Evaluation scale and behavioral model construction for intention to use postpartum exercise rehabilitation mobile application based on user experience
Zhiyuan Wang, Zheng Wang, Rong Deng, Meng Xia, Liming Huang

TL;DR
This study identifies key factors influencing postpartum women's intention to use exercise rehabilitation mobile apps and develops an evaluation scale and behavioral model to improve app design and user experience.
Contribution
The study introduces a new evaluation scale and behavioral model for postpartum exercise rehabilitation mobile app usage based on user experience.
Findings
Five key factors were identified that influence the intention to use postpartum exercise rehabilitation mobile apps.
Exercise safety assurance, physical activity tracking, emotional social support, and health benefits significantly affect user intention.
Dialogue support was found to have no direct effect on the intention to use these apps.
Abstract
Physical exercise is a widely recognized and practical approach to postnatal rehabilitation. In recent years, its delivery through mobile applications has become increasingly prevalent due to their accessibility and affordability. These mobile applications are crucial in supporting postpartum women in restoring physical and mental well-being and promoting sustainable health behaviors. The intention to use such mobile applications is a key determinant of user behavior and offers valuable guidance for designing and improving digital health services. Despite this, current research has largely overlooked the intention to use postpartum exercise rehabilitation mobile applications from the user experience perspective. This gap has contributed to a limited understanding of the specific needs of postpartum women, which are frequently underestimated or disregarded in the design process. This…
Click any figure to enlarge with its caption.
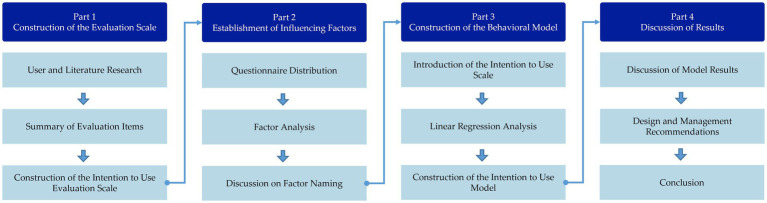 Figure 1
Figure 1 Figure 2
Figure 2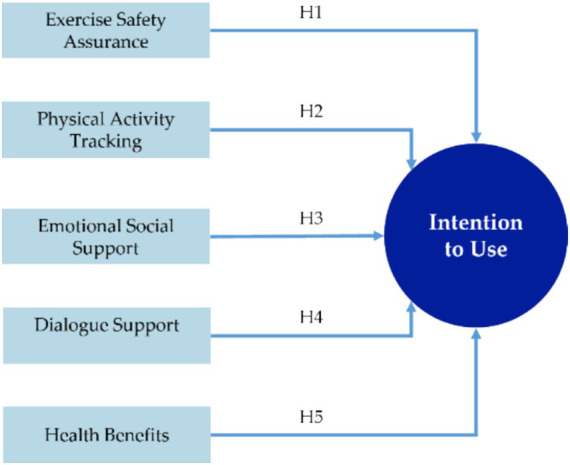 Figure 3
Figure 3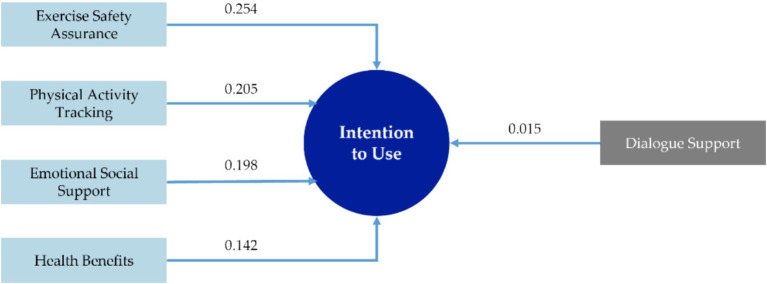 Figure 4
Figure 4| Research elements | Sources |
|---|---|
| Motivational Material, Social Support |
|
| Technological Affordances, Engagement, Motivational Technology |
|
| Barrier Identification and Resolution, Self-Efficacy, Self-Management, Achievable Goal Setting, |
|
| Social Support |
|
| Self-Efficacy, Capacity for Customizations, Self-Assessed, Usability, Ease of Navigation |
|
| Evidence-Based Exercise Guidance, Personalization, Progress Tracking, Social Support, Symptom Tracking, Usability, Ease of Navigation, Inclusivity |
|
| Perceived Severity and Susceptibility, Perceived Barriers, Perceived, Benefit, Cue-to-Action, Self-Efficacy, Social Support, Evidence-Based Exercise Guidance |
|
| Effectiveness |
|
| Engagement, Risk Perception, Responsibility, Functionality |
|
| Title | Option | Frequency | Percentage |
|---|---|---|---|
| Age group | 21 ~ 30 | 93 | 31.00 |
| 31 ~ 40 | 158 | 52.67 | |
| 41 ~ 50 | 29 | 9.67 | |
| 51 ~ 60 | 20 | 6.67 | |
| Educational background | Junior high school and below | 8 | 2.67 |
| High school vocational school | 15 | 5.00 | |
| Associate degree | 31 | 10.33 | |
| Bachelor’s degree | 168 | 56.00 | |
| Master’s degree | 72 | 24.00 | |
| Doctoral degree | 6 | 2.00 | |
| Occupation | Civil servant | 7 | 2.33 |
| State-owned enterprise | 34 | 11.33 | |
| Private enterprise | 202 | 67.33 | |
| Public institution | 36 | 12.00 | |
| Foreign-invested enterprise | 16 | 5.33 | |
| Student | 5 | 1.67 | |
| Total | 300 | 100.00 | |
| Item | Detailed description | Frequency | Source |
|---|---|---|---|
| Q1 | Personalized exercise rehabilitation plan customization | 58 | Literature Review ( |
| Q2 | Experts in the relevant field supervise and guide me during exercise | 53 | Literature Review ( |
| Q3 | Providing professional and effective exercise methods and techniques | 40 | Literature Review ( |
| Q4 | Effectively helps me recover from physical injuries caused by pregnancy | 32 | Literature Review ( |
| Q5 | Effectively reduces my weight and helps me achieve a good physique | 25 | Literature Review ( |
| Q6 | Regularly provide feedback on my physical changes | 25 | Literature Review ( |
| Q7 | Low-cost or free of charge items | 25 | User Survey |
| Q8 | Track and record various physical data indicators | 23 | Literature Review ( |
| Q9 | Flexible exercise duration | 23 | Literature Review ( |
| Q10 | Equipped with community interaction and communication features | 20 | Literature Review ( |
| Q11 | Improve physical fitness and restore my level of physical activity | 18 | Literature Review ( |
| Q12 | Teach me relevant knowledge and precautions regarding postpartum rehabilitation | 17 | Literature Review ( |
| Q13 | Provide dietary and nutrition plans during postpartum rehabilitation | 15 | User Survey |
| Q14 | Can provide support to motivate me to exercise | 14 | Literature Review ( |
