Mild Encephalitis/Encephalopathy With a Reversible Splenial Lesion (MERS) in an Adult: An Associated Finding in Severe Acute Pancreatitis With Multisystem Involvement
Nada Nfaoui, Mina Aallam, Safae Zahlane, Mohamed Chraa, Nissrine Louhab

TL;DR
A rare brain condition called MERS was found in an adult with severe pancreatitis and other health issues, showing the importance of recognizing this syndrome in adults.
Contribution
This paper reports an atypical adult case of MERS associated with severe multisystem involvement, expanding its clinical recognition in adults.
Findings
An adult with severe acute pancreatitis and neurological symptoms was found to have a MERS lesion.
The patient showed clinical and radiological recovery after supportive treatment.
The case emphasizes the need for awareness of MERS in adults with systemic infections and neurological symptoms.
Abstract
Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) is a rare clinico-radiological syndrome characterized by transient lesions of the splenium of the corpus callosum, typically occurring in the context of infections. While most frequently observed in children, adult cases remain infrequent and underreported. We present the case of a 30-year-old male patient with a preceding viral-like illness who was admitted for acute pancreatitis, renal failure, and neurological symptoms including confusion, dysarthria, ataxia, and postural tremors. An MRI of the brain revealed a reversible lesion in the splenium of the corpus callosum. Admission blood workup showed systemic inflammation, elevated inflammatory markers, and cytopenias, except cerebrospinal fluid (CSF) analysis and infectious serologies were unremarkable. The patient required hemodialysis and supportive management,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
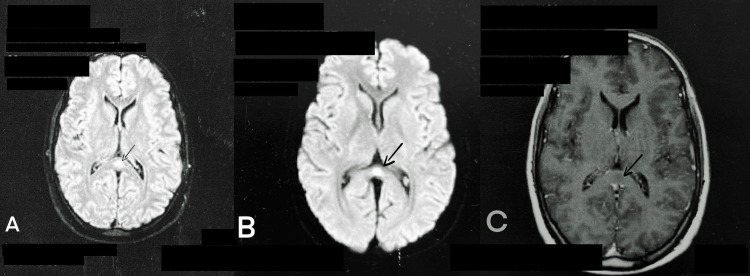 Figure 1
Figure 1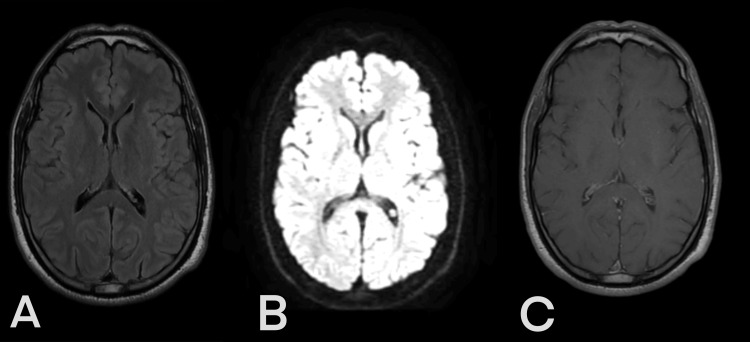 Figure 2
Figure 2| Values | Observed values | Normal range |
| Hemoglobin | 8.5 g/dL | 13-17 g/dl |
| Platelets | 108000 uL | 150 000-450 000 uL |
| Lymphocytes | 770 uL | 1000 -4000 uL |
| White cell count | 20800 uL | 4000-10000 uL |
| Ferritin | 3903 ng/ml | 30-400 ng/ml |
| Erythrocyte sedimentation rate (ESR) | 87 mm/h | 00-10 mm/h |
| Creatine kinase (CK) | 13502 UI/L | 39-308 UI/L |
| Neutrophils | 16510 Ul | 2000-7500 Ul |
| Urea | 3.87 g/l | 0.25-0.48 g/l |
| Creatinine | 121.2 mg/l | 07-12.00 mg/l |
| Human immunodeficiency virus (HIV) | Non-reactive | Non-reactive |
| Hepatitis C virus (HCV) | Non-reactive | Non-reactive |
| Hepatitis B surface antigen (HBsAg) | Non-reactive | Non-reactive |
| Venereal disease research laboratory (VDRL) | Non-reactive | Non-reactive |
| Aspartate aminotransferase (AST) | 96 U/L | 10.00-50.00 U/L |
| Alanine aminotransferase (ALT) | 74 U/L | 10.00-41.00 U/L |
| Alkaline phosphatase | 95 U/L | 40-129 U/L |
| Gamma glutamyl transferase (GGT) | 70 U/L | 10.00-71.00 U/L |
| C-reactive protein | 155 mg/dL | <6 mg/dL |
| Lactate dehydrogenase | 691 U/L | 0 - 250 |
| Lipase | 567 U/L | 13 - 60 |
| Prothrombin rate | 54.2% | 70%-100 % |
| International normalized ratio (INR) | 1.42 | 1.00 |
| Activated partial thromboplastin time (aPTT) | 23.5 sec | 30 - 35 sec |
| Mean corpuscular volume (MCV) | 81.9 fL | 80-100 fL |
| Mean corpuscular hemoglobin concentration (MCHC) | 34 g/dL | 32-35 g/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Bacterial Infections and Vaccines · Viral Infections and Immunology Research
Introduction
Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) is a clinical and radiological spectrum disorder called “reversible splenial lesion syndrome.” The splenium is the posterior part of the corpus callosum. Functionally, the corpus callosum allows the transfer of information from one hemisphere to the other and coordinates the responses of each hemisphere. Its anterior part, connecting the prefrontal cortices, is involved in cognitive functions, while its posterior, splenial part is involved in sensory functions. The usual clinical neurological features of MERS are mild central nervous system disorders such as seizures, confusion, and delirium. Other neurological