Eosinophilic gastroenteritis in a 14-year-old patient with Noonan syndrome with a PTPN11 variation: a case report
Nobuhiko Koga, Shuichi Yatsuga, Kei Kubota, Toshikazu Niimi, Takahito Inoue, Shinichiro Nagamitsu

TL;DR
A 14-year-old girl with Noonan syndrome and a PTPN11 gene variation was diagnosed with eosinophilic gastroenteritis, a first in medical literature.
Contribution
This is the first reported case linking Noonan syndrome with eosinophilic gastroenteritis.
Findings
The patient had a PTPN11 gene variation and was diagnosed with eosinophilic gastroenteritis.
Eosinophilic gastroenteritis symptoms were managed with antihistamines and a leukotriene antagonist.
The PTPN11 gene variation may contribute to eosinophilic disorders via RAS/MAPK pathway activation.
Abstract
Noonan syndrome has a wide range of symptoms due to dysregulation of the RAS/MAPK pathway with several gene variations, including the PTPN11 gene. There are currently no case reports of Noonan syndrome with eosinophilic gastroenteritis. A 14-year-old Japanese girl was clinically diagnosed with Noonan syndrome. She had intermittent abdominal pain and vomiting from 10 years old. The patient was diagnosed with eosinophilic gastroenteritis on the basis of the pathological finding of multiple foci with > 20 eosinophils/high power field in the mucosal lamina propria of the colon by endoscopy at 12 years old. Vomiting and abdominal pain are currently being controlled by antihistamines and leukotriene antagonist therapy. Genetic testing showed the missense variation p.Ala72Gly in the PTPN11 gene. The pathogenesis of eosinophilic gastroenteritis is similar to that of other allergic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
