Case report: A novel technique of robotic low-tension hiatal hernia repair using mediastinoplication
Carlos Eduardo Domene, Carlos Augusto Scussel Madalosso, Victor Ramos Mussa Dib, Paulo Reis Rizzo Esselin de Melo, André Valente Santana, William Carlos Giglio Mira Neto, Paula Volpe

TL;DR
This paper introduces a new robotic surgical technique called mediastinoplication to improve hiatal hernia repair and reduce recurrence.
Contribution
The novel use of robotic suturing to perform mediastinoplication for low-tension hiatal hernia repair is introduced.
Findings
Robotic surgery allows better access to mediastinal structures for precise suturing.
Mediastinoplication reduces tension and dead space, potentially lowering recurrence rates.
The technique aligns with surgical principles and shows promise for complex hiatal hernia cases.
Abstract
Surgery for giant hiatal hernias presents significant challenges, with laparoscopic surgery widely regarded as the gold standard. This approach typically involves complete resection of the hernia sac, thorough esophageal mobilization, tension-free closure of the diaphragmatic crura, and proper fundoplication. Despite various strategies to reduce recurrence, such as mesh reinforcement, there is no consensus on their superiority over traditional methods. Robotic surgery introduces greater precision, particularly in complex cases involving large hernias (grades III and IV). It facilitates safer dissections and more effective esophageal mobilization, challenging the concept of a short esophagus. A novel technique, mediastinoplication, addresses the positive abdominal-thoracic pressure gradient, a key factor in hernia recurrence. By reducing mediastinal dead space and approximating…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
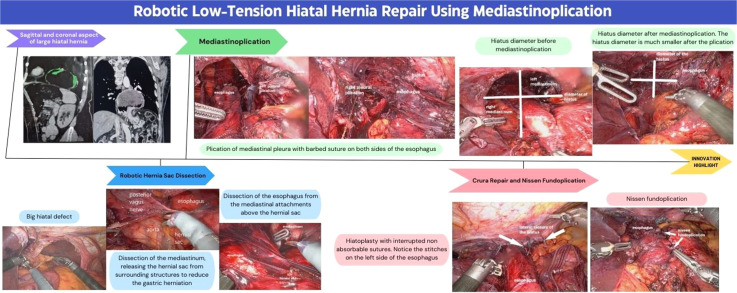 Figure 1
Figure 1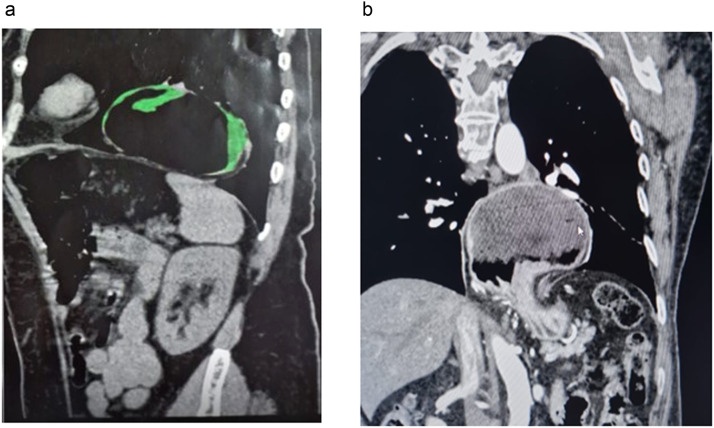 Figure 2
Figure 2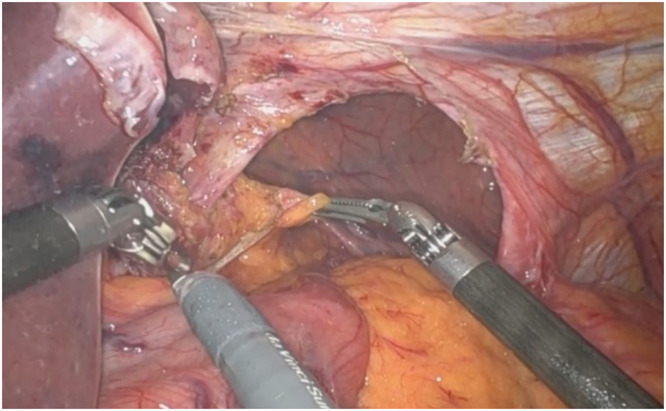 Figure 3
Figure 3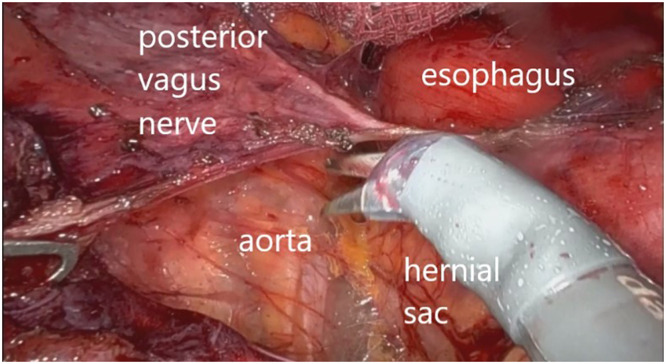 Figure 4
Figure 4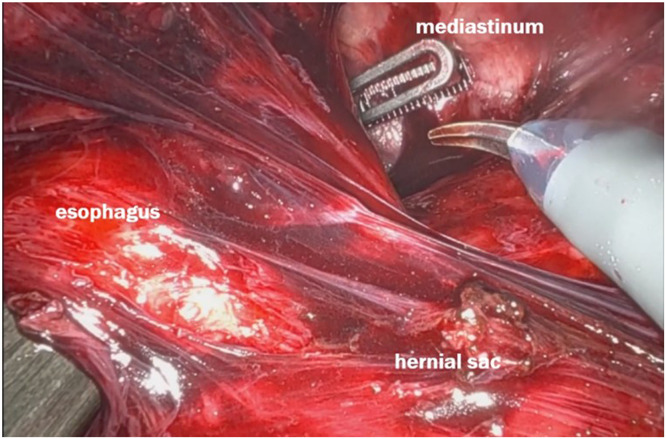 Figure 5
Figure 5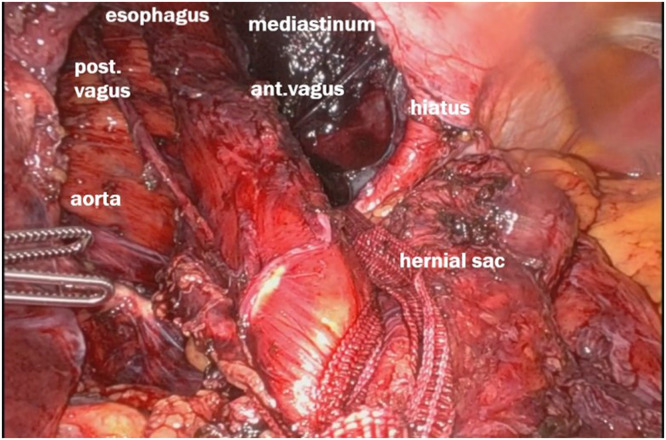 Figure 6
Figure 6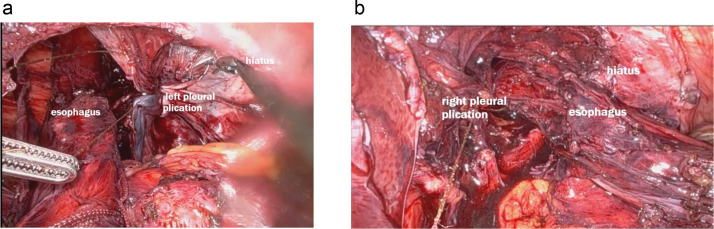 Figure 7
Figure 7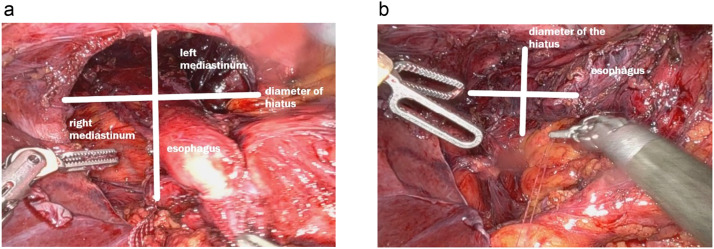 Figure 8
Figure 8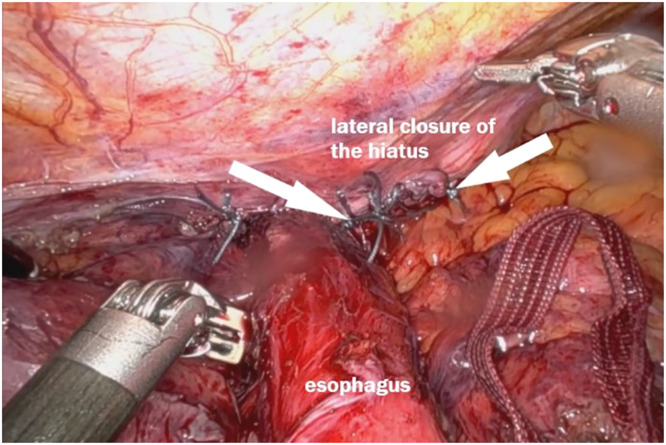 Figure 9
Figure 9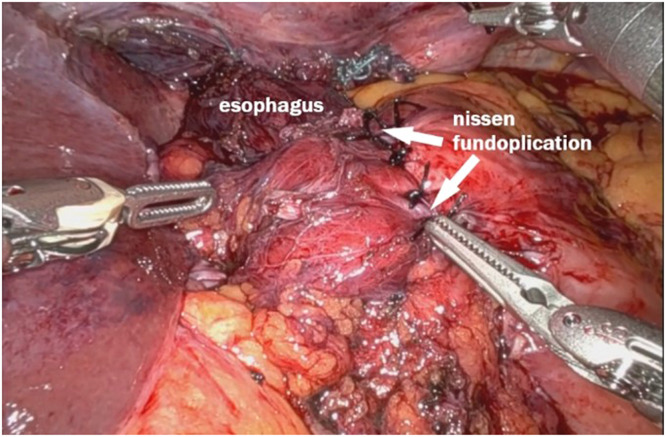 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Esophageal and GI Pathology · Congenital Diaphragmatic Hernia Studies
Specifications tableSubject area:Medicine and DentistryMore specific subject area:Robotic-assisted surgical techniques for the repair of giant hiatal hernias with mediastinal involvement.Name of your method:Robotic Low-Tension Hiatal Hernia Repair Using MediastinoplicationName and reference of original method:Not applicableResource availability:Robotic access
Background
Hiatal hernia repairs are commonly performed to treat symptomatic gastroesophageal reflux disease (GERD) and prevent recurrence. The standard procedure typically involves hernia sac dissection, crura repair, gastropexy and Nissen fundoplication [1]. However, in cases of giant hiatal hernias, recurrence is frequent [2] with significant mediastinal involvement, achieving a tension-free repair can be challenging [3] which leads to many different inconclusive interventions such as use of absorbable or non-absorbable mesh, relaxing incisions [4] use of ligament teres [5] or a left triangular ligament flap [6]. Here, we present a novel approach utilizing mediastinoplication as part of a robotic-assisted low-tension hiatal hernia repair, which we found effective in ensuring a durable and tension-free repair.
