. A temporary pacemaker was also placed.
Abdominal radiograph demonstrating gastric distentionThe arrow indicates the gastric distention.
Initial computed tomography imaging demonstrating emphysematous gastritisThe arrows indicate the emphysematous gastritis.
Two days later, his leukocyte count peaked at 13,200 cells/µL. Ongoing evaluation of the NG tube contents revealed bloody material. He subsequently underwent esophagogastroduodenoscopy (EGD) three days after the NG tube placement. The procedure revealed multiple ulcers in the gastric cardia and fundus that were covered by clots (Figures 4A, 4B). Given these findings, the EGD was terminated, and biopsies were not obtained. A repeat CT of the abdomen and pelvis with contrast, completed soon after the EGD, showed improving emphysematous gastritis (Figure 5). The NG tube was subsequently removed. During the interval between NG tube insertion and removal, the patient required maintenance fluids amounting to 6 L.
Results from esophagogastroduodenoscopy(A) Gastric body; (B) gastric fundus.
Repeat computed tomography imaging demonstrating improving emphysematous gastritisThe arrows indicate the improving emphysematous gastritis.
The following day, the temporary pacemaker was removed after improvement of the bradycardia. The cardiology team determined that the patient did not require permanent pacemaker placement while inpatient. Over the rest of his hospitalization, his encephalopathy ultimately resolved. Blood cultures, which were obtained upon presentation, remained negative throughout the hospitalization. He completed a six-day course on antibiotics, per infectious diseases recommendations. He was stable at discharge and was advised to continue the pantoprazole. Outpatient gastroenterology and cardiology follow-up appointments were also recommended.
Discussion
Emphysematous gastritis is a rare condition characterized by gas in the gastric wall and can have a mortality rate of up to 60% [3]. It is important to differentiate emphysematous gastritis from gastric emphysema [4]. Gastric emphysema is generally considered benign and results from air being introduced into the gastric wall [4]. On imaging, intramural gas tends to appear round, whereas intramural gas is more linear in emphysematous gastritis [4]. Management of gastric emphysema is often conservative, and the condition often resolves spontaneously [4].
Emphysematous gastritis can be associated with medications, chronic medical conditions, and ingestions [5]. Categories of medications associated with the condition include immunosuppressive agents, non-steroidal anti-inflammatory drugs, and corticosteroids [5]. Medical conditions associated with emphysematous gastritis include diabetes mellitus, ethanol consumption, renal disease, and poor nutrition [5]. Consumption of corrosive material is also associated with the condition [6]. Causative organisms have been determined in approximately half of the cases [7]. In cases where an organism is identified, the most common species of organisms include Klebsiella, Candida, Clostridium, Streptococcus, and Pseudomonas [4]. As compared to patients with gastric emphysema, patients with emphysematous gastritis tend to show signs of severe illness, such as sepsis [4]. In our case, the patient's diagnosis was based on the severity of presentation and intramural gas appearance on imaging.
Symptoms of emphysematous gastritis can include pain in the epigastric region, nausea, emesis, loose stools, leukocytosis, and hemodynamic instability [8]. Various imaging modalities can be used to help diagnose emphysematous gastritis [3]. Abdominal radiographs can show gastric dilation with intramural gas [3]. However, CT scans are often used since they are more sensitive [3]. Pertinent imaging findings for emphysematous gastritis include thickening of the gastric wall and the presence of intramural, irregular, mottled gas [9].
Management of emphysematous gastritis involves both medications and supportive measures [5]. Intravenous fluids, along with antibiotics that have coverage against gram-negative and anaerobic organisms, are often necessary [5]. Additionally, an NG tube can be placed to assist with gastric decompression [10]. Surgical intervention may be required if the patient's status declines or there are concerns for peritonitis, infarction of the stomach, or inadequate response to medical management [11].
Conclusions
Emphysematous gastritis is an uncommon condition with a mortality rate of up to 60%. It can be associated with medications, chronic medical problems, or ingestions. In approximately 50% of cases, a causative organism is identified. It is often diagnosed using imaging, with CT scans being more sensitive than radiographs. Management of the condition is generally supportive care alongside antibiotic coverage. However, in some cases, surgical intervention may be necessary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Successful conservative treatment of emphysematous gastritis Intern Med Takano Y Yamamura E Gomi K 1951985420152574301110.2169/internalmedicine.54.3337 · doi ↗ · pubmed ↗
- 2Successful medical management of emphysematous gastritis Chest Cecchini A Cecchini A Darweesh M Sill J 01642023 https://journal.chestnet.org/article/S 0012-369202343-7/fulltext
- 3Emphysematous gastritis: case report and literature review Int J Surg Al-Jundi W Shebl A 066200810.1016/j.ijsu.2007.02.00717446149 · doi ↗ · pubmed ↗
- 4Emphysematous gastritis in a patient with neutropenic sepsis: a case report and literature review with comment on management J Intensive Care Soc Jenkins JK Georgiou A Laugharne M Meisner S Cook T 3283312420233774407010.1177/17511437231153048 PMC 10515328 · doi ↗ · pubmed ↗
- 5Emphysematous gastritis: a case series on a rare but critical gastrointestinal condition Cureus Qasim A Penikelapate S Sosa F Jyala A Ghazanfar H Patel H Dev A 015202310.7759/cureus.50409 PMC 1078395938213347 · doi ↗ · pubmed ↗
- 6Role of conservative management in emphysematous gastritis BMJ Case Rep Nemakayala DR Rai MP Rayamajhi S Jafri SM 2018201810.1136/bcr-2017-222118 PMC 584790029477992 · doi ↗ · pubmed ↗
- 7Emphysematous gastritis BMJ Case Rep Ono R Ito R Yamamoto K Aoki K Kobayashi Y 15202210.1136/bcr-2022-251314 PMC 937948435961686 · doi ↗ · pubmed ↗
- 8The predictors of mortality and secular changes in management strategies in emphysematous gastritis Clin Res Hepatol Gastroenterol Watson A Bul V Staudacher J Carroll R Yazici C 0741201710.1016/j.clinre.2016.02.01127339595 · doi ↗ · pubmed ↗