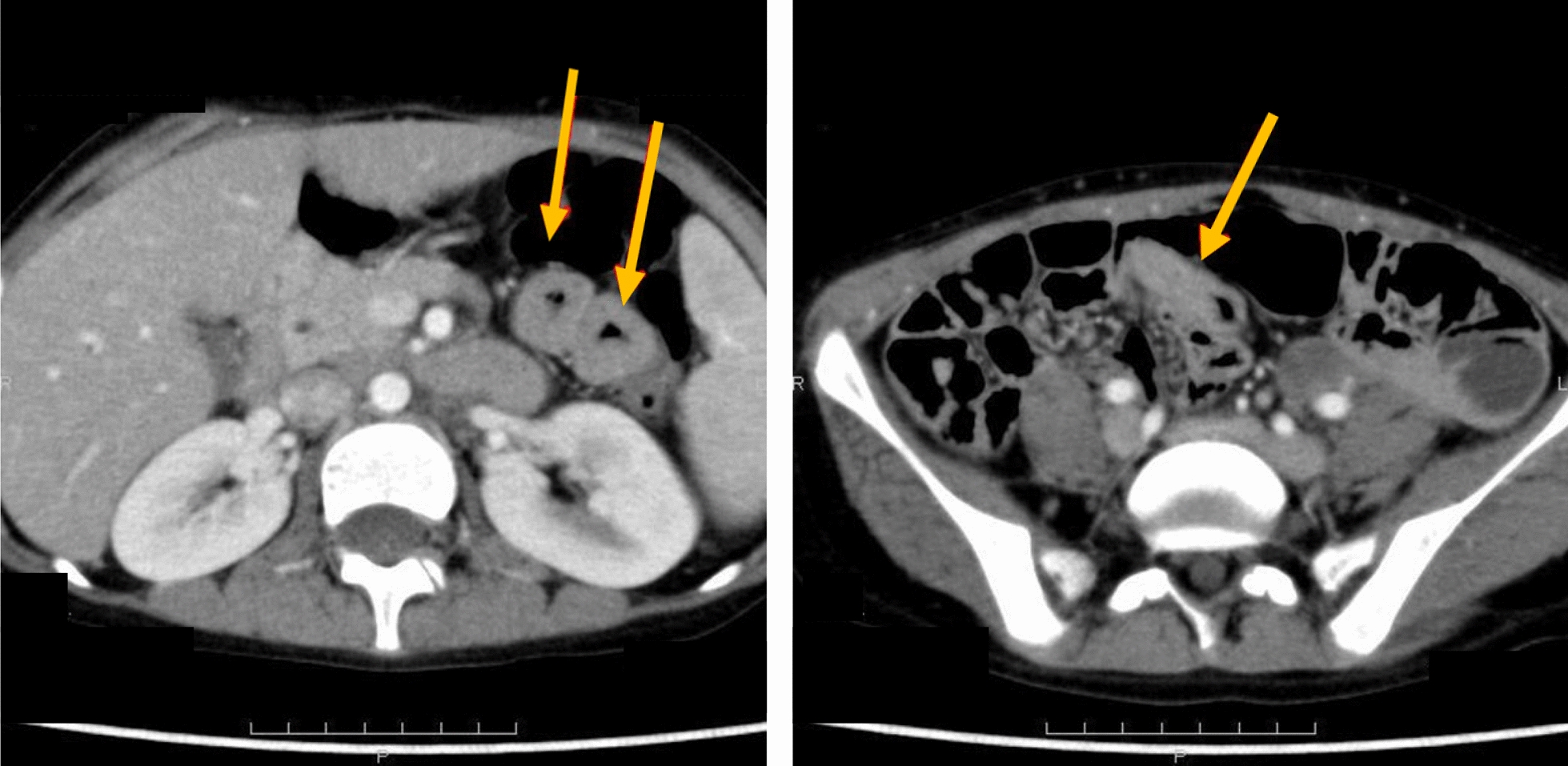 Figure 1
Figure 1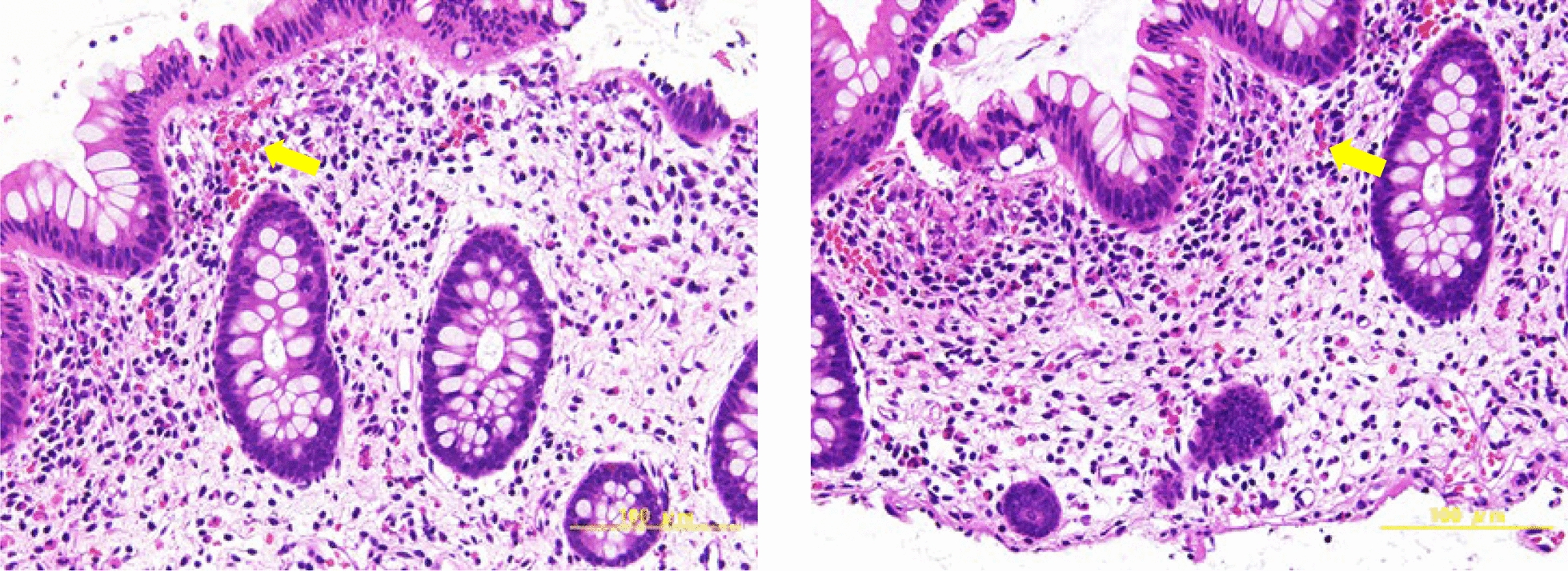 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Esophagitis · Eosinophilic Disorders and Syndromes · Gastrointestinal disorders and treatments
Background
Noonan syndrome (NS) is a genetic disease with a prevalence of 1 in 1000–2500 live births [1]. It is caused by several genes, with PTPN11 gene missense variations accounting for nearly 50% of cases [2]. NS may present with a number of symptoms, including a short stature, congenital heart disease, and characteristic facial features because of dysregulation of RAS/MAPK pathway [3].
Eosinophilic gastroenteritis (EGE) is a rare disease that is characterized by eosinophil infiltration of the gastrointestinal tract due to the release of cytokines, such as interleukin-5 (IL-5), which is associated with eosinophil differentiation and proliferation. EGE exhibits various symptoms, including abdominal pain, nausea, vomiting, diarrhea, and weight loss. Regarding affected ages and sex, EGE is found most frequent in middle age (30–50 years), and the sex ratio is reported to be roughly equal. Multiple therapeutic regimens have been used, such as corticosteroids, leukotriene antagonist therapy, and dietary restriction for EGE [4].
