Endoscopic submucosal dissection of early gastric cancer in the gastric fundus: challenges and techniques
Rafael Prado Pessoa, Laís Martins Magalhães Almeida, Caroline Assis Aleixo Chaves, Lucas Gallo de Alvarenga Mafra, Bernardo Ferreira de Paula Ricardo, Nelson Tomio Miyajima, Rodrigo Roda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
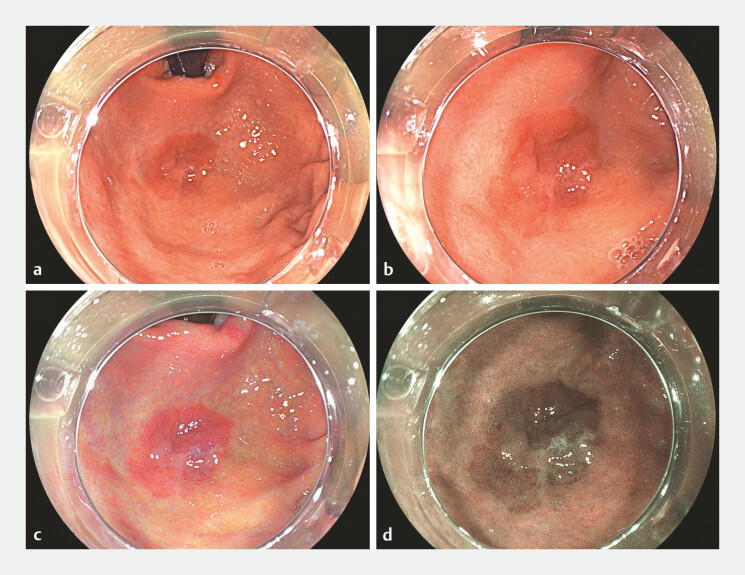 Fig. 1
Fig. 1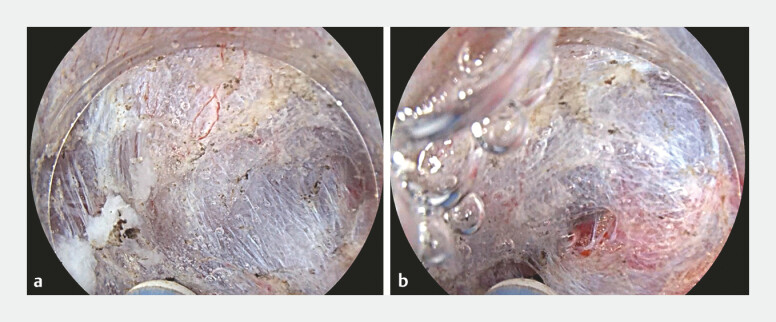 Fig. 2
Fig. 2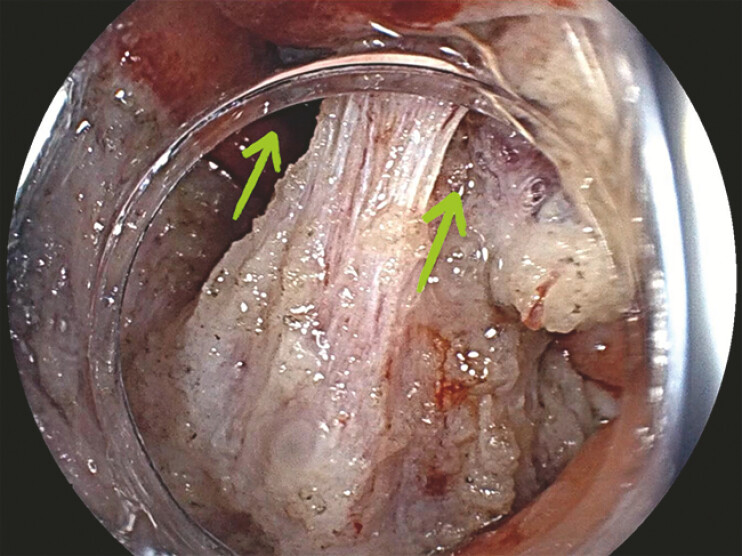 Fig. 3
Fig. 3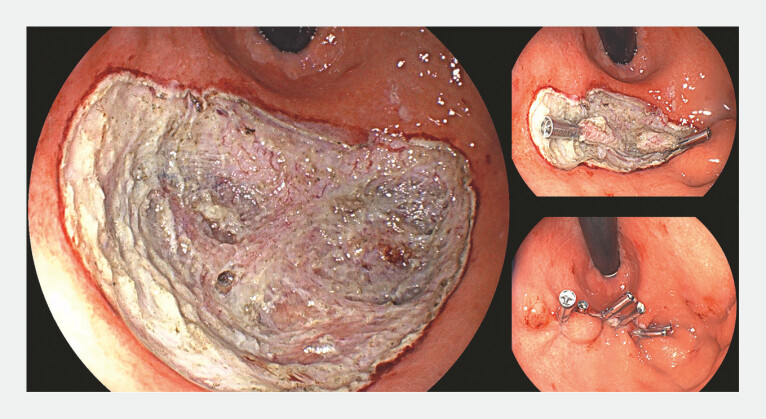 Fig. 4
Fig. 4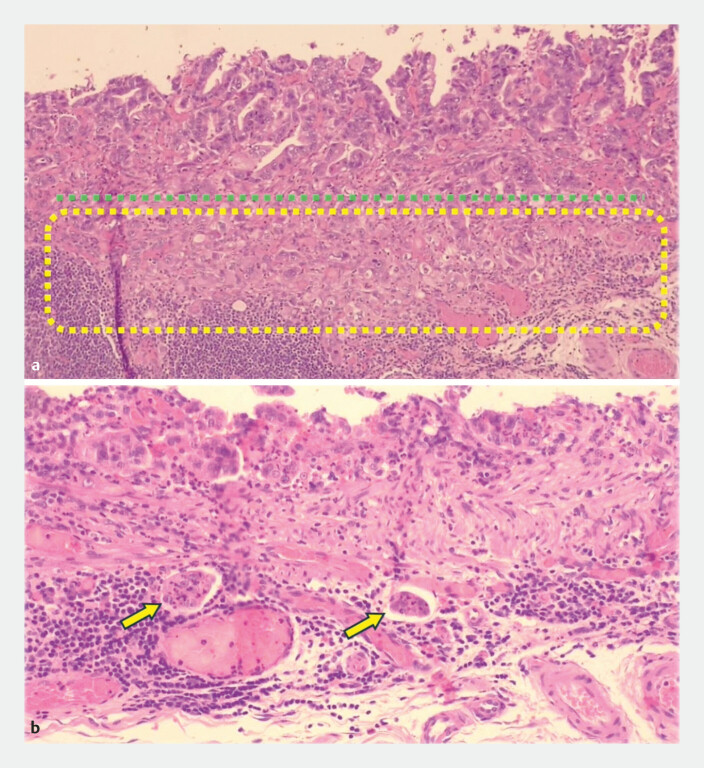 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Metastasis and carcinoma case studies · Gastrointestinal Tumor Research and Treatment
Endoscopic submucosal dissection (ESD) of tumors located in the gastric fundus is technically challenging. The wall is thin and has a rich vascularization, which increases the risk of perforation and bleeding 1 . The procedure is mostly performed in retroflexion, and the tip of the endoscope has limited reach.
In this video ( Video 1 ), we presented a case of a 73-year-old patient with upper gastrointestinal endoscopy showing an elevated superficial lesion (0–IIa) measuring 30 mm × 20 mm, in the gastric fundus ( Fig. 1 ). Biopsies showed high-grade dysplasia.
Endoscopic submucosal dissection of early gastric cancer in the gastric fundus using the underwater approach and an external traction technique.Video 1
Elevated superficial lesion (Paris 0–IIa) measuring approximately 30 mm × 20 mm, in the gastric fundus. Targeted biopsies showed high-grade dysplasia. a and b White light aspect of the lesion. c LCI. d BLI. Abbreviations: BLI, blue laser imaging; LCI, linked color imaging.
The procedure was performed with an optical magnification gastroscope (EG-760Z, Fujifilm Medical). The knife used was an injectable needle knife (ORISE ProKnife; Boston Scientific).
Due to the gastric fundus thin wall, it was possible to visualize the visceral fat through the wall. At two points, the dissection was deepened into the muscular layer, without complete perforation. The underwater technique was then performed to avoid over-distension of the organ, an undesirable distance of the resection area and to position the tip of the knife more parallel to the muscular layer 2 ( Fig. 2 ).
Underwater approach. The tip of the knife is almost parallel to the muscle layer, which makes dissection safer against perforation.
