Economic analysis of triclosan-coated versus uncoated sutures at preventing surgical site infection in patients undergoing abdominal surgery
Mwayi Kachapila, Dmitri Nepogodiev, Bryar Kadir, Maria Picciochi, Sivesh K Kamarajah, Aneel Bhangu, Raymond Oppong

TL;DR
This study evaluates whether triclosan-coated sutures reduce surgical site infections and healthcare costs compared to uncoated sutures, finding significant uncertainty in cost savings.
Contribution
The study introduces a global economic analysis of triclosan-coated sutures using country-specific data and sensitivity analyses.
Findings
Cost differences per patient ranged from −$466 to $171 in high-HDI countries using triclosan-coated sutures.
The largest potential savings and expenditure occurred in contaminated-dirty wounds.
Similar results were observed in 184 of 193 countries at the national level.
Abstract
A recent meta-analysis of high-quality randomized trials casts doubt on the effectiveness of triclosan-coated sutures in reducing surgical site infection (SSI). This economic analysis is aimed at assessing whether triclosan-coated sutures, compared with uncoated sutures, can reduce costs from a healthcare perspective. This was a model-based economic analysis mainly informed by baseline SSI rates, effect size CIs from a recent meta-analysis of high-quality trials (OR 0.90, 95% CI 0.74 to 1.09, p=0.29), and country-specific cost data. This was a worldwide analysis that estimated average cost savings aggregated for high, middle, and low Human Development Index (HDI) countries and country-specific cost savings for the 193 countries on the HDI list. Participants were patients undergoing abdominal surgery. The analysis was informed by baseline SSI rates from an international cohort study…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
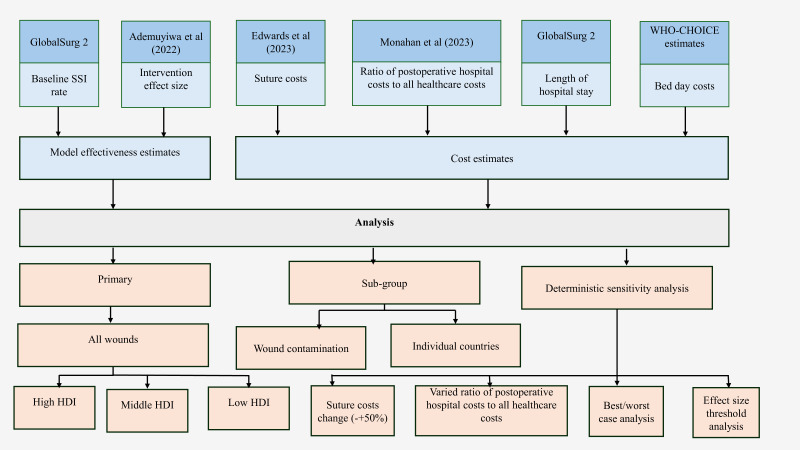 Figure 1
Figure 1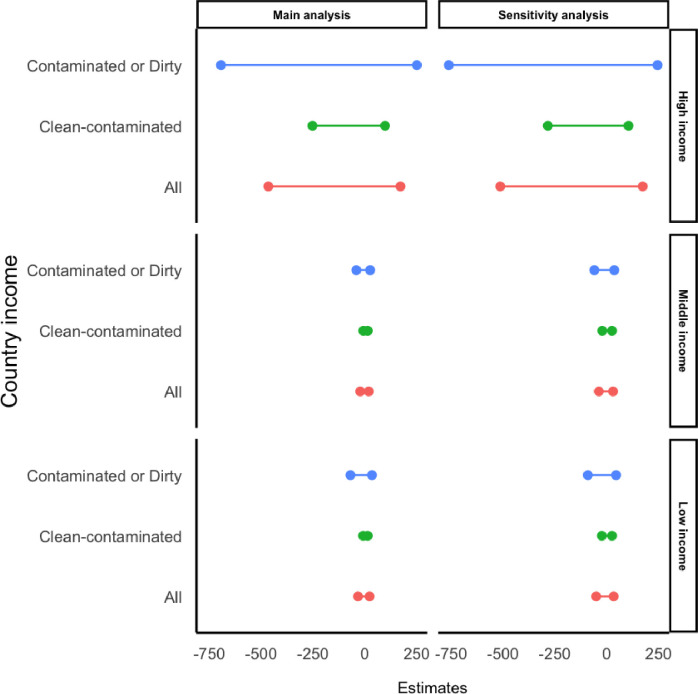 Figure 2
Figure 2| Patient category | Baseline SSI rate (%) | Intervention arm SSI rate (%) | Length of hospital stay (patients with SSI) | Length of hospital stay (patients without SSI) | Hospital bed-day cost (all patients) | Cost of hospital stay (patients with SSI) | Cost of hospital stay (patients without SSI) |
|---|---|---|---|---|---|---|---|
| High-HDI countries: clean-contaminated wounds | 7.6 | 6.8 | 11.40 | 4.20 | $1610 | $18 357 | $6763 |
| High-HDI countries: contaminated-dirty wounds | 19.0 | 17.1 | 14.20 | 6.60 | $1610 | $22 866 | $10 628 |
| Middle-HDI countries: clean-contaminated wounds | 11.1 | 10.0 | 6.20 | 2.90 | $138 | $856 | $401 |
| Middle-HDI countries: contaminated-dirty wounds | 20.0 | 18.0 | 11.50 | 5.50 | $138 | $1588 | $760 |
| Low-HDI countries: clean-contaminated wounds | 16.1 | 14.5 | 7.80 | 4.30 | $92 | $720 | $397 |
| Low-HDI countries: contaminated-dirty wounds | 39.0 | 35.1 | 15.20 | 8.20 | $92 | $1403 | $757 |
| Item | Data source short name | Possible variations between countries | Possible variations within countries |