Method details
Patient presentation
A 65-year-old female, BMI 26.2Kg/m2, retired, on progesterone therapy, using PPI on demand, with a history of severe GERD presented with symptoms of dysphagia, regurgitation, and epigastric discomfort. Imaging studies, including an upper endoscopy, upper GI series and CT scan, revealed a large hiatal hernia with significant intrathoracic stomach and esophageal displacement – Fig. 1. No other comorbidities were referred. The patient was referred to surgical intervention.Fig. 1CT scan (right) showing sagittal and coronal aspect of large hiatal hernia with significant intrathoracic stomach and esophageal displacement.Fig 1
Surgical technique
Robotic hernia sac dissection
The patient was positioned supine and placed under general anesthesia. Using a robotic-assisted approach, trocars were inserted after the abdomen was insufflated. There was a big hiatal defect, with migration of almost all the stomach to the mediastinum – Fig 2. A complete dissection of the hernia sac was performed, with careful attention to avoid injury to surrounding structures, including the vagus nerves – Fig 3. The hernia sac was fully mobilized from the mediastinum, allowing for clear exposure of the crura and esophagus [7,8] – Fig 4.Fig. 2A big hiatal defect, with migration of almost all the stomach to the mediastinum.Fig 2. Fig. 3Dissection of the mediastinum, releasing the hernial sac from surrounding structures to reduce the gastric herniation.Fig 3. Fig. 4Dissection of the esophagus from the mediastinal attachments above the hernial sac.Fig 4
Esophageal mobilization
The next step involved a complete mobilization of the esophagus within the mediastinum [9]. The esophagus was carefully dissected free from its mediastinal attachments, ensuring adequate length for a tension-free repair. This step was critical for preventing postoperative recurrence and ensuring that the esophagus could lie comfortably within the abdominal cavity even before a crura repair had been performed – Fig 5.Fig. 5. Esophagus fully mobilized from mediastinum, with good abdominal length.Fig 5
Mediastinoplication
A novel aspect of this procedure involved the plication of the mediastinal fibers, mediastinal pleura, and pericardium on both the right and left sides with barbed sutures [10] – Fig 6. This plication served to reduce the mediastinal space and tension. This prevents the esophagus from migrating back into the thoracic cavity. Separate sutures were placed on each side to obliterate the wide space remaining after hernia reduction. The plication effectively reduced the hollow volume of the mediastinum, creating a tighter and firm environment to keep the esophagus in place – Fig 7.Fig. 6. Plication of mediastinal pleura with barbed suture on both sides of the esophagus.Fig 6. Fig. 7LEFT: Hiatus diameter before mediastinoplication. RIGHT: hiatus diameter after mediastinoplication. The hiatus diameter is much smaller after the plication.Fig 7
Crura repair
Following the mediastinoplication, a reduced tension was also observed in the crura. This allowed a natural approximation of the right and the left crura. A tension-free repair was done by using non-absorbable sutures. A sequential testing of bougie progression through the hiatus was done to ensure that the esophagus could pass freely without constriction or obstacle. This step was repeated until a satisfactory hiatus closure was achieved, with no tension and adequate space for the esophagus – Fig 8.Fig. 8. Hiatoplasty with interrupted non absorbable sutures. Notice the stitches on the left side of the esophagus.Fig 8
Nissen fundoplication
Finally, a Nissen fundoplication was performed using the mobilized abdominal esophagus. The stomach was wrapped 360 degrees around the esophagus to create a valve mechanism that would prevent reflux. Given the adequate esophageal mobilization and the reduction in mediastinal space achieved through the mediastinoplication, the fundoplication was completed without tension. The lack of tension is crucial in preventing postoperative dysphagia or recurrence ensuring long-term success – Fig 9.Fig. 9. Nissen fundoplication.Fig 9
Operative time
The total operating time lasted 3 h and 48 min, and did not have any complication.
This video (link1) demonstrates the Robotic Low-Tension Hiatal Hernia Repair Using Mediastinoplication.