| Q15 | Improve postpartum psychological issues and maintain mental health | 13 | Literature Review ( |
| Q16 | Equipped with notification and reminder functions to encourage me to exercise | 9 | Literature Review ( |
| Q17 | Can communicate online with doctors or relevant professionals | 9 | Literature Review ( |
| Q18 | Adjust the exercise intensity and plan in real time based on my actual exercise and physical condition | 8 | Literature Review ( |
| Q19 | Provide corresponding safety measures to reduce my exercise risks | 8 | Literature Review ( |
| Q20 | Engage in exercise in a group setting | 6 | Literature Review ( |
| Q21 | Help family and friends understand the importance of postpartum exercise | 6 | Literature Review ( |
| Q22 | Incorporates a reward mechanism | 5 | User Survey |
| Q23 | Data recording is accurate and effective | 5 | User Survey |
| Q24 | Able to assess the accuracy of exercise postures and provide corrections | 4 | User Survey |
| Q25 | Able to protect personal privacy and security | 3 | User Survey |
| Q26 | Timely update on the latest knowledge and exercise programs related to postpartum rehabilitation | 3 | User Survey |
| Q27 | Help me develop healthy lifestyle habits | 3 | Literature Review ( |
| Q28 | Can help me gain a sense of pride and confidence | 3 | Literature Review ( |
| Latent variable | Observed variable | Literature source |
|---|---|---|
| Intention to Use, ITU | If I plan to have a child in the near term, I will use a postpartum exercise rehabilitation mobile application in the near future |
|
| I am willing to use a postpartum exercise rehabilitation mobile application | ||
| I would recommend that others use a postpartum exercise rehabilitation mobile application |
| Item | Factor loading coefficients | Communality | |||||
|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | ||
| Q1 | 0.693 | 0.063 | 0.042 | 0.123 | 0.296 | −0.001 | 0.589 |
| Q2 | 0.683 | 0.156 | 0.207 | 0.096 | 0.063 | 0.196 | 0.585 |
| Q7 | 0.577 | 0.077 | 0.071 | 0.199 | 0.056 | 0.212 | 0.432 |
| Q9 | 0.466 | 0.141 | 0.514 | 0.094 | −0.064 | 0.292 | 0.599 |
| Q18 | 0.486 | 0.252 | 0.107 | 0.307 | 0.344 | −0.108 | 0.535 |
| Q19 | 0.667 | 0.256 | 0.031 | 0.057 | 0.039 | 0.204 | 0.558 |
| Q24 | 0.567 | 0.186 | 0.196 | 0.225 | 0.339 | −0.048 | 0.562 |
| Q3 | 0.120 | 0.413 | 0.140 | 0.569 | 0.142 | 0.001 | 0.548 |
| Q4 | 0.077 | 0.471 | −0.080 | 0.477 | −0.044 | 0.332 | 0.574 |
| Q6 | 0.054 | 0.704 | 0.273 | 0.247 | 0.166 | −0.038 | 0.663 |
| Q8 | 0.245 | 0.621 | −0.016 | 0.276 | 0.184 | 0.145 | 0.577 |
| Q23 | 0.369 | 0.583 | 0.286 | 0.025 | 0.272 | 0.047 | 0.634 |
| Q25 | 0.244 | 0.553 | 0.040 | 0.133 | 0.219 | 0.328 | 0.539 |
| Q26 | 0.228 | 0.581 | 0.334 | 0.085 | 0.116 | 0.153 | 0.545 |
| Q10 | 0.240 | 0.146 | 0.152 | 0.165 | 0.548 | 0.321 | 0.532 |
| Q20 | 0.085 | 0.256 | 0.096 | 0.085 | 0.657 | 0.190 | 0.558 |
| Q21 | 0.009 | 0.195 | 0.413 | 0.011 | 0.452 | 0.477 | 0.641 |
| Q14 | 0.061 | 0.244 | 0.686 | 0.128 | 0.053 | 0.136 | 0.571 |
| Q16 | 0.125 | 0.023 | 0.698 | 0.021 | 0.276 | 0.042 | 0.582 |
| Q22 | 0.079 | 0.093 | 0.805 | 0.008 | 0.082 | 0.014 | 0.671 |
| Q5 | 0.052 | 0.340 | 0.257 | 0.680 | 0.087 | 0.094 | 0.664 |
| Q11 | 0.291 | 0.288 | −0.044 | 0.657 | 0.096 | 0.080 | 0.617 |
| Q27 | 0.226 | −0.099 | 0.006 | 0.762 | 0.213 | 0.181 | 0.720 |
| Q28 | 0.254 | 0.094 | 0.158 | 0.200 | 0.688 | 0.009 | 0.612 |
| Q12 | 0.307 | 0.410 | 0.373 | 0.183 | 0.055 | 0.275 | 0.514 |
| Q13 | 0.200 | 0.033 | 0.173 | 0.351 | 0.228 | 0.490 | 0.486 |
| Q15 | 0.246 | 0.185 | 0.129 | 0.121 | 0.139 | 0.648 | 0.565 |
| Q17 | 0.379 | 0.226 | 0.017 | 0.075 | 0.333 | 0.318 | 0.413 |
| Before rotation | |||||||
| Eigenvalue | 9.359 | 1.974 | 1.563 | 1.164 | 1.049 | 0.978 | |
| Variance explained (%) | 33.426 | 7.049 | 5.583 | 4.157 | 3.748 | 3.494 | |
| After rotation | |||||||
| Eigenvalue | 3.462 | 3.141 | 2.748 | 2.677 | 2.297 | 1.762 | |
| Variance explained (%) | 12.364 | 11.217 | 9.813 | 9.561 | 8.203 | 6.294 | |
| KMO and Bartlett’s Test | |||||||
| KMO | 0.931 | ||||||
| Bartlett’s sphericity test | |||||||
| Item | Factor Loading Coefficients | Communality | ||||
|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | ||
| Q1 | 0.744 | 0.085 | 0.18 | 0.036 | 0.114 | 0.608 |
| Q2 | 0.712 | 0.165 | 0.155 | 0.169 | 0.066 | 0.591 |
| Q18 | 0.537 | 0.196 | 0.262 | 0.085 | 0.291 | 0.487 |
| Q19 | 0.712 | 0.254 | 0.01 | 0.055 | 0.096 | 0.584 |
| Q24 | 0.617 | 0.172 | 0.256 | 0.168 | 0.213 | 0.549 |
| Q6 | 0.053 | 0.717 | 0.138 | 0.241 | 0.227 | 0.645 |
| Q8 | 0.203 | 0.679 | 0.193 | −0.052 | 0.298 | 0.631 |
| Q23 | 0.38 | 0.596 | 0.229 | 0.263 | −0.005 | 0.621 |
| Q25 | 0.271 | 0.623 | 0.251 | 0.047 | 0.106 | 0.538 |
| Q26 | 0.224 | 0.642 | 0.124 | 0.311 | 0.081 | 0.581 |
| Q10 | 0.257 | 0.173 | 0.624 | 0.119 | 0.212 | 0.544 |
| Q20 | 0.15 | 0.265 | 0.703 | 0.049 | 0.051 | 0.592 |
| Q21 | 0.042 | 0.223 | 0.652 | 0.378 | 0.009 | 0.619 |
| Q28 | 0.297 | 0.07 | 0.64 | 0.123 | 0.23 | 0.57 |