|---|---|---|---|
| Baseline SSI rates | GlobalSurg 2 | Used country-specific data. Low chances of bias because of using country-specific data from a prospective international study. | Model used country averages, but SSI rates may vary within a country. |
| Effect size | Ademuyiwa | Effect sizes may vary by country due to epidemiological factors, but a global effect size was used being the best available data. | Effect size may vary within a country, but this was the best available data. |
| Coated and uncoated suture costs | Edwards | Cost of the suture was available from only one supplier, but the actual cost may vary by country. Wide range of the costs used in the sensitivity analysis. | There might be within-country variations that cannot be captured with the available data. |
| Ratio of postoperative hospital costs to all healthcare costs | Monahan | The ratio may vary by country, but this was the best available data. | The ratio may vary within a country, but this was the best available data. |
| Length of hospital stay (LoS) | GlobalSurg 2 | Used HDI group averages assuming that the LoS will apply to all countries in a given HDI category. | The LoS may vary within a country, but this was the best available data. |
| Bed-day costs | WHO-CHOICE estimates | Used country-specific data. Low chances of bias because of using country-specific data from a prospective international study. | Model used country averages, but SSI rates may vary within a country. |
| Patient category | Average total cost difference for patients with and without an SSI | Coated suture | Uncoated suture | Cost difference per patient |
|---|---|---|---|---|
| High-HDI countries: all wounds | $11 916 | $1382 to $2019 | $1848 | −$466 to $171 |
| High-HDI countries: clean-contaminated wounds | $11 594 | $776 to $1026 | $1028 | −$253 to $97 |
| High-HDI countries: contaminated-dirty wounds | $12 238 | $2032 to $2726 | $2726 | −$694 to $250 |
| Middle-HDI countries: all wounds | $642 | $120 to $161 | $144 | −$23 to $18 |
| Middle-HDI countries: clean-contaminated wounds | $456 | $78 to $99 | $86 | −$8 to $13 |
| Middle-HDI countries: contaminated-dirty wounds | $829 | $177 to $244 | $221 | −$43 to $25 |
| Low-HDI countries: all wounds | $484 | $152 to $208 | $186 | −$34 to $22 |
| Low-HDI countries: clean-contaminated wounds | $323 | $81 to $103 | $90 | −$9 to $13 |
| Low-HDI countries: contaminated-dirty wounds | $646 | $256 to $361 | $326 | −$71 to $34 |
| Patient category | Cost of coated suture was increased by 50% | Cost of coated suture was decreased by 50% | Cost of uncoated suture was increased by 50% | Cost of uncoated suture was decreased by 50% | The proportion of hospital stay costs to all healthcare costs was adjusted to 0.88 | The proportion of hospital stay costs to all healthcare costs was adjusted to 0.96 | Best-case scenario | Worst-case scenario |
|---|---|---|---|---|---|---|---|---|
