Comparative histopathologic analysis of COVID-19-associated pseudo-chilblains (“COVID-toes”), with idiopathic pernio, and chilblains lupus erythematosus
Taylor Harp, Tionna Szymanski, Haitao Chu, Zheng Wang, Jensen Fisher, Kevin J. Gaddis, David R. Pearson

Abstract
Click any figure to enlarge with its caption.
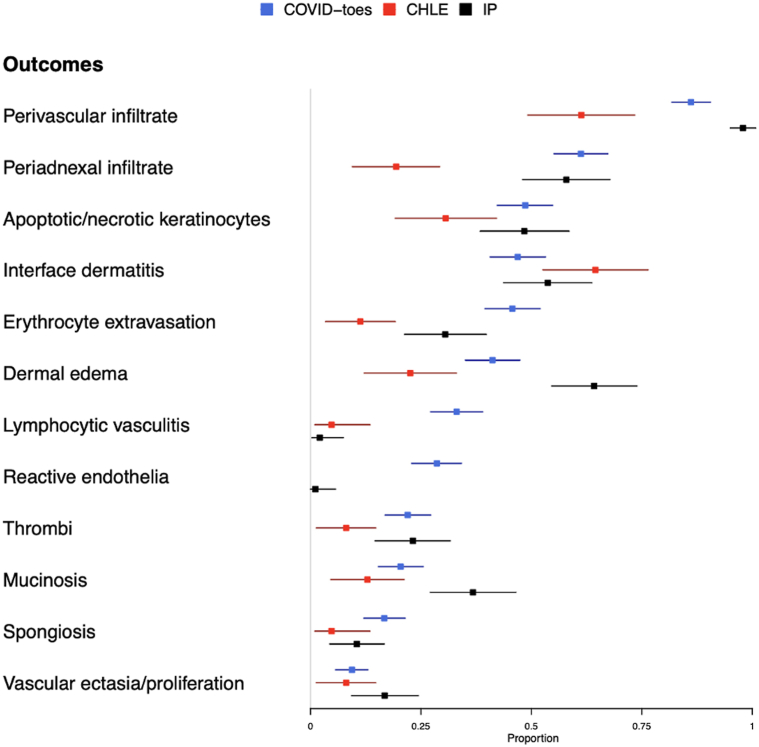 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological and COVID-19 studies · Body Contouring and Surgery · Skin Diseases and Diabetes
To the Editor: COVID-19-associated pseudo-chilblains (COVID-toes) presents as asymptomatic to tender, violaceous, acral subcutaneous papules. Its association with SARS-CoV-2 is debated because it often affects younger, asymptomatic patients with negative COVID-19 polymerase chain reaction results.1 COVID-toes may result from immunologic stimulation, direct viral effect, or an epiphenomenon from self-isolation. This study evaluates histopathology of COVID-toes and compares it to chilblains lupus erythematosus (ChLE) and idiopathic pernio (IP) in order to differentiate them.
A literature search was conducted to identify peer-reviewed, primary observational studies containing histopathologic data for COVID-toes, IP, and ChLE. 50 COVID-toes, 5 IP, and 5 ChLE articles were included. Explicitly reported (present or absent) histopathologic findings from biopsies of clinically diagnosed COVID-toes lesions were compared with IP and ChLE through common effect meta-analysis, using proportions and odds ratios (ORs).