| Q14 | 0.083 | 0.268 | 0.076 | 0.722 | 0.13 | 0.623 |
| Q16 | 0.13 | 0.047 | 0.269 | 0.703 | 0.046 | 0.587 |
| Q22 | 0.128 | 0.103 | 0.075 | 0.816 | −0.023 | 0.699 |
| Q5 | 0.088 | 0.34 | 0.101 | 0.27 | 0.667 | 0.651 |
| Q11 | 0.22 | 0.359 | 0.078 | −0.058 | 0.712 | 0.694 |
| Q27 | 0.214 | −0.014 | 0.203 | 0.006 | 0.806 | 0.737 |
| Before rotation | ||||||
| Eigenvalue | 6.984 | 1.77 | 1.316 | 1.096 | 0.987 | |
| Variance explained (%) | 34.919 | 8.851 | 6.58 | 5.481 | 4.934 | |
| After rotation | ||||||
| Eigenvalue | 2.869 | 2.783 | 2.235 | 2.228 | 2.038 | |
| Variance explained (%) | 14.345 | 13.913 | 11.176 | 11.142 | 10.188 | |
| Cronbach α | 0.793 | 0.811 | 0.727 | 0.718 | 0.734 | |
| KMO and Bartlett’s test | ||||||
| KMO | 0.918 | |||||
| Bartlett’s sphericity test | ||||||
| Factor | Item | Coef. | Std. Error | z |
| Std. Estimate | AVE | CR |
|---|---|---|---|---|---|---|---|---|
| Factor 1 | Q1 | 1 | – | – | – | 0.647 | 0.434 | 0.793 |
| Q2 | 1.158 | 0.122 | 9.47 | 0 | 0.668 | |||
| Q18 | 1.011 | 0.109 | 9.308 | 0 | 0.653 | |||
| Q19 | 1.028 | 0.115 | 8.919 | 0 | 0.619 | |||
| Q24 | 1.229 | 0.125 | 9.866 | 0 | 0.705 | |||
| Factor 2 | Q6 | 1 | – | – | – | 0.68 | 0.464 | 0.812 |
| Q8 | 0.885 | 0.088 | 10.035 | 0 | 0.664 | |||
| Q23 | 1.009 | 0.093 | 10.888 | 0 | 0.731 | |||
| Q25 | 0.926 | 0.094 | 9.854 | 0 | 0.65 | |||
| Q26 | 0.904 | 0.088 | 10.229 | 0 | 0.678 | |||
| Factor 3 | Q10 | 1 | – | – | – | 0.663 | 0.402 | 0.728 |
| Q20 | 0.935 | 0.107 | 8.708 | 0 | 0.613 | |||
| Q21 | 1.004 | 0.113 | 8.851 | 0 | 0.625 | |||
| Q28 | 1.077 | 0.12 | 8.944 | 0 | 0.634 | |||
| Factor 4 | Q14 | 1 | – | – | – | 0.689 | 0.461 | 0.719 |
| Q16 | 1.006 | 0.117 | 8.612 | 0 | 0.659 | |||
| Q22 | 1.152 | 0.131 | 8.794 | 0 | 0.687 | |||
| Factor 5 | Q5 | 1 | – | – | – | 0.669 | 0.48 | 0.734 |
| Q11 | 1.197 | 0.124 | 9.632 | 0 | 0.748 | |||
| Q27 | 1.021 | 0.114 | 8.958 | 0 | 0.657 |
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | |
|---|---|---|---|---|---|
| Factor 1 |
| ||||
| Factor 2 | 0.585 |
| |||
| Factor 3 | 0.557 | 0.572 |
| ||
| Factor 4 | 0.345 | 0.446 | 0.446 |
| |
| Factor 5 | 0.492 | 0.531 | 0.437 | 0.231 |
|
| Item | Factor loading coefficients | Communality | |||||
|---|---|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | ITU | ||
| Q1 | 0.745 | 0.086 | 0.185 | 0.036 | 0.109 | 0.077 | 0.616 |
| Q2 | 0.682 | 0.13 | 0.136 | 0.169 | 0.056 | 0.224 | 0.582 |
| Q18 | 0.541 | 0.201 | 0.276 | 0.08 | 0.281 | 0.102 | 0.505 |
| Q19 | 0.702 | 0.239 | 0.003 | 0.063 | 0.082 | 0.143 | 0.582 |
| Q24 | 0.596 | 0.136 | 0.222 | 0.163 | 0.202 | 0.252 | 0.554 |
| Q6 | 0.076 | 0.742 | 0.159 | 0.25 | 0.22 | −0.007 | 0.692 |
| Q8 | 0.209 | 0.693 | 0.205 | −0.046 | 0.29 | 0.068 | 0.657 |
| Q23 | 0.363 | 0.574 | 0.219 | 0.26 | −0.021 | 0.208 | 0.621 |
| Q25 | 0.224 | 0.567 | 0.206 | 0.044 | 0.08 | 0.369 | 0.559 |
| Q26 | 0.203 | 0.608 | 0.101 | 0.312 | 0.064 | 0.244 | 0.583 |
| Q10 | 0.225 | 0.143 | 0.598 | 0.117 | 0.2 | 0.234 | 0.537 |
| Q20 | 0.145 | 0.247 | 0.668 | 0.051 | 0.042 | 0.169 | 0.561 |
| Q21 | 0 | 0.172 | 0.606 | 0.378 | −0.009 | 0.293 | 0.626 |
| Q28 | 0.316 | 0.107 | 0.685 | 0.121 | 0.226 | −0.05 | 0.649 |
| Q14 | 0.06 | 0.233 | 0.058 | 0.719 | 0.123 | 0.19 | 0.63 |
| Q16 | 0.155 | 0.073 | 0.299 | 0.705 | 0.044 | −0.08 | 0.624 |
| Q22 | 0.126 | 0.089 | 0.059 | 0.812 | −0.02 | 0.072 | 0.692 |
| Q5 | 0.067 | 0.316 | 0.074 | 0.272 | 0.656 | 0.204 | 0.656 |
| Q11 | 0.22 | 0.362 | 0.081 | −0.059 | 0.701 | 0.117 | 0.694 |
| Q27 | 0.196 | −0.025 | 0.193 | 0.005 | 0.799 | 0.149 | 0.737 |
| ITU1 | 0.227 | 0.123 | 0.122 | 0.095 | 0.123 | 0.746 | 0.662 |
| ITU2 | 0.235 | 0.149 | 0.125 | −0.015 | 0.236 | 0.752 | 0.714 |
| ITU3 | 0.167 | 0.19 | 0.327 | 0.226 | 0.101 | 0.5 | 0.482 |
| Before rotation | |||||||
| Eigenvalue | 7.905 | 1.826 | 1.1 | 1.324 | 0.98 | 1.08 | |
| Variance explained (%) | 34.368 | 7.937 | 4.784 | 5.756 | 4.262 | 4.695 | |
| After rotation | |||||||
| Eigenvalue | 2.876 | 2.688 | 2.269 | 2.283 | 2.036 | 2.062 | |
| Variance explained (%) | 12.502 | 11.687 | 9.865 | 9.925 | 8.854 | 8.966 | |
| Cronbach α | 0.793 | 0.811 | 0.718 | 0.727 | 0.734 | 0.700 | |
| KMO and Bartlett’s test | |||||||
| KMO | 0.923 | ||||||
| Bartlett’s sphericity test | |||||||
| Factor | Item | Coef. | Std. Error | z |
| Std. Estimate | AVE | CR |
|---|---|---|---|---|---|---|---|---|
| Factor 1 | Q1 | 1 | – | – | – | 0.641 | 0.434 | 0.793 |
| Q2 | 1.171 | 0.124 | 9.47 | 0 | 0.669 | |||
| Q18 | 1.021 | 0.11 | 9.302 | 0 | 0.653 | |||
| Q19 | 1.033 | 0.116 | 8.879 | 0 | 0.616 | |||
| Q24 | 1.25 | 0.126 | 9.909 | 0 | 0.71 | |||
| Factor 2 | Q6 | 1 | – | – | – | 0.669 | 0.464 | 0.812 |
| Q8 | 0.891 | 0.091 | 9.849 | 0 | 0.657 | |||
| Q23 | 1.029 | 0.095 | 10.782 | 0 | 0.733 | |||
| Q25 | 0.956 | 0.097 | 9.877 | 0 | 0.66 | |||
| Q26 | 0.924 | 0.091 | 10.164 | 0 | 0.682 | |||
| Factor 3 | Q10 | 1 | – | – | – | 0.666 | 0.402 | 0.729 |
| Q20 | 0.931 | 0.106 | 8.798 | 0 | 0.612 | |||