| High income: all wounds | −$448 to $189 | −$483 to $155 | −$480 to $157 | −$452 to $185 | −$500 to +$183 | −$430 to +$159 | −$533 | $192 |
| High income: clean-contaminated wounds | −$235 to $115 | −$270 to $80 | −$267 to $83 | −$239 to $111 | −$270 to +$104 | −$234 to +$91 | −$303 | $124 |
| High income: contaminated-dirty wounds | −$676 to $268 | −$711 to $233 | −$708 to $236 | −$680 to $264 | −$749 to +$269 | −$637 to +$230 | −$783 | $265 |
| Middle income: all wounds | −$5 to $36 | −$40 to $1 | −$37 to $3 | −$9 to $31 | −$25 to +$19 | −$20 to +$17 | −$57 | $49 |
| Middle income: clean-contaminated wounds | $10 to $31 | $25 to −$4 | −$22 to −$2 | $6 to $26 | −$9 to +$13 | −$6 to +$12 | −$41 | $44 |
| Middle income: contaminated-dirty wounds | −$25 to $43 | −$60 to $8 | −$57 to $10 | −$29 to $38 | −$46 to +$26 | −$38 to +$23 | −$78 | $55 |
| Low income: all wounds | −$16 to $40 | −$51 to $5 | −$48 to $7 | −$20 to $35 | −$37 to +$23 | −$30 to +$20 | −$69 | $52 |
| Low income: clean-contaminated wounds | $9 to $31 | −$26 to −$4 | −$23 to −$1 | $5 to $27 | −$10 to +$13 | −$7 to +$12 | −$42 | $44 |
| Low income: contaminated-dirty wounds | −$52 to $52 | −$87 to $17 | −$85 to $20 | −$57 to $48 | −$77 to +$37 | −$63 to +$32 | −$109 | $64 |
- —http://dx.doi.org/10.13039/501100000272National Institute for Health and Care Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Surgical Sutures and Adhesives · Orthopedic Infections and Treatments
Introduction
Surgical site infection (SSI) is the most common complication after surgery worldwide and affects both patients and healthcare systems.1 It affects 9.4% of surgical patients in high Human Development Index (HDI) countries, 14.0% in middle-HDI countries, and 23.2% in low-HDI countries.2 Patients experience pain, anxiety, and emotional and social adverse effects, including a decline in mental health and quality of life, which can persist for several months and incur higher direct and indirect healthcare costs compared with patients without SSIs.38 Additionally, patients with SSI have higher societal costs associated with lost income due to late return to work and mortality, which may represent 90% of overall SSI costs.5
In the past decade, the WHO recommended 29 strategies for SSI prevention, including chlorhexidine gluconate for skin preparation and triclosan-coated suture for abdominal wall closure.9 10 However, evidence that informed the recommendations was not of high quality.1 Meta-analyses of randomized trials for triclosan-coated sutures have proved overwhelmingly positive effect but have mostly been based on mixed quality data with a strong dilution effect from low-quality trials. More recent meta-analysis that focused on only five methodologically high-quality randomized trials showed that there was no significant difference in SSI rates between triclosan-coated sutures and uncoated sutures.11 The data were from high, middle, and low-HDI countries and numerically outweighed data from low-quality trials, providing a more definitive conclusion.