ORs with 95% confidence intervals (CIs) and standardized mean differences (SMD) were calculated for histopathologic findings. Means and ORs with 95% CI were calculated for demographics. Further details Supplemental Materials, available via Mendeley at https://data.mendeley.com/preview/py7n8284gj?a=b0a4b242-c292-4cec-a1b1-9cd443aa3c66.2
COVID-toes patients were younger (25.8 years), compared with ChLE (40.76 years) and IP (41.95 years).2 Males were 13.2 times more likely to be diagnosed with COVID-toes than females when compared to ChLE (95% CI 5.4, 41.4), and 3.1 times more likely compared to IP (95% CI 1.9, 5.2).2
The most common histopathologic findings in COVID-toes were lymphohistiocytic perivascular infiltrate (86.1%), periadnexal infiltrates (61.2%; predominantly perieccrine), apoptotic or necrotic keratinocytes (48.6%), and interface dermatitis (46.9%; predominantly vacuolar). Other common findings were erythrocyte extravasation (45.7%), dermal edema (41.2%), lymphocytic vasculitis (33.1%), reactive endothelia (28.6%), and microthrombi (22%) (Table I and Fig 1).Table IAggregated proportions of histopathologic findings of COVID-19-associated pseudo-chilblains, ChLE, and IPHistopathologic FindingCOVID-toesChLEIPCOVID-toes vs ChLECOVID-toes vs IPnTotal NProportion (95% CI)nTotal NProportion (95% CI)nTotal NProportion (95% CI)OR∗ (95% CI)SMD∗OR∗ (95% CI)SMD∗Perivascular infiltrate2112450.861 (0.818, 0.905)38620.613 (0.492, 0.734)93950.979 (0.95, 1.008)3.901 (2.089, 7.269)0.5880.164 (0.033, 0.504)****0.445Periadnexal infiltrate1502450.612 (0.551, 0.673)12620.194 (0.095, 0.292)55950.579 (0.48, 0.678)6.367 (3.352, 12.934)****0.9441.15 (0.71, 1.855)0.068Apoptotic/necrotic keratinocytes1192450.486 (0.423, 0.548)19620.306 (0.192, 0.421)46950.484 (0.384, 0.585)**2.107 (1.183, 3.868)**0.3731.006 (0.627, 1.614)0.003Interface dermatitis1152450.469 (0.407, 0.532)40620.645 (0.526, 0.764)51950.537 (0.437, 0.637)0.492 (0.274, 0.865)0.360.765 (0.475, 1.226)0.135Erythrocyte extravasation1122450.457 (0.395, 0.52)7620.113 (0.034, 0.192)29950.305 (0.213, 0.398)6.236 (2.958, 15.051)0.8251.9 (1.16, 3.167)****0.317Dermal edema1012450.412 (0.351, 0.474)14620.226 (0.122, 0.33)61950.642 (0.546, 0.739)2.349 (1.267, 4.588)0.4080.394 (0.24, 0.638)****0.473Thrombi542450.22 (0.169, 0.272)5620.081 (0.013, 0.148)22950.232 (0.147, 0.316)2.975 (1.275, 8.398)0.3990.93 (0.536, 1.65)0.027Mucinosis502450.204 (0.154, 0.255)8620.129 (0.046, 0.21235950.368 (0.271, 0.465)1.656 (0.789, 3.869)0.2020.44 (0.263, 0.74)****0.37Spongiosis412450.167 (0.121, 0.214)3620.048 (0.01, 0.135)10950.105 (0.044, 0.1673.45 (1.267, 12.956)0.3911.652 (0.829, 3.567)0.182Reactive endothelia702450.286 (0.229, 0.342)NANANA1950.011 (0, 0.057)NANA****25.308 (6.743, 225.216)****0.84Lymphocytic vasculitis812450.331 (0.272, 0.39)3620.048 (0.01, 0.135)2950.021 (0.003, 0.074)8.422 (3.171, 31.233)0.77218.529 (6.221, 90.507)****0.89Vascular ectasia/proliferation232450.094 (0.057, 0.13)5620.081 (0.013, 0.148)16950.168 (0.093, 0.244)1.104 (0.445, 3.23)0.0470.509 (0.259, 1.018)0.222COVID-19-associated pseudo-chilblains (COVID-toes). Bold values indicate statistical significance.∗Unadjusted odds ratio (OR) between the diagnoses and histopathologic finding and tis 95% confidence interval were estimated by Firth logistic regression to reduce the bias that may by introduced by small numbers. The standardized mean differences (SMDs) for each histopathologic finding between Covid-toes vs CHLE, and between Covid-toes vs IP, were computed based on Yang and Dalton. SMD values >0.8 indicate a large difference between the 2 groups, 0.5-0.8 a medium difference, 0.2-0.5 a small difference, <0.2 a very small difference.Fig 1. Forest plot of the proportions of histopathologic findings observed in COVID-toes, ChLE, and IP.