symptoms include motor deterioration, slurred speech, neck stiffness, coma, tremor, ataxia, somnolence, dysarthria, visual disturbance, and dizziness. Affected patients usually recover completely without any sequelae within a month after the onset of neurological symptoms [1]. T2-weighted and fluid attenuated inversion recovery (FLAIR) brain MRI sequences show hyperintensities without contrast enhancement in the center of the corpus callosum, which resolve completely [2]. Usually, MERS is seen in children and is much less frequent among adults [3]. We describe a case of MERS in an adult with pancreatitis and severe kidney failure and review the literature on MERS in adults.
Case presentation
This is the case of a 30-year-old male patient admitted to the ER with the sudden onset of epigastric pain, melena, and kidney failure, preceded by flu-like symptoms a week before. On admission, the patient was drowsy and in a state of confusion. His past medical history was unremarkable, and there was no history of past or recent drug use or alcohol intoxication. Neurological examination revealed dysarthria, limb ataxia, and postural tremors. In addition, he presented generalized purpura.
Blood workup upon admission showed normochromic normocytic anemia, an elevated leukocyte count with bi-cytopenia (lymphocytes and platelets), and elevated serum markers of inflammation. There was further alteration of kidney function (creatinine 121.2 mg/l, blood urea nitrates 3.87 g/l). Infectious serology for human immunodeficiency virus (HIV), hepatitis B and C viruses, and syphilis was negative. Cerebrospinal fluid (CSF) analysis was normal (Table 1).
Brain MRI revealed one nodular lesion in the splenium of the corpus callosum (SCC). It was hypointense on T1, hyperintense on T2-weighted images, fluid-attenuated inversion recovery images (FLAIR), and diffusion-weighted images (DWI) and without contrast enhancement (Figure 1).
Brain MRI obtained on admission (axial view)(A) A hyperintense lesion in the splenium of the corpus callosum (SCC) on fluid‐attenuated inversion recovery images (FLAIR) (black arrow); (B) A hyperintense lesion in the SCC on diffusion-weighted imaging (DWI) (arrow); (C): no contrast enhancement on T-1 weighted images (arrow)
Workup for gastrointestinal symptoms revealed stage A pancreatitis on abdominal CT scan. There was also extensive wall thickening of the colon, suggesting an inflammatory origin. Thoracic CT revealed pneumomediastinum and micronodules likely of infectious origin, and no notable findings on the abdominal ultrasound.
After conditioning and blood transfusion, the patient underwent hemodialysis and was placed on dual antibiotic therapy for the pancreatitis. The overall evolution was favorable, with the improvement of both neurological and extraneurological symptoms. Cerebellar symptoms resolved within one month. Brain MRI performed two months after the onset of the condition revealed complete disappearance of the splenial lesion (Figure 2), and a second thoracic and abdominal CT done after two months also came back normal. The diagnosis of MERS was retained.
Brain MRI (axial view) obtained two months after the onset of the condition(A) Fluid‐attenuated inversion recovery image (FLAIR); (B) Diffusion‐weighted image (DWI); (C) T1‐weighted imaging
Discussion
It is a clinical-radiological neurological condition typically found in extraneurological infections. MERS is rare in adults. The novelty in the present case is the association with an infectious syndrome with systemic inflammation and multiorgan involvement.
The main neurological manifestation in our case was drowsiness and cerebellar involvement (dysarthria, ataxia, and postural tremors). According to a systematic review of 51 patients, neurological manifestations were preceded by prodromal symptoms in most patients (88%), with fever (78%) being the most common. Headache was the most common neurological symptom (50%), followed by seizures (22%) and altered consciousness (22%). Inflammatory changes in CSF were present in half of the patients [4]. Other general clinical symptoms include digestive tract disturbances (vomiting and diarrhea) [5, 6].