Previous economic analyses that evaluated the impact of triclosan-coated sutures, compared with uncoated sutures, at SSI prevention included data from Italy, USA, Egypt, and UK among several surgical procedures including abdominal surgery.1215 However, economic analysis results, including analyses on SSIs, from one country may not be useful to decision-makers in another country because of differences in SSI rates, wound complications, healthcare systems, and economic conditions across countries.16 17 The aim of this economic analysis was to assess the costs associated with SSIs when triclosan-coated suture was used, compared with uncoated suture, among patients undergoing elective and emergency abdominal surgery in all countries in the world. We aimed to use a CI approach, in keeping with statistical decision-making around clinical effects, where interpretation is based around uncertainty from a CI rather than a single point estimate, which is highly likely to be misleading.
Methods
Overall study design
This model-based economic analysis was conducted to determine whether triclosan-coated suture use is associated with a net reduction in healthcare costs from a healthcare perspective in high, middle, and low HDIs using the 2022 classifications.18 19 The multistep analysis evaluated the average total healthcare costs associated with SSIs in triclosan-coated versus uncoated suture groups in patients undergoing abdominal surgery based on the 95% CI of the effect size of coated suture.11 This model focused on the suture-related cost, defined as the fascial suture cost plus the average cost per patient of treating SSI, calculated by multiplying the SSI rate and cost of managing one SSI.
Patient and public involvement
Patient and public involvement was not appropriate for this study because it was a model-based economic analysis that used secondary data from published studies. As this study used existing data, direct engagement with patients or the public was not necessary. While the study aims at improving the patient outcomes through reduced SSIs and reduced costs, the modeling approach used in the study presented challenges for direct patient and public involvement in that specific aspect of the research process.
Data sources
To perform the analysis, several data sources (figure 1) were required as below:
Baseline effect size: The baseline SSI rates for each country were identified from a dataset of a recent international, prospective, multicenter, cohort study. The study measured the incidence of SSI among 12 539 patients (from 343 hospitals in 66 countries) undergoing elective or emergency gastrointestinal resection in high, middle, and low-HDI countries (GlobalSurg 2) between January and July 2016.2 It aimed to estimate the burden of SSI and quantify the differences in SSI rates across varying HDI settings. GlobalSurg 2 recruited consecutive patients undergoing elective or emergency or gastrointestinal resection for a prespecified 2-week period at each participating hospital. The study assessed the patients for SSIs at 30 days following the surgery in line with the US Centers for Disease Control and Prevention definition by trained SSI assessors.2 The dataset disaggregated surgical patients by wound contamination: clean-contaminated, contaminated, and dirty surgery. For this analysis, SSI rates for contaminated and dirty surgery were aggregated into one category (tables12). Limitations of the study have been included in online supplemental appendix S4.Intervention effect size: Since our primary aim was to estimate the potential cost increases or savings from SSIs using triclosan-coated sutures, we used estimated effect sizes from a recently published meta-analysis of five high-quality randomized trials.11 In keeping with frequentist statistical techniques, we used the 95% CI rather than the central point estimate, replicating significance results and policy decision-making. In such methodologies, if the CI crosses one, this indicates non-significance; the central point estimate is not used in isolation. The published meta-analysis established a 95% CI of 0.74 to 1.09 (central point estimate 0.90, p=0.29).11 Therefore, 0.74 then acts as the lower bound (ie, reduction in SSI) and 1.09 as the upper bound (ie, increase in SSI). In the base case, we did not calculate models for the central point estimate, in keeping with this preplanned methodology.Cost of SSI: The cost of an SSI was informed by a study that estimated the postoperative costs of patients with and without an SSI in middle-HDI countries. The study found that the proportion of postoperative hospital stay costs to total postoperative healthcare costs was 0.92.7 Therefore, the additional cost of an SSI was based on the cost of the hospital stay, as well as the expenses for treatments (dressings, investigations, medications, and postoperative follow-up) resulting from the SSI. The postoperative length of hospital stay for both patients with and without an SSI was sourced from the GlobalSurg 2 dataset.2 The hospital bed-day costs were sourced from the WHO-CHOICE country-specific costs (table 1).20 The bed-day costs were