Although gastrointestinal symptoms occur in NS, there have been no case reports of NS complicated by EGE. We herein describe the first known case of EGE in a female patient with NS with a missense variation in the PTPN11 gene, including the genetic background; it may suggest a novel genotype–phenotype association.
Case presentation
The patient was a 14-year-old Japanese girl of non-consanguineous parents who was born at 36 weeks and 4 days of gestation with a birth weight of 3444 g and birth height of 50.0 cm. She was admitted to the neonatal intensive care unit (NICU) in our hospital due to neonatal hypercapnia. Pulmonary artery valve stenosis and an atrial septal defect were detected. She had no allergic diseases. There was no family history of allergic diseases. She had two half-siblings with no underlying diseases.
She was clinically diagnosed with NS on the basis of characteristic facial features, short stature, chest anomalies, developmental delay, and congenital heart diseases at 1 year old. A genetic analysis conducted at the Kazusa DNA Research Institute involved the analysis of the protein-coding regions of the PTPN11, SOS1, RAF1, RIT1, KRAS, NRAS, SHOC2, CBL, BRAF, SOS2, MRAS, RRAS, LZTR1, and RRAS2 genes. The analysis was performed using next-generation sequencing, focusing on rare variation with an allele frequency of 0.1% or lower. The genetic test revealed a missense variation, NM_002834.5:c.215C > G/NP_002825.3:p.Ala72Gly in the PTPN11 gene (ClinVar Variation ID: 13,325), which is classified as pathogenic/likely pathogenic on the basis of the ClinVar database and evaluated in accordance with the American College of Medical Genetics and Genomics (ACMG) guidelines. The classification is supported by evidence such as PS1 (same amino acid change with a different nucleotide substitution), PM1 (location in a mutational hotspot region associated with Noonan syndrome), and PP3 (deleterious predictions by multiple in silico tools). This finding aligns with the patient’s clinical features, supporting the diagnosis and enhancing our understanding of the genetic basis of the condition.
She struggled to adapt to school life from 10 years old onward, and continuously and simultaneously had mild abdominal pain, which was attributed to infectious enteritis, constipation, and stress associated with developmental delay. The patient was hospitalized for abdominal pain and vomiting for 1 week at 12 years old. Blood tests showed a white blood cell count (WBC) of 4700/µL (neutrophils 53.1%, lymphocytes 34.5%, and eosinophils 6.0%) and C-reactive protein (CRP) at 0.02 mg/dL. The patient is not taking any regular medications that may potentially induce eosinophilia in relation to their developmental delays. Contrast-enhanced computed tomography (CT) of the abdomen showed thickening of the intestinal wall and narrowing of the lumen with a contrast enhancement effect from the duodenum to the jejunum, but no neoplastic lesions in the abdominal cavity (Fig. 1).Fig. 1. Contrast-enhanced computed tomography of the abdomen: Intestinal wall thickening and lumen narrowing with contrast enhancement, observed from the duodenum to the jejunum, are indicated with arrows
Abdominal pain and vomiting were relieved by symptomatic medication. The patient was hospitalized due to the recurrence of frequent vomiting and severe abdominal pain 2 weeks after being discharged. Upper and lower endoscopies were performed, and a pathological examination showed multiple foci of eosinophils with an eosinophil count > 20/high power field (HPF) in the mucosal lamina propria of the colon (Fig. 2). EGE was diagnosed, and antihistamines were administered. She underwent second-line investigations, and infections, such as parasitic infections; allergies; drug-induced symptoms/conditions; inflammatory bowel disease; and systemic diseases were considered negative.Fig. 2. Pathological findings of lower gastrointestinal endoscopy: Multiple foci with an eosinophil count > 20 per high-powered field were detected in the mucosal intrinsic layer of the colon. Eosinophils are abundant in the specimen, and representative ones are indicated with arrows
She was hospitalized due to vomiting and severe abdominal pain 3 months later. Intravenous prednisolone and leukotriene antagonist therapy attenuated abdominal pain. Vomiting and abdominal pain are currently being controlled by antihistamines and leukotriene antagonist therapy. She underwent a follow-up colonoscopy 2 years later, which revealed chronic inflammation from the jejunum to the rectum and eosinophilic infiltration ranging from 35 to 70/HPF from the jejunum to the transverse colon.
Discussion
This case of NS was in a 14-year-old girl with recurrent vomiting and abdominal pain. EGE was diagnosed by upper endoscopy and a pathological examination. Abdominal symptoms are being controlled by antihistamines and leukotriene antagonist therapy [5].
