Two-devices-in-one-channel method using biopsy forceps for ultrasonography-guided hepaticogastrostomy reintervention
Akito Furuta, Shunsuke Omoto, Hironori Tanaka, Takashi Koriyama, Mamoru Takenaka, Taro Inoue, Wataru Ono

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
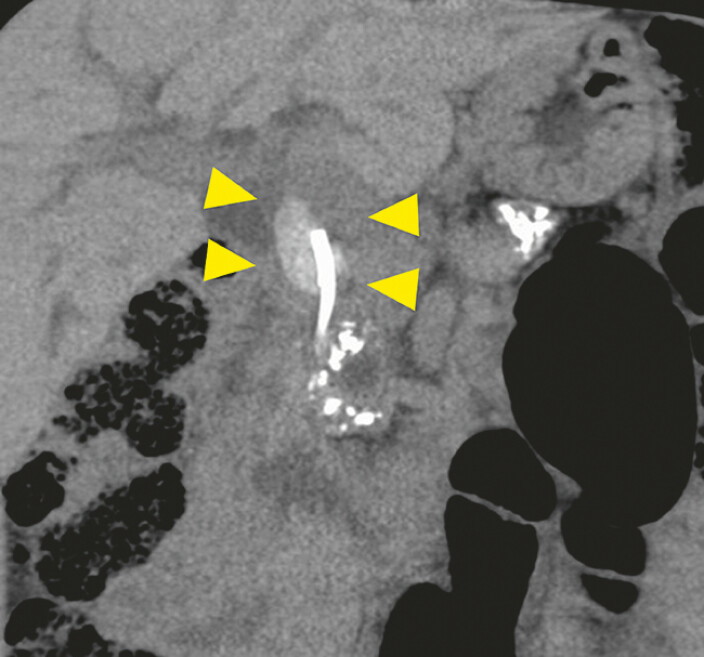 Fig. 1
Fig. 1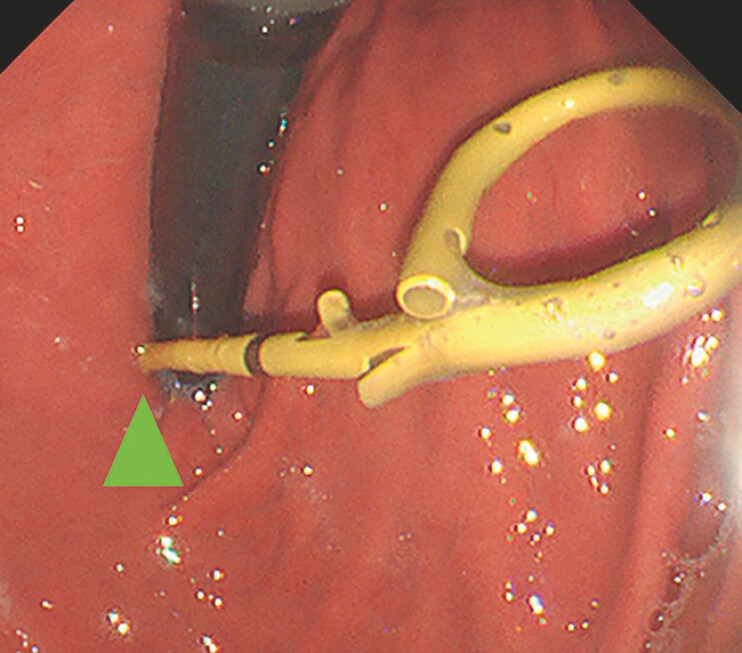 Fig. 2
Fig. 2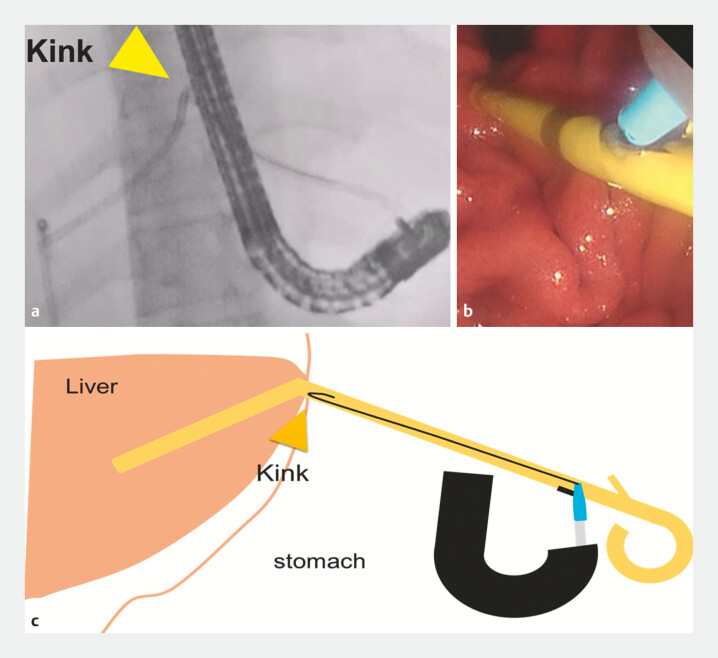 Fig. 3
Fig. 3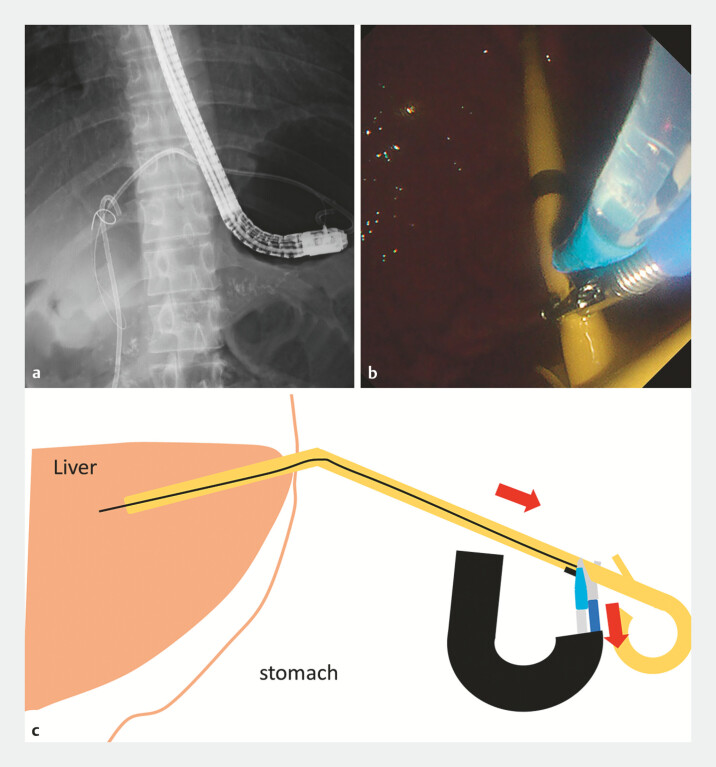 Fig. 4