| Q21 | 1.015 | 0.112 | 9.055 | 0 | 0.635 | |||
| Q28 | 1.052 | 0.118 | 8.906 | 0 | 0.622 | |||
| Factor 4 | Q14 | 1 | – | – | – | 0.689 | 0.461 | 0.719 |
| Q16 | 1.006 | 0.117 | 8.616 | 0 | 0.659 | |||
| Q22 | 1.152 | 0.131 | 8.796 | 0 | 0.687 | |||
| Factor 5 | Q5 | 1 | – | – | – | 0.671 | 0.48 | 0.734 |
| Q11 | 1.187 | 0.122 | 9.708 | 0 | 0.744 | |||
| Q27 | 1.022 | 0.113 | 9.044 | 0 | 0.659 | |||
| ITU | ITU1 | 1 | – | – | – | 0.663 | 0.447 | 0.707 |
| ITU2 | 1.006 | 0.105 | 9.571 | 0 | 0.714 | |||
| ITU3 | 0.95 | 0.109 | 8.721 | 0 | 0.625 |
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | ITU | |
|---|---|---|---|---|---|---|
| Factor 1 |
| |||||
| Factor 2 | 0.585 |
| ||||
| Factor 3 | 0.557 | 0.572 |
| |||
| Factor 4 | 0.345 | 0.446 | 0.446 |
| ||
| Factor 5 | 0.492 | 0.531 | 0.437 | 0.231 |
| |
| ITU | 0.559 | 0.549 | 0.525 | 0.315 | 0.465 |
|
| Hypothesis | Unstandardized coefficients | Standardized coefficients | t |
| Collinearity diagnosis | Result | ||
|---|---|---|---|---|---|---|---|---|
| B | Standard error | Beta | VIF | Tolerance | ||||
| H1 | 0.260 | 0.061 | 0.254 | 4.288 | 0.000** | 1.800 | 0.556 | Supported |
| H2 | 0.208 | 0.064 | 0.205 | 3.256 | 0.001** | 2.033 | 0.492 | Supported |
| H3 | 0.196 | 0.058 | 0.198 | 3.35 | 0.001** | 1.802 | 0.555 | Supported |
| H4 | 0.011 | 0.036 | 0.015 | 0.293 | 0.77 | 1.347 | 0.743 | Rejected |
| H5 | 0.135 | 0.052 | 0.142 | 2.613 | 0.009** | 1.523 | 0.657 | Supported |
| Factor | Recommendations |
|---|---|
| Exercise safety assurance | 1. Establish a multidisciplinary team of postnatal exercise rehabilitation experts. |
| Physical activity tracking | 1. Implement real-time tracking and recording of physiological and exercise-related data. |
| Emotional social support | 1. Establish an online community. |
| Health benefits | 1. Offer a comprehensive, medically-supported exercise rehabilitation program. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMobile Health and mHealth Applications · Diverse Approaches in Healthcare and Education Studies
Introduction
1
The postpartum period encompasses the puerperal phase, typically lasting 4–6 weeks following childbirth, and the subsequent recovery period extends from 6 months to 1 year. During this time, a woman’s physiological functions and hormone levels gradually return to a non-pregnant state. This phase represents a critical period of transformation in a woman’s life, marked by significant emotional vulnerability and profound changes across physiological, psychological, and social dimensions, creating a strong need for comprehensive recovery (Brites-Lagos et al., 2023). Throughout this period, women face a variety of postnatal conditions, including postpartum weight retention, pelvic floor dysfunction, rectal displacement, musculoskeletal pain, and postpartum depression (Tseng et al., 2015; Gebregziabher et al., 2020; de Castro et al., 2022), all of which can substantially affect their quality of life (Norhayati et al., 2015). As a result, postpartum rehabilitation has become a key area of maternal care and research (Skoura et al., 2024), aimed at preserving postpartum women’s physical and mental well-being. Physical exercise, as a cost-effective and straightforward approach to postpartum rehabilitation, has been shown to alleviate several postpartum conditions, significantly improve physical fitness (Tinius et al., 2022), and promote the development of healthy lifestyles (Lee et al., 2021). This makes it an essential component in safeguarding the health and well-being of women during the postpartum period (Bane, 2015). Recent research in physiology, psychology, and public health has demonstrated that exercise supports postpartum recovery by improving cardiovascular function (Mottola, 2002), strengthening pelvic floor muscles (Artymuk and Khapacheva, 2022), and promoting musculoskeletal health (Vladutiu et al., 2015). It also helps alleviate psychological and endocrine conditions such as postpartum depression, insomnia, stress, and role adjustment difficulties (Yang and Chen, 2018). Governments and organizations worldwide have increasingly recognized exercise as an essential recovery tool for women in the postpartum phase (Mottola et al., 2018; Birsner and Gyamfi-Bannerman, 2020; Campos et al., 2021; Brown et al., 2022). In conclusion, postpartum exercise rehabilitation not only serves as an effective means of improving physical health and preventing or treating various dysfunctions, but it also contributes to mental well-being by alleviating anxiety and depression, thereby helping women regain self-confidence and restore both their physical and psychological health.