EGE is difficult to diagnose because of its nonspecific gastrointestinal symptoms [5]. It is defined by symptoms of abdominal pain and/or diarrhea and the pathological finding of a dense eosinophilic infiltrate in the gastrointestinal wall. EGE is classified on the basis of the site of inflammation, and the threshold for eosinophil count determined by histological findings varies by location. An eosinophil count of ≥ 50/HPF in the colon is one of the diagnostic criteria, and this case was considered eosinophilic colitis on the basis of the clinical symptoms and histological findings [6]. Invasive examinations, such as laparoscopy and/or laparotomy, are often performed because a definitive diagnosis of EGE is difficult due to its nonspecific symptoms [7]. EGE is considered to be related to atopic and allergic factors, and causality appears to be driven by genetic factors, the gut microbiota, and environmental factors, particularly food allergens [8]; however, its etiology remains unknown [9]. Genetic factors related to EGE, such as TXN, PRDX2, NR3C1, GRB2, PIK3C3, AP2B1, and REPS1, have been reported [10]. PTPN11 gene variations may be one of the genetic factors for EGE; however, this needs to be confirmed on the basis of analyses of more NS cases with EGE. There may be an association, which needs further studies to confirm.
The PTPN11 gene is located on chromosome 12q24.13 in humans [11]. This gene spans approximately 163 kb and consists of 16 exons [12]. The PTPN11 gene encodes the protein SHP-2 [11], which belongs to the protein tyrosine phosphatase (PTP) family and plays a critical role in intracellular signal transduction [13]. The PTPN11 gene is the first identified and major NS disease gene, encoding SHP-2, that is found mutated in 50–60% of patients with NS [14]. The PTPN11 gene variation identified in Noonan syndrome are known as gain-of-function mutations of the RAS/MAPK pathway [15]. The activation of the RAS/MAPK pathway is essential for the differentiation of type-2 helper T cells, which subsequently promotes the production of IL-5 [16]. IL-5 is a key cytokine involved in eosinophilic inflammation and allergic responses, and the development of eosinophilic airway inflammation in a mouse bronchial asthma model are attenuated in transgenic mice by the overexpression of enzymatically inactive Ras molecules in T cells [17]. Therefore, the activation of RAS/MAPK pathway induces the production of IL-5 and allergic disease, such as bronchial asthma. It is well documented that patients with eosinophilic gastroenteritis demonstrate a high prevalence of allergy-related medical conditions, and IL-5 plays a crucial role in the pathogenesis of EGE [18]. Bronchial asthma has been reported as the most prevalent allergic comorbidity, representing more than 50% of cases with allergic history in EGE [19]. These findings suggest a potential pathophysiological link between NS, which results from RAS/MAPK pathway activation due to PTPN11 pathogenic variation, and eosinophilic disorders.
The codon Ala72 in the PTPN11 gene appears to be a mutational hotspot with multiple reported variants, including p.Ala72Gly, p.Ala72Asp, p.Ala72Val, p.Ala72Ser, p.Ala72Thr, and p.Ala72Pro [20, 21]. Functional studies have demonstrated that p.Ala72Val and p.Ala72Ser promote SHP-2 gain-of-function by destabilizing the catalytically inactive conformation of the protein, leading to prolonged signal flux through the RAS/MAPK pathway [20, 21]. For example, p.Ala72Val has been linked to hypertrophic cardiomyopathy and distinctive facial features [20]. In our study, we observed NS with p.Ala72Gly variation in the PTPN11 gene presented with EGE. Further studies, including functional and larger cohort analyses, are needed to confirm these findings and to better understand the full spectrum of clinical manifestations linked to Ala72 variants.
Although the present case had no allergic history and blood tests did not show an elevated eosinophil count, endoscopic pathology revealed an eosinophilic infiltrate. Difficulties are associated with identifying EGE on the basis of a history of allergy or blood test findings; therefore, we need to consider a thorough examination, including imaging and endoscopy, for recurring abdominal symptoms of NS.
Information on abdominal and allergic symptoms related to NS is limited, and the genetic relationship between EGE and NS currently remains unclear. Although abdominal symptoms in the present case may have been an accidental complication, this is the first case report of NS complicated with EGE. However, the association between NS with PTPN11 variant and EGE remains purely hypothetical, and the interpretation of causality represents a limitation of this case report.
Conclusion
We encountered a case of NS with a PTPN11 gene variant complicated by EGE. A molecular genetic link between PTPN11 mutations and EGE is suggested; however, the underlying mechanisms remain poorly understood. Further analysis of additional cases will be essential to elucidate this association.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tartaglia M., et al. (2006). Gain-of-function mutations in PTPN 11 in Noonan syndrome and related disorders. Nat Genet. 2006:37(6), 675–682.