In this case report, the cause was probably a viral infection based on the patient's history and the fact that no germ was identified in our investigation. In 87% of the literature, MERS was found to occur in the context of an infection. Various germs (mainly viruses but also bacteria or parasites) can trigger MERS, but they failed to be identified in around 50% of the cases in a series by Grosset et al. [7]. It remains unclear why reversible splenial lesions selectively occur in the SCC, despite numerous pathology and neuroimaging studies. It could be that the specific affinity of viral antigens or induced antibodies to the splenial axonal receptors is responsible for the splenial involvement in viral encephalitis. Moreover, it has been speculated that the SCC has a specific vulnerability to excitotoxic injury in metabolic diseases, which makes this area selectively involved in different pathological events [8-11].
Typical MRI features are reversible hyperintense signals on T2-weighted images, FLAIR, and DWI. In addition, the apparent diffusion coefficient (ADC) of the lesion is decreased on ADC maps, and hypo- or isointense signals may appear on T1-weighted imaging sequences without contrast enhancement [1, 12]. The reversibility of lesions defines the syndrome and confirms the final diagnosis. This was the case with our patient.
Neurological symptoms are expected to disappear within a month, and isolated reversible lesions in the SCC are a good prognostic marker for a benign disease course in affected patients [3]. Although it is described as mild and reversible, the outcome isn’t always benign, as impaired consciousness or other system involvement may shift the prognosis to a more dire one, including death as a probable outcome. In contrast, there have been case reports of patients who presented with only fever or headache and without neurological symptoms [1].
Further research is required to better understand the mechanisms of MERS so that we can do better at predicting the disease's evolution and prognosis, all of which will help us give efficient care to the patient.
Conclusions
This case is a reminder of the possibility of MERS in adults and its possible association with severe multisystem disease. It is a clinical-radiological disorder that can manifest on a spectrum from headache to altered consciousness. The severity in our patient, other than his confusional state, entailed the extra-neurological involvement. This points to the importance of the associations or context of diagnosis of MERS as determinants of outcomes. This context should be clearly identified to allow for prompt, specific treatment of associated conditions. This may require exhaustive workup and collaboration with other specialties to manage patients, as was the case with our patient. While this case is a reminder of the possibility of MERS in adults, it should also serve as a reminder of the need for more work on the subject to better characterize the condition and help understand the underlying mechanisms of its occurrence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reversible lesion in the splenium of the corpus callosum Brain Behav Tetsuka S 09201910.1002/brb 3.1440 PMC 685181331588684 · doi ↗ · pubmed ↗
- 2Reversible splenial lesion syndrome (RESLES): what's in a name?J Neuroimaging Garcia-Monco JC Cortina IE Ferreira E Martínez A Ruiz L Cabrera A Beldarrain MG 01421201110.1111/j.1552-6569.2008.00279.x 18681931 · doi ↗ · pubmed ↗
- 3Mild encephalitis/encephalopathy with reversible splenial lesion (MERS) in adults-a case report and literature review BMC Neurol Yuan J Yang S Wang S Qin W Yang L Hu W 1031720172854541910.1186/s 12883-017-0875-5PMC 5445341 · doi ↗ · pubmed ↗
- 4Adult-onset of mild encephalitis/encephalopathy with reversible splenial lesion (MERS): case report and systematic review Neurol Sci Chiara R Vanessa P Nazerian P Gabriele V Antonio F Luca M Francesco A 518951994520243890490010.1007/s 10072-024-07627-0 · doi ↗ · pubmed ↗
- 5Two newly proposed infectious encephalitis/encephalopathy syndromes Brain Dev Takanashi J 5215283120091933912810.1016/j.braindev.2009.02.012 · doi ↗ · pubmed ↗
- 6Reversible splenial lesion syndrome in children: retrospective study and summary of case series Brain Dev Chen WX Liu HS Yang SD 9159273820162759111810.1016/j.braindev.2016.04.011 · doi ↗ · pubmed ↗
- 7Mild encephalopathy with reversible splenial lesion: description of nine cases and review of the literature Seizure Grosset L Hosseini H Bapst B 83868820213383956210.1016/j.seizure.2021.03.032 · doi ↗ · pubmed ↗
- 8Clinicoradiological spectrum of reversible splenial lesion syndrome (RESLES) in adults: a retrospective study of a rare entity Medicine (Baltimore) Zhang S Ma Y Feng J 094201510.1097/MD.0000000000000512 PMC 460273025674746 · doi ↗ · pubmed ↗