External traction method with clip and snare was also used 3 ( Fig. 3 ). This traction technique allows you to pull or push the snare, which was attached to the clip, applying the appropriate tension to safely expose the submucosa.
External traction technique using clip and snare. This traction technique allows you to pull or push the snare, which was attached to the clip, applying the appropriate tension to safely expose the submucosa.
After complete resection of the lesion, it was placed two clips over the submucosa and then, complete closure of the ulcer area ( Fig. 4 ).
Final aspect of the procedure. Two clips were applied into the dissection layer, followed by the complete closure of the ulcer.
Regarding histopathology, the resection was classified as endoscopic curability C-2 (eCuraC-2) ( Fig. 5 ). Therefore, the patient must undergo surgical completion 4 .
a The green dotted line corresponds to the muscularis mucosae. The content of the yellow rectangle corresponds to the invasion of the submucosa. b The arrows correspond to the angiolymphatic emboli.
With the case presented, we can conclude that the endoscopist must be prepared to use techniques such as external traction and underwater dissection for the viability of technically challenging ESD’s. The monobloc resection ensured accurate staging and reinforced surgical indication.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baldaque-Silva F Pereira JP Maltzman H Topflight endoscopic submucosal dissection: a novel strategy for the resection of gastric fundus tumors Video GIE 2023849349610.1016/j.vgie.2023.08.01138155819 PMC 10751465 · doi ↗ · pubmed ↗
- 2Libânio D Pimentel-Nunes P Bastiaansen B Endoscopic submucosal dissection techniques and technology: European Society of Gastrointestinal Endoscopy (ESGE) technical review Endoscopy 20235536138910.1055/a-2031-087436882090 · doi ↗ · pubmed ↗
- 3Deng R Wu J Li D Clip-and-snare method with a pre-looping technique versus conventional method in the treatment of precancerous lesion and early gastric cancer: a retrospective study BMC Gastroenterol 20242417038760726 10.1186/s 12876-024-03231-w PMC 11100069 · doi ↗ · pubmed ↗
- 4Japanese Gastric Cancer Association Japanese gastric cancer treatment guidelines 2021 Gastric Cancer 20232612536342574 10.1007/s 10120-022-01331-8PMC 9813208 · doi ↗ · pubmed ↗