In recent years, digital health has emerged as an innovative approach that leverages digital information and communication technologies to enhance health outcomes, improve healthcare services, and promote disease prevention. It has made significant contributions to public health development and the self-management of individual health, playing a crucial role in improving population health, enhancing healthcare efficiency and precision, and fostering the personalization of services (Hu et al., 2017; Brewer et al., 2020). mHealth, a key component of digital health, delivers reliable health information and interventions through low-cost, easily accessible methods, effectively promoting public health, particularly in underserved areas such as rural regions (Griffin et al., 2020). This is especially pertinent given the widespread adoption of smartphones and the large-scale deployment of 5G technology. mHealth offers a promising solution for managing, assessing, and supporting postpartum exercise rehabilitation. Research has demonstrated that mobile applications have become a primary tool for pregnant women to access health information and make health decisions (Brown et al., 2020). Among these, fitness and exercise apps are the most frequently used and downloaded health-related mobile applications, with evidence showing their positive influence on physical activity behaviors (Radzi et al., 2020). As a specialized subset, postpartum exercise rehabilitation mobile applications are designed to address the unique physiological and psychological needs of women during the postnatal period. These mobile applications provide flexible, low-cost exercise interventions that are not limited by time or environment, thereby supporting postpartum women in re-establishing a connection with their bodies (McGannon and McMahon, 2022), alleviating psychological stress (Lesser et al., 2023), and achieving various physical health benefits (DiPietro et al., 2019). Given their accessibility and targeted functionality, such mobile applications hold considerable potential for advancing women’s self-empowerment (Wolinsky, 1980), safeguarding postpartum mental health and well-being (Tinius et al., 2022), and improving health outcomes among women in low-income and resource-constrained settings (Tinius et al., 2021; Turner et al., 2023).
However, existing research on mobile applications for postpartum exercise rehabilitation presents several limitations. First, current mobile applications in the physical activity category and related studies often fail to address the specific characteristics of the postpartum population. In particular, there is a lack of mobile applications explicitly designed for postpartum exercise rehabilitation (Yu et al., 2022), which results in the needs of postpartum women being frequently underestimated or overlooked, despite the significant physical and psychological challenges they face during this period (Edie et al., 2021). Second, while existing research on postpartum exercise rehabilitation mobile applications tends to focus on the alleviation of various postpartum conditions (Radzi et al., 2020), the enhancement of women’s motivation to exercise (Tinius et al., 2022), and the functionality of the mobile applications (Tinius et al., 2021), it largely neglects the examination of postpartum women’s intention to use these mobile applications from the perspective of user experience. The intention to use, which refers to a user’s willingness or likelihood to engage with a technology or system in the future, is a crucial predictor of actual usage and reflects the user’s needs and interests in postpartum exercise rehabilitation (Davis, 1989). Additionally, although postpartum rehabilitation mobile applications can offer comprehensive health information and inclusivity, a lack of user-centered design may render these mobile applications ineffective in meeting the needs of the target population (Torous et al., 2018). While some studies have addressed user experience in the context of postpartum exercise rehabilitation, most of these investigations rely on established theories, scales, or literature-based identification of relevant factors. For instance, Rachel et al. employed the Mobile application Rating Scale (MARS) to evaluate postpartum women’s satisfaction with the BumptUp^®^ mobile application (Tinius et al., 2022), and applied the Health Belief Model to examine the barriers to and determinants of maternal physical activity in rural areas (Tinius et al., 2021). Although existing theoretical models have been extensively validated in the broader fields of health behavior and technology adoption, they have not been systematically applied to the specific context of postpartum exercise rehabilitation. Measurement scales derived from these models often lack sensitivity to the postnatal period’s unique physiological and psychological characteristics, rendering them only partially effective in assessing the intention to use mobile applications for postpartum exercise. As a result, such scales tend to be limited in scope and may introduce limitations into the evaluation process. Table 1 provides an overview of detailed studies on user experience in this context.