Method validation
Postoperative course
The patient tolerated the procedure well and was extubated in the operating room. Postoperatively, the patient was started on a liquid diet and advanced to soft solids over the course of a week. She was discharged on postoperative day 2 with minimal discomfort. At the 6-week follow-up, the patient reported a complete resolution of her preoperative symptoms, including dysphagia and regurgitation. A follow-up upper GI series showed no evidence of esophageal obstruction. Upper endoscopy did not find abnormalities with a hiatus properly calibrated.
Limitations
We present a technique aimed at treating large and complex hiatal hernias characterized by an enlarged hiatus. This approach seeks to provide a safe, tension-free repair, eliminating the need for prostheses such as synthetic meshes. However, it is important to highlight certain limitations associated with the procedure, such as the requirement for robotic platforms to ensure safety during transhiatal mediastinal suturing, as well as adequate training in robotic surgery. Additionally, the results of this method must be monitored over time to identify potential recurrences or complications.
Ethics statements
The authors confirm that informed consent was obtained from the patient involved in the study. This consent included permission to use clinical data and images for research and publication purposes, ensuring compliance with ethical standards and patient confidentiality.
Related research article
None
CRediT authorship contribution statement
Carlos Eduardo Domene: Conceptualization, Methodology, Investigation, Resources, Writing – original draft, Visualization. Carlos Augusto Scussel Madalosso: Resources, Writing – original draft, Visualization. Victor Ramos Mussa Dib: Writing – review & editing. Paulo Reis Rizzo Esselin de Melo: Writing – review & editing. André Valente Santana: Writing – review & editing. William Carlos Giglio Mira Neto: Writing – review & editing. Paula Volpe: Supervision, Writing – review & editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leeder P.Smith G.Dehn T.Laparoscopic management of large paraesophageal hiatal hernia Surg. Endosc. Other Intervent. Tech.1720031372137510.1007/s 00464-002-9192-012820060 · doi ↗ · pubmed ↗
- 2Akmaz B.Hameleers A.Boerma E.G.Vliegen R.F.A.Greve J.W.M.Meesters B.Hiatal hernia recurrences after laparoscopic surgery: exploring the optimal technique Surg. Endosc.3762023443144423678147010.1007/s 00464-023-09907-w · doi ↗ · pubmed ↗
- 3Hanna N.M.Kumar S.S.Collings A.T.Pandya Y.K.Kurtz J.Kooragayala K.Management of symptomatic, asymptomatic, and recurrent hiatal hernia: a systematic review and meta-analysis Surg. Endosc.3862024291729383863017910.1007/s 00464-024-10816-9 · doi ↗ · pubmed ↗
- 4Ugliono E.Rebecchi F.Seno E.Morino M.Large hiatal hernia: minimizing early and long-term complications after minimally invasive repair Mini-invasive Surgery 2021112
- 5Chaudhry S.Farsi S.Nakanishi H.Parmar C.Ghanem O.M.Clapp B.Ligamentum teres augmentation for hiatus hernia repair after bariatric surgery: a systematic review and meta-analysis Surg. Laparosc. Endosc. Percutaneous Tech.344202439439910.1097/SLE.000000000000129538946644 · doi ↗ · pubmed ↗
- 6Ghanem O.Doyle C.Sebastian R.Park A.New surgical approach for giant paraesophageal hernia repair: closure of the esophageal hiatus anteriorly using the left triangular ligament Dig. Surg.32220151241282576642910.1159/000375131 · doi ↗ · pubmed ↗
- 7Watson D.I.Davies N.Devitt P.G.Jamieson G.G.Importance of dissection of the hernial sac in laparoscopic surgery for large hiatal hernias Arch. Surg.134101999106910731052284810.1001/archsurg.134.10.1069 · doi ↗ · pubmed ↗
- 8Arcerito M.Perez M.G.Kaur H.Annoreno K.M.Moon J.T.Robotic fundoplication for large paraesophageal Hiatal Hernias JSLS.241202010.4293/JSLS.2019.00054 PMC 706572932206010 · doi ↗ · pubmed ↗