averaged for all countries in a given HDI category, and for the country-level analysis, each country was assigned a specific country-level cost from the WHO-CHOICE country-specific costs. All costs were converted to US dollars using purchasing power parity (PPP) exchange rates, and where the PPP conversion rates were not available, the implied PPP conversion rates were used.21 22 The costs were adjusted to 2022 US dollars using the Consumer Price Index (CPI) published by the World Bank.23 Where the CPI rates were not available, the rates were estimated by taking an average of countries in the same HDI category in each region: Arab, East Asia and the Pacific, Europe, Europe and Central Asia, Latin America and the Caribbean, North America, South Asia, and Sub-Saharan Africa.Suture cost: The costs of plus antibacterial (triclosan-coated) and uncoated sutures were sourced from a systematic review and model-based economic evaluation that estimated the costs and outcomes of using the two types of sutures among abdominal surgery patients in the UK.15 The sutures are manufactured by Ethicon, J&J MedTech, and the costs were assumed to be the cost in all countries as this reflects the cost of procuring the suture from the manufacturer of the product. After converting the costs to 2022 US dollars, it was estimated that coated suture cost 28.21 23
Flow chart showing all data sources used in the model. Threshold analysis is a sensitivity analysis that is conducted to identify the value of a given parameter that alters the base case results in an analysis. Best/worst-case scenario is a sensitivity analysis that examines the combination of the most favorable/unfavorable values of parameters on the results of the analysis. HDI, Human Development Index; SSI, surgical site infection.
Outcome measures
This analysis estimated the preoperative and postoperative costs of patients with SSI within 30 days of an operation as defined by the US Centers for Disease Control and Prevention.24 SSI rates for coated and uncoated sutures were estimated to quantify and value the postoperative costs associated with each strategy. The timeframe for this evaluation was 30 days, in line with the timeframe for assessing SSIs used in the trial from which SSI rate estimates were sourced.2 The costs and effectiveness of the strategies were not discounted because the model timeframe was less than 1 year.25
Statistical analysis
To perform the modeling activity, several assumptions were made: (1) the only difference in pre, and intraoperative resource use and total costs between the arms was the cost of sutures, so the costs of the initial operation (other than the fascial suture cost) and postoperative care (other than the management of SSI) were not included in the model; (2) effect size of the triclosan-coated suture versus uncoated suture from the meta-analysis was applicable across all HDI countries because the meta-analysis pooled effectiveness data across country HDI categories11; and (3) uncoated suture was the standard practice in the hospitals that participated in the GlobalSurg 2 study.2 As such, the baseline rates reported in the study represented SSI rates for the uncoated suture arm. Bed-day unit costs were not available in eight countries, so they were estimated by taking the averages of countries in the same HDI category in the same region. Similarly, baseline SSI rates for 11 countries were not available and were imputed by taking averages of countries in the same HDI category in the same region. 26 countries had missing CPI data for some years and were also imputed by taking the averages of countries in the same HDI category in their respective regions (full list in online supplemental appendix S1).
We estimated the probability of each patient suffering an SSI after surgery and the expected cost of the SSI informed by the probability of suffering the SSI. However, we applied the 100% cost of suture to the patient in each arm as suture was used on the patient regardless of SSI status. The primary analysis estimated the difference in average total healthcare costs associated with an SSI between triclosan-coated suture and uncoated suture surgery in high, middle, and low-HDI countries separately. The analysis estimated the range of differences in costs associated with SSIs between the two groups based on the range of the effect size of the intervention. The lower and upper bounds of effect size from the meta-analysis (0.74, 1.09) were multiplied by the baseline SSI rates in each country and HDI categories to estimate the SSI rates in the intervention arm for each country and HDI categories.11 The absolute risk difference was estimated as the difference in SSI rates between the arms (uncoated minus coated suture arms). The cost difference per patient was estimated as the product of the absolute risk difference in SSIs and the average cost of an SSI plus the absolute difference in the cost of suture. The analysis conducted for the HDI categories was repeated for the country-level analysis to obtain estimates for the difference in costs associated with an SSI per patient by country as subgroup analyses.