Therefore, this study draws on the established methodologies of Wang et al. (2022); Wang et al. (2023) and Xing and Jiang (2024), integrating qualitative research approaches, including user interviews, open-ended questionnaires, and literature review, with quantitative techniques such as factor analysis and linear regression. The study will systematically investigate the primary factors influencing postpartum women’s use of postpartum exercise rehabilitation mobile applications and the relationships between these factors and users’ intention to use. Based on these insights, the study aims to develop a targeted evaluation scale and a behavioral model of intention to use. This research holds significant theoretical and practical value by addressing gaps in existing theoretical frameworks, offering a clearer understanding of user behavior, and providing valuable insights to inform the design and optimization of postpartum exercise rehabilitation mobile applications.
Materials and methods
2
Research design
2.1
Building upon the previous discussion, this study will be conducted in four main parts, with the overall flow of the research depicted in Figure 1.
Research process.
The first part involves the construction of the evaluation scale. In this stage, the study will begin by collecting postpartum women’s assessments of postpartum exercise rehabilitation mobile applications through a literature review and user interviews. Industry experts will then summarize and review these assessments to finalize the evaluation scale for measuring the intention to use postpartum exercise rehabilitation mobile applications.
The second part focuses on identifying influencing factors. The evaluation scale developed in the previous section will be distributed as a questionnaire in this phase. Reliability analysis, exploratory factor analysis, and confirmatory factor analysis will be employed to identify the key factors influencing the intention to use postpartum exercise rehabilitation mobile applications. Subsequently, the factors will be named based on a thorough literature review concerning the specific items within each factor and the characteristics of postpartum exercise rehabilitation mobile applications, further clarifying the dimensions influencing users’ intention to use.
The third part involves constructing a behavioral model. At this stage, the study will investigate the relationship between the influencing factors identified in the second part and users’ intention to use the mobile application. First, this study will introduce a well-established “Intention to Use” evaluation scale during the questionnaire distribution phase in the second part of the research. It will be distributed alongside the evaluation scale developed in the first part to gather user feedback. Subsequently, exploratory and confirmatory factors will be conducted to ensure that the “Intention to Use” factor has good discriminant validity from the influencing factors established in previous research and that the observed variables within each factor demonstrate strong convergent validity. Following validation, linear regression analysis will be employed to examine the relationship between the influencing factors and intention to use, leading to the construction of a behavioral model of postpartum exercise rehabilitation mobile application usage intention based on the findings.
The fourth part focuses on discussing the results. At this stage, the study will analyze and discuss the relationships between the influencing factors and the intention to use, as identified by the model developed in the third part. Based on this analysis, the study will offer design strategies and management recommendations for designing and optimizing postpartum exercise rehabilitation mobile applications.
Participants
2.2
This study was primarily conducted within China, and its representativeness and research value can be justified from several perspectives.
First, China has a substantial population of postpartum women. According to the 2024 World Population Prospects report from the Population Division of the United Nations Department of Economic and Social Affairs, China is projected to have approximately 8.89 million newborns in 2023, ranking second globally (United Nations, 2024). This large cohort provides a robust sample for this study.
Second, China exhibits high Internet penetration and widespread acceptance of health-related mobile applications. By the end of 2024, the number of mobile Internet users had reached 1.17 billion, with a penetration rate exceeding 80%, encompassing nearly all women of childbearing age (Intelligence, 2024). Additionally, surveys indicate that 61% of Chinese citizens have recently used or are currently using mobile health applications, ranking among the highest globally (Statista, 2024). These figures suggest that the adoption and acceptance of postpartum mobile applications among Chinese women are likely equal to or greater than the global average. Therefore, conducting this study in China ensures access to a large and representative sample and enhances the study’s practical relevance and potential generalizability.
Third, the primary approaches to postpartum exercise rehabilitation in China align closely with those recommended by international authorities and widely adopted in developed countries (Health and Excellence, 2006; China, 2017; Syed et al., 2021; Zhu et al., 2022; Zhang et al., 2023). Although certain families in China continue to adhere to traditional cultural beliefs that discourage postpartum women from engaging in physical activity and encourage extended periods of rest (Pillsbury, 1978), the growing dissemination of modern medical knowledge and improvements in living standards have contributed to an increasing number of Chinese women embracing structured exercise to support their recovery (Zhu et al., 2022; Zhang et al., 2023). This trend indicates that the physiological and psychological recovery needs of postpartum women possess a degree of cross-cultural commonality, highlighting the potential universality of evidence-based postpartum rehabilitation practices.
In conclusion, this study highlights that investigating the intention to use postpartum exercise rehabilitation mobile applications in China offers significant advantages regarding universality and sample size. Such research can potentially contribute to optimizing and adopting such mobile applications.
In the user study phase, this research initially conducted in-depth interviews with 71 postpartum women who had participated in postpartum exercise to gather evaluations of the postpartum exercise rehabilitation mobile application. Of the respondents, 44 had used such mobile applications, while 27 had only received postpartum exercise rehabilitation training. This sample size meets the criteria for user interviews (Zhao et al., 2021; Wen et al., 2023). Subsequently, five postgraduate students, who had no vested interest in the study, and two university professors specializing in relevant fields, were invited to review and evaluate the results of the user interviews. Following this initial evaluation, 313 questionnaires were collected through the online platform “Credamo.” After a thorough review to eliminate invalid responses, such as those with unusually short response times, duplicate answers, or missing data, 300 valid questionnaires were retained, yielding a validity rate of 95.85%. This sample size is sufficient for factor analysis (Comrey and Lee, 1992; Price, 1993; Dai et al., 2020; Hair et al., 2021). All respondents were women who had either used the postpartum exercise rehabilitation mobile application or received structured postpartum exercise rehabilitation training. The demographic details of the respondents are presented in Table 2.