Fig. 4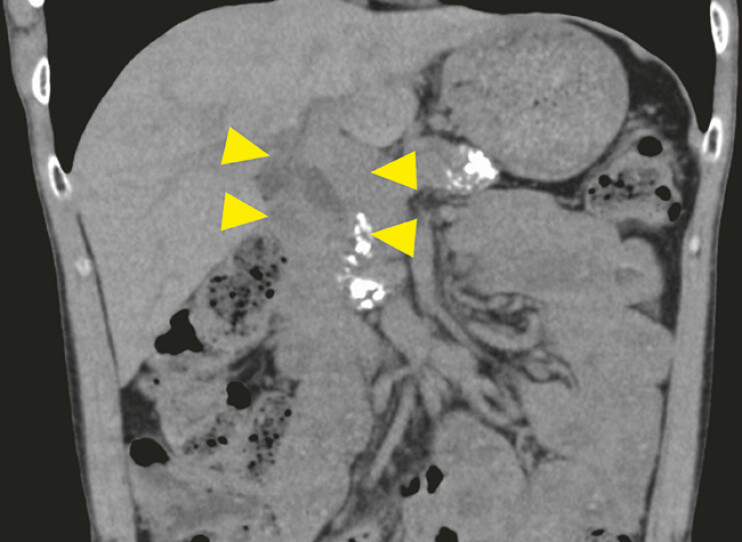 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research · Pediatric Hepatobiliary Diseases and Treatments
Reintervention following endoscopic ultrasonography-guided hepaticogastrostomy (EUS-HGS) remains challenging 1 . Several reintervention techniques have been described in the literature 2 3 4 5 . A particular technical difficulty arises when the endoscope position is unstable, especially when the HGS stent is placed in segment B2, where the proximity of the puncture site to the esophagus complicates the approach.