The average cost difference per patient (CD) with coated suture versus uncoated suture was calculated as:
where CC is cost of coated suture, CU is cost of uncoated suture, RCS is SSI rate with coated suture, RUS is SSI rate with uncoated suture, CS is treatment cost per SSI, CBD is cost of bed-day, PHH is the proportion of hospital stay costs to all postoperative healthcare costs, LoS SSI is the average length of hospital stay for a patient with an SSI, and LoS no SSI is the average length of hospital stay for a patient without an SSI.
Subgroup analyses were performed to understand total costs by wound contamination group (ie, clean-contaminated or contaminated-dirty) to establish the effect of wound contamination in HDI stratified countries. The analysis was then repeated for each individual of the 193 countries on the HDI list based on specific healthcare-related costs.
Deterministic sensitivity analysis (DSA) was conducted to assess the sensitivity of the results to changes in the model input parameters. DSA assessed the impact of variation in suture cost, hospital stay costs, and the effect size. DSA involves varying one parameter while holding the rest of the parameters constant to assess the impact of the parameter being varied on the results.25 The following DSAs were conducted: (1) the costs of coated and uncoated sutures were varied upward and downward by 50%; (2) the estimated proportion of hospital stay costs to all postoperative healthcare costs was varied upward and downward based on the lower and upper bounds of the 95% CI (0.88 to 0.96) of this proportion; (3) threshold analysis was conducted to establish the effect size that would make the cost difference zero; and (4) best-case and worst-case scenario analyses were conducted. In the best-case scenario, the upper bound for the cost of uncoated suture (18) and the proportion of hospital stay costs to all healthcare costs (0.88), as the higher proportion reflects the lower cost of SSI. The worst-case scenario used the reciprocal bounds of those applied in the best-case scenario: the cost of uncoated suture (53), and the proportion of hospital stay costs to all postoperative healthcare costs (0.96). The primary analysis adopted a fully pooled multicountry costing approach that pooled both effectiveness data from all countries in a given HDI category and aggregated cost data from all the countries in a given HDI category.26 The subgroup analyses conducted at the country level applied country-specific effectiveness and cost estimates. All analyses were conducted in Microsoft Excel for Microsoft 365 V.2405.
Results
Baseline data
For clean-contaminated wounds, the average total cost difference between patients with and without an SSI was 456 in middle-HDI countries, and 12 238 in high-HDI countries, 646 in low-HDI countries (table 3).
Primary analysis
When all wounds were included in the model (clean-contaminated and contaminated-dirty), the average SSI-related cost per patient with coated suture in high-HDI countries ranged from 2019 compared with 466 or increased costs by 171 ([table 3](#T3)). Similarly, in middle-HDI countries, the mean SSI-related cost of coated suture ranged from 120 to 144 for uncoated suture, such that coated suture either reduced the costs by 18. In low-HDI countries, the average SSI-related cost of coated suture ranged from 208 compared with 34 or increased the costs by 175, 8 in average costs in high, middle, and low HDIs, respectively (online supplemental table S1).
Subgroup analysis: wound categories
Coated sutures reduced more costs in the contaminated-dirty wound category compared with the clean-contaminated wound category in all the three HDI categories (figure 2). In high-HDI countries, for example, coated suture saved up to 250 in the contaminated-dirty wound category compared with the clean-contaminated wound category, where it saved up to 97 (table 3).
Primary and sensitivity analysis results.
Country-level analyses
When all wounds were included in the model, the results were similar to the primary analysis in 184 of the 193 countries where coated suture could reduce or increase the SSI-related costs (online supplemental table S2). However, in nine countries, coated suture was associated with increased costs even when the effect size was 0.74. Higher cost savings were observed in high-HDI countries (online supplemental figure S2 and S3). For example, at the effect size of 0.74, the three biggest savings were observed in Brunei Darussalam (2833), and Ireland (3.30), Nepal (2.46) (online supplemental table S2). Similar results were observed for the clean-contaminated and contaminated-dirty subgroup analyses. In the clean-contaminated model, coated suture was associated with cost increases in 15 countries compared with seven countries in the contaminated-dirty model (online supplemental tables S3 and S4).