Construction of the evaluation scale
2.3
The process of constructing the evaluation scale for the intention to use the postpartum exercise rehabilitation mobile application is illustrated in Figure 2. This study draws on the established methodologies of Wang et al. (2022); Wang et al. (2023); Wang et al. (2025), which has been widely applied in various studies focused on user behavior research (Chen et al., 2024; Xing and Jiang, 2024). When the evaluation scales constructed using this method were distributed as questionnaires, the returned data exhibited high reliability and validity, yielding promising results in subsequent data analysis.
Construction process of the evaluation scale.
During the user research phase, this study utilized structured interviews to gather postpartum women’s evaluations of postpartum exercise rehabilitation mobile applications. The core interview questions were: “What advantages do you believe a postpartum exercise rehabilitation mobile application offers that would make you want to use it?” “What disadvantages do you perceive that would make you reluctant to use such an mobile application?” and “What features or elements should a postpartum exercise rehabilitation mobile application include to encourage your usage?” All participants were fully briefed on the study’s content and purpose before the interview, and their consent was obtained before proceeding. Participants were informed that they could terminate the interview at any time. For participants who had received postpartum exercise rehabilitation training but had not used relevant mobile applications, the study introduced “Kegel Exercise,” a widely used and highly rated mobile application in China, explicitly designed for postpartum women. Participants were familiarized with its functions through guided trial use. Once they had acquired sufficient familiarity with the mobile application, they continued to respond to the interview questions based on their rehabilitation experience and impressions of the mobile application. Ultimately, 427 original evaluations were obtained during the user study phase. To minimize potential bias and skewed data arising from a single source of evaluation, this study also supplemented the user data by collating relevant evaluations of postpartum exercise rehabilitation mobile applications from existing literature. In total, 486 evaluations were collected in the user study phase.
Next, the study consolidated evaluation items derived from the user research phase. Five graduate students with no vested interest in the research were invited to merge evaluation items with similar or identical content to ensure objectivity and reduce potential bias. Following this initial consolidation, two university professors with expertise in postpartum exercise rehabilitation were invited to review the results. In cases where discrepancies arose, the graduate students revised the items until both professors reached complete agreement. The consolidation process yielded 38 items. All negatively worded statements were rephrased into positive formulations to ensure consistency in phrasing. Moreover, to enhance data validity, items with a post-merging frequency of fewer than three responses were excluded from further analysis (Wang et al., 2023). As a result, 28 items were retained for developing the evaluation scale assessing the intention to use postpartum exercise rehabilitation mobile applications. These items are listed in Table 3.
To further investigate the intrinsic relationships between various influencing factors and users’ intention to use in subsequent studies, this research selected a well-established “Intention to Use” evaluation scale to gather postpartum women’s feedback on their use of postpartum exercise rehabilitation mobile applications. The chosen scale has demonstrated strong validity in measuring user intention and behavioral attitudes and has been widely cited in numerous studies. The specific content of the questionnaire is presented in Table 4. In adapting this evaluation scale for the study, the wording was modified to fit the context, replacing the research subject with postpartum exercise rehabilitation mobile applications to ensure relevance. The final evaluation scale was created by merging the summarized evaluation scale with the existing “Intention to Use” scale. This final scale will be published online as a seven-point Likert scale to gather user feedback. Before participants could provide input, a participant informed consent form was included at the beginning of the questionnaire. Respondents were required to read the form thoroughly and select the “Agree” option to proceed with the survey. Additionally, a screening question, “Have you used a postpartum exercise rehabilitation mobile application or undergone postpartum exercise rehabilitation training?” was incorporated to ensure that only respondents with relevant experience participated, enhancing the responses’ authenticity and validity.
Data analysis
2.4
In this study, an exploratory factor analysis was performed on the data from 300 respondents using SPSS 26.0 software, identifying five key factors. These factors included: exercise safety assurance (comprising items Q1, Q2, Q18, Q19, Q24), physical activity tracking (comprising items Q6, Q8, Q23, Q25, Q26), emotional social support (comprising items Q10, Q20, Q21, Q28), dialogue support (comprising items Q14, Q16, Q22), and health benefits (comprising items Q5, Q11, Q27). The Cronbach’s α values for each factor were above 0.7, indicating strong internal consistency and good reliability [68]. Subsequently, a confirmatory factor analysis was conducted using Amos 26.0 software, which confirmed that the factors exhibited satisfactory convergent and discriminant validity. This suggests that the user experience dimensions identified in this study are robust and coherent.
Building on these results, linear regression analysis was performed to examine the relationships between the identified factors and users’ intention to use the postpartum exercise rehabilitation mobile application. The analysis revealed that, except for dialogue support, all other factors directly impacted users’ intention to use the mobile application.
Results
3
Factor analysis results
3.1
Exploratory factor analysis
3.1.1
In this study, the user evaluation data presented in Table 3 were first subjected to exploratory factor analysis to identify the key elements influencing postpartum women’s intention to use the postpartum exercise rehabilitation mobile application. Upon importing the data into SPSS 26.0 software, six factors with eigenvalues greater than 1 were initially identified, as shown in Table 5. However, the analysis revealed some issues with factor entanglement, where the factor loading coefficients of certain items exceeded 0.4 across multiple factors. This indicated that these items did not exclusively correspond to a single underlying construct but were influenced by various constructs, undermining the distinctiveness between the factors. As a result, the factors failed to meet the criterion of one dimension corresponding to a set of questions, essential for ensuring valid and meaningful factor structures. This suggested that the initial exploratory factor analysis results were invalid. To address this issue, the study adopted a refinement approach based on the methodologies of Joshi et al. (2022), Wei et al. (2020), and Wang et al. (2022); Wang et al. (2023). Specifically, items exhibiting factor entanglement were sequentially deleted, and exploratory factor analyses were conducted after each deletion. This process continued until each observed variable was associated with a single factor, with a factor loading coefficient greater than 0.4. This iterative procedure was crucial for ensuring that the factor structure exhibited both high purity and discriminant validity. Other researchers have widely utilized and validated the approach, demonstrating its scientific rigor and credibility.