Herein, we report a case in which biopsy forceps were used to successfully facilitate guidewire insertion through the side hole of a type IT stent (Gadelius Medical, Tokyo, Japan) in segment B2, using the two-devices-in-one-channel technique ( Video 1 ).
The biopsy forceps facilitated guidewire insertion for ultrasonography-guided hepaticogastrostomy reintervention through the side hole of a plastic stent placed in segment B2, using the two-devices-in-one-channel method.Video 1
The patient, a 39-year-old man with alcoholic chronic pancreatitis, had undergone biliary plastic stent placement for distal bile duct stricture 8 years previously. Computed tomography revealed a stent retained in the common bile duct (CBD) with a large integrated stone ( Fig. 1 ). We successfully removed the stent via initial endoscopic retrograde cholangiopancreatography (ERCP). However, a severe stricture persisted in the distal bile duct. When balloon dilation proved inadequate, transpapillary ERCP was abandoned in favor of EUS-HGS. An IT stent was deployed in segment B2 to facilitate stone removal.
Computed tomography of a patient with chronic pancreatitis revealed a retained stent in the common bile duct with a large integrated stone (arrow).
For reintervention, we used an ERCP scope (TJF-Q290V; Olympus, Tokyo, Japan). The position of the plastic stent near the esophagogastric junction created access difficulties ( Fig. 2 ). The stent flap was resected using a snare to facilitate guidewire insertion. Although the guidewire successfully entered the stent, its passage was impeded by the kinking at the gastric wall ( Fig. 3 ). Biopsy forceps were used to grasp and retract the stent, thereby stabilizing it and correcting the kink, enabling guidewire passage ( Fig. 4 ) and successful CBD stone removal ( Fig. 5 ).
The position of the plastic stent near the esophagogastric junction (arrow) created access difficulties.
Although the guidewire successfully entered the stent, its passage was impeded by kinking at the gastric wall (arrow). a Fluoroscopic image. b Endoscopic image. c Schematic.
Biopsy forceps were used to grasp and retract the stent, thereby stabilizing it and correcting the kink, enabling guidewire passage. a Fluoroscopic image. b Endoscopic image. c Schematic.
Finally, the common bile duct stone was successfully removed (arrow).
This case illustrates the utility of the two-devices-in-one-channel technique for EUS-HGS reintervention. The simultaneous use of biopsy forceps for stent manipulation while maintaining guidewire access through a single channel offers a viable solution for technically demanding cases.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Minaga K Kitano M Uenoyama Y Feasibility and efficacy of endoscopic reintervention after covered metal stent placement for EUS-guided hepaticogastrostomy: a multicenter experience Endosc Ultrasound 20221147848610.4103/EUS-D-22-0002936537385 PMC 9921972 · doi ↗ · pubmed ↗
- 2Hijioka S Sakamoto Y Nagashio Y Novel and safe plastic stent exchange method after endoscopic ultrasound-guided hepaticogastrostomy with incomplete fistula (side hole method)Endoscopy 20235501 E 24E 2536113486 10.1055/a-1930-6319 PMC 9812677 · doi ↗ · pubmed ↗
- 3Ishikawa-Kakiya Y Maruyama H Yamamura MA simple replacement method for a 7 Fr dedicated plastic stent in endoscopic ultrasound-guided hepaticogastrostomy Endoscopy 20235501 E 745E 74637236259 10.1055/a-2081-9593 PMC 10219760 · doi ↗ · pubmed ↗
- 4Takenaka M Nakai A Kudo M Large balloon expansion method for re-intervention after endoscopic ultrasound-guided hepaticogastrostomy for stent obstruction Dig Endosc 201931 e 99e 10010.1111/den.1346231273839 · doi ↗ · pubmed ↗
- 5Minaga K Takenaka M Miyata T Through-the-mesh technique after endoscopic ultrasonography-guided hepaticogastrostomy: a novel re-intervention method Endoscopy 201648 E 369E 37010.1055/s-0042-11771427875842 · doi ↗ · pubmed ↗