Sensitivity analysis results
The results by country HDI categories were sensitive to the effect size (online supplemental figure S1, S2 and S4) and sensitive when the cost of either coated or uncoated suture was reduced or increased by 50% for clean-contaminated dirty model (online supplemental appendix S3, online supplemental tables S5–S8). When the proportion of hospital stay costs to overall postoperative healthcare costs was adjusted downward and upward, the results were similar to the primary analysis (online supplemental tables S9 and S10). In all the changes to the suture costs or proportional hospital stay costs to all postoperative healthcare costs, coated suture could reduce or increase the costs associated with an SSI (table 4). The effect size that would make the cost difference zero was 1.00, 0.92, and 0.93 in high, middle, and low-HDI countries, respectively. In the best-case scenario, coated suture was associated with cost savings in all country HDI categories (online supplemental table S11). In the worst-case scenario, coated suture was associated with an increase in costs across all country HDI categories (online supplemental table S12).
Discussion
This study has demonstrated that, across health systems globally, uncertainty exists around potential cost savings when using triclosan-coated sutures to reduce SSI. These findings highlight the economic uncertainty, influenced by factors such as baseline SSI rates, wound contamination levels, and healthcare systems. While cost savings were more pronounced in contaminated-dirty wounds and high-HDI countries, uncertainties in the intervention’s effectiveness, reflected in a wide CI for its effect size, highlight the need for caution in policy and procurement decisions. This study does not justify routine use of triclosan-coated suture across all patients and whole health systems.
The subgroup and sensitivity analyses provide the necessary deeper insights into the variability and robustness of the results to justify the conclusions. Subgroup analysis revealed that cost savings were more significant in patients with contaminated-dirty wounds, highlighting the differential economic impact based on wound contamination levels. Sensitivity analysis demonstrated the stability of the findings under varying cost inputs and assumptions, identifying key parameters influencing cost differences. The main results were observed in 184 of 193 countries included in the country-level secondary analyses. However, in nine countries, coated suture was associated with an increase in costs even at the best possible effect size of the intervention.
A key strength of this analysis, based on the CI from a published meta-analysis of high-quality randomized trials, is its reliance on robust and reliable data, which strictly minimizes bias and enhances the validity of findings. By focusing exclusively on high-quality studies, this approach ensures that the economic analysis reflects evidence from well-designed trials with greater methodological rigor. However, a limitation of this approach is the exclusion of low-quality randomized trials, which often report overwhelmingly positive effects for interventions like triclosan-coated sutures. While these studies might exaggerate benefits, their exclusion might overlook potentially favorable scenarios. Despite the debate surrounding the decision to prioritize high-quality data, this analysis deliberately adopted this approach to ensure credibility and relevance, particularly as high-quality randomized trials now numerically and geographically (including high, middle, and low-HDI settings) outweigh the low-quality data, providing a more comprehensive evidence base. This model used the best available data, including the effect size and SSI rates from a real trial conducted across HDI settings. However, there are resource use variations and SSI incidence within and between countries that are not captured by the average data used in the model. Further, the analysis was based on the same level of effectiveness of the intervention globally. However, the effectiveness may vary between and within countries based on epidemiological factors and healthcare systems. Still, a wide range of sensitivity analyses were conducted on the effectiveness of the intervention at HDI categories and country level, and the results show that the intervention can reduce or increase the average costs, except in a few scenarios. The sensitivity analysis results on the suture costs indicate the price range that will be associated with cost increases or reductions. This range gives an indication to the industry on the feasible suture price range but also can help governments with negotiations on the suture reimbursement costs.
Cost savings were greater in high-HDI countries due to higher relative costs and input parameters compared with low- and middle-HDI countries, where healthcare costs are generally lower.16 In low- and middle-HDI countries, a significant proportion of patients incur out-of-pocket expenses, which were not accounted for due to the narrower healthcare perspective of this study.27 A broader societal perspective might reveal greater cost savings in these settings. Interestingly, middle-HDI countries showed lower costs than low-HDI countries, likely due to shorter lengths of stay, though the reasons for this difference remain unclear.