Compared to ChLE, COVID-toes patients more often demonstrated perivascular (OR 3.901, 95% CI 2.089-7.269, SMD 0.588) and periadnexal infiltrates (OR 6.367, 95% CI 3.352-12.934, SMD 0.944), but less often had interface dermatitis (OR 0.492, 95% CI 0.274-0.865, SMD 0.36) (Table I and Fig 1). Compared to IP, COVID-toes patients more often demonstrated reactive endothelia (OR 25.308, 95% CI 6.743-225.216, SMD 0.84) and lymphocytic vasculitis (OR 18.529, 95% CI 6.221-90.507, SMD 0.89), but less often showed dermal edema (OR 0.394, 95% CI 0.240-0.638, SMD 0.473) (Table I and Fig 1).
The histopathologic patterns suggest a more vasculocentric inflammatory pattern in COVID-toes, possibly by SARS-CoV-2 infecting endothelium, leading to thrombosis and vasculitis.3 It has been postulated that IFN-I is upregulated, causing inflammatory damage, also a proposed mechanism in clustered cases of IP.2^,^4^,^5 Our study does not provide evidence to comment on this. This study is limited by the number of articles available, inconsistent data reporting, and inability for authors to review the slides to confirm findings.
Diagnosis of COVID-toes may be aided by demographics and histopathology. Younger males with vascular damage are more likely to have a diagnosis of COVID-toes, while older patients with perivascular and periadnexal infiltrates, particularly if interface dermatitis is observed, are more likely to have a diagnosis of IP or ChLE.
COVID-toes is a unique condition with distinct histopathology. While more biopsies and research are needed to differentiate these conditions and enhance diagnostic accuracy, this study provides valuable insights for diagnosis and future investigations.
Conflicts of interest
Dr Pearson is or has been a clinical trial investigator for Bristol-Meyers-Squibb, Corbus Pharmaceuticals, Elorac, Eli Lilly and Company, EMD Serono, Emerald Health Pharmaceuticals, Kadmon, Pfizer, and Soligenix, and has received consulting fees from Biogen and Pfizer within the last 3 years. Dr Wang is employed by a pharmaceutical company, Merck & Co, Inc. Authors Harp, Fisher, Szymanski and Drs Chu and Gaddis have no conflicts of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rocha K.O.Zanuncio V.V.Freitas B.A.C.Lima L.M.“COVID-toes”: a meta-analysis of case and observational studies on clinical, histopathological, and laboratory findings Pediatr Dermatol 38520211143114910.1111/pde.1480534515379 PMC 8646534 · doi ↗ · pubmed ↗
- 2Harp T.Pearson D.“Supplemental Material: Comparative Histopathologic Analysis of COVID-19-Associated Pseudo-Chilblains (“COVID-toes”), with Idiopathic Pernio, and Chilblains Lupus Erythematosus”2023 Mendeley Data, V 110.17632/py 7n 8284 gj.1 · doi ↗
- 3LabòN.Ohnuki H.Tosato G.Vasculopathy and coagulopathy associated with SARS-Co V-2 infection Cells 972020158310.3390/cells 907158332629875 PMC 7408139 · doi ↗ · pubmed ↗
- 4Hubiche T.Cardot-Leccia N.Le Duff F.Clinical, laboratory, and interferon-alpha response characteristics of patients with chilblain-like lesions during the COVID-19 pandemic JAMA Dermatol 1572202120220610.1001/jamadermatol.2020.432433237291 PMC 7689569 · doi ↗ · pubmed ↗
- 5Cordoro K.M.Reynolds S.D.Wattier R.Mc Calmont T.H.Clustered cases of acral perniosis: clinical features, histopathology, and relationship to COVID-19Pediatr Dermatol 373202041942310.1111/pde.1422732396999 PMC 7272804 · doi ↗ · pubmed ↗