The results of the exploratory factor analysis were refined after the sequential deletion of items Q3, Q4, Q7, Q9, Q12, Q13, Q15, and Q17. Ultimately, five factors with eigenvalues greater than 1 were identified, with all factor loadings and communalities exceeding 0.4 for each item within the factors. Additionally, Bartlett’s test of sphericity yielded a p-value of 0.000 (<0.05), and the Kaiser-Meyer-Olkin (KMO) measure was 0.918 (>0.6), indicating that there were significant differences among the observed variables within each factor and strong correlations between them. These results demonstrate that the exploratory factor analysis was successful and met the requirements for factor validity (Kaiser, 1958). The final results are presented in Table 6. Subsequently, a reliability analysis was conducted, revealing that the Cronbach’s alpha for each factor exceeded 0.7, signifying good internal consistency and reliability of the data used in this study (Eisinga et al., 2013). This further supported the adequacy of the data for subsequent confirmatory factor analysis.
Confirmatory factor analysis
3.1.2
A confirmatory factor analysis was conducted to further assess the internal consistency of the observed variables within each factor and the discriminant validity among factors. The results in Table 7 indicate that the standardized factor loadings for all observed variables exceeded 0.5, the average variance extracted (AVE) values for all factors were above 0.36, and the composite reliability (CR) values were greater than 0.6. These findings suggest a strong correspondence between each factor and its associated items and satisfactory convergent validity across the scale (Shevlin and Miles, 1998; Muilenburg and Berge, 2005). In addition, the square root of the AVE for each factor exceeded the correlation coefficients between that factor and all other factors, as shown in Table 8. This demonstrates that each factor is empirically distinct, thereby confirming the discriminant validity of the measurement model. These results indicate that the intention-to-use evaluation scale developed in this study meets established criteria for reliability, convergent validity, and discriminant validity, supporting its applicability for assessing users’ intention to use postpartum exercise rehabilitation mobile applications.
Factor naming
3.1.3
The findings of the above analysis confirm that the five factors identified through factor analysis meet established research criteria. Accordingly, this study defines and names each factor based on the content of its associated items, supported by a comprehensive review of relevant literature, to clarify the conceptual dimensions they represent.
Factor 1 comprises five items: Q1, Q2, Q18, Q19, and Q24. These items emphasize the importance of incorporating safety measures into postpartum exercise rehabilitation mobile applications, including developing and adjusting personalized exercise programs. Such measures are intended to prevent physical injuries and avoid worsening postpartum health conditions during use. This is similar to the “Injury Prevention and Control” concept proposed by Ranney et al. and the “Efficacy and Safety” suggested by Dieter et al. Ranney et al. (2022) highlighted the pivotal role of remote monitoring and safety alerts in safeguarding users during exercise. Dieter et al. (2024) emphasized that expert guidance and in-app monitoring can significantly reduce the risk of exercise-related injuries. In addition, the American College of Sports Medicine (ACSM) has consistently emphasized the importance of exercise safety in successive editions of its guidelines for exercise testing and prescription (Medicine, 2013). Based on synthesizing these findings, this study designates Factor 1 as “Exercise Safety Assurance.” This construct refers to applying comprehensive methods to safeguard postpartum women during rehabilitation training and minimize the risk of injury or symptom exacerbation.
Factor 2 comprises five items: Q6, Q8, Q23, Q25, and Q26. These items collectively reflect the mobile application’s capabilities in data collection, feedback provision, accuracy of recorded information, privacy protection, and continuous knowledge updating. These elements address postpartum women’s need for comprehensive data management and individualized feedback regarding their physical condition. This factor aligns with the established “Physical Activity Tracking” concept within the broader framework of physical activity self-regulation (Ehlers and Huberty, 2014). Physical activity tracking involves using technological tools, such as wearable devices and mobile applications, to monitor, record, analyze, and provide feedback on an individual’s exercise behavior (Li et al., 2021). Prior studies have demonstrated that this process supports users in self-assessing their progress (Ehlers and Huberty, 2014) and enhances their health-related knowledge acquisition (Krebs and Duncan, 2015). Based on this conceptual alignment, Factor 2 is designated “Physical Activity Tracking.” It refers to a systematic approach to monitoring and evaluating postpartum physical activity through digital technologies, enabling users to track progress, receive timely feedback, and access personalized health information while ensuring data privacy and integrity.
Factor 3 comprises four items: Q10, Q20, Q21, and Q28. These items focus on fostering a supportive and non-judgmental environment for postpartum women by encouraging interpersonal communication and social support. These items aim to enhance users’ confidence and motivation to engage in physical activity. This aligns with the “Emotional Social Support” concept defined by House, who categorizes social support into four types: emotional, informational, instrumental, and appraisal support. Emotional social support specifically involves expressions of empathy, care, attentive listening, and encouragement, which help individuals feel understood and accepted (House, 1983). Beyond verbal reassurance, it also encompasses the sense of connection and belonging fostered through group interactions and shared experiences (Weiss, 1975; Barrera, 1986). Based on this conceptual correspondence, Factor 3 is labeled “Emotional Social Support” in this study.
Factor 4 comprises three items: Q14, Q16, and Q22. These items reflect mechanisms designed to encourage and motivate postpartum women to engage in physical activity, including regular encouragement, push notifications, and reward-based incentives. These elements closely correspond to the “Dialogue Support” concept outlined by Oinas et al. within the Persuasive Systems Design (PSD) framework, which identifies dialogue support as one of four core system functions. This concept refers to the interactive communication between a system and its user, aimed at promoting and sustaining desired behaviors through responsive feedback (Oinas-Kukkonen and Harjumaa, 2018). Such support simulates human interaction by offering timely reminders, suggestions, praise, and rewards, reinforcing the user’s motivation and commitment to the behavior (Orji and Moffatt, 2018; Oyebode et al., 2021). In light of this alignment, Factor 4 is designated as “Dialogue Support” in this study.
Factor 5 comprises three items: Q5, Q11, and Q27. These items reflect users’ perceptions of the postpartum exercise rehabilitation mobile application as effective in promoting weight loss, restoring physical fitness, and fostering healthy lifestyle habits. These features align with the broader concept of “Health Benefits,” which refers to the positive psychological and physiological outcomes of regular physical activity or structured exercise programs. Such outcomes include reduced risk of chronic illness, improved emotional well-being, and adoption of long-term healthy behaviors (Warburton et al