Results from three previous evaluations suggested that triclosan-coated sutures are potentially cost saving in SSI prevention. A US study reported cost reductions between 53 244 per SSI prevented, with higher savings when a societal perspective was used over a hospital or third-party perspective. Further, higher cost savings were noted when the likelihood of preventing SSIs increased.13 Similarly, a 2019 Italian hospital analysis estimated an annual savings of €14 785 (23 204 converted to 2022 US dollars in the current study).[12](#R12) An Egyptian hospital study projected an annual savings of 1 517 727 when using coated sutures for various surgeries.14 Also, a UK study estimated that triclosan-coated sutures were associated with 22 cost savings per patient and observed higher savings in non-clean wounds compared with clean wounds.[15](#R15) The point estimate of the current study reports cost reductions of 175, 8 when all wound categories are included in the model for high, middle, and low HDIs, respectively. While these studies align with the cost-saving potential of coated sutures, their findings differ from the current analysis, as they rely on central point estimate effect sizes rather than a CI-based approach that includes only high-quality trials.
This economic analysis is strengthened by its reliance on high-quality randomized trial data and global SSI baseline estimates, allowing for robust and comprehensive cost evaluations across 193 countries. These findings provide valuable insights for decision-makers at the country level. However, a key limitation lies in the CI of the effect size, which indicates that coated sutures may reduce or increase SSIs. This introduces uncertainty, particularly when the effect size exceeds 1, identifying the need for cautious interpretation of the results.
Future research should address the significant uncertainty surrounding the clinical effectiveness and economic impact of triclosan-coated sutures for SSI prevention in abdominal surgery. Further randomized trials should adhere to rigorous methodologies, as outlined in the recent systematic review and meta-analysis, to provide more definitive evidence on the effectiveness of triclosan-coated sutures compared with uncoated sutures.28 This study illustrates how economic analyses can successfully be based on clinical CIs, which can aid clinical policy making.
Supplementary material
10.1136/bmjsit-2025-000383online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ademuyiwa AO Hardy P Runigamugabo E et al Reducing surgical site infections in low-income and middle-income countries (FALCON): a pragmatic, multicentre, stratified, randomised controlled trial The Lancet 202139816879910.1016/S 0140-6736(21)01548-8PMC 858673634710362 · doi ↗ · pubmed ↗
- 2Bhangu A Ademuyiwa AO Aguilera ML et al Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study Lancet Infect Dis 2018185162510.1016/S 1473-3099(18)30101-429452941 PMC 5910057 · doi ↗ · pubmed ↗
- 3Andersson AE Bergh I Karlsson J et al Patients’ experiences of acquiring a deep surgical site infection: an interview study Am J Infect Control 201038711710.1016/j.ajic.2010.03.01721034980 · doi ↗ · pubmed ↗
- 4Perencevich EN Sands KE Cosgrove SE et al Health and economic impact of surgical site infections diagnosed after hospital discharge Emerg Infect Dis 2003919620310.3201/eid 0902.02023212603990 PMC 2901944 · doi ↗ · pubmed ↗
- 5Badia JM Casey AL Petrosillo N et al Impact of surgical site infection on healthcare costs and patient outcomes: a systematic review in six European countries J Hosp Infect 20179611510.1016/j.jhin.2017.03.00428410761 · doi ↗ · pubmed ↗
- 6Monahan M Jowett S Pinkney T et al Surgical site infection and costs in low- and middle-income countries: A systematic review of the economic burden P Lo S One 202015 e 023296010.1371/journal.pone.023296032497086 PMC 7272045 · doi ↗ · pubmed ↗
- 7Monahan M Glasbey J Roberts TE et al The costs of surgical site infection after abdominal surgery in middle-income countries: Key resource use In Wound Infection (KIWI) study J Hosp Infect 2023136384410.1016/j.jhin.2023.03.02337086854 · doi ↗ · pubmed ↗
- 8Kamarajah S Li E Ademuyiwa A et al Development of a risk of bias assessment tool specifically for meta-analysis of trials for surgical site infection Impact Surgery 20241240210.62463/surgery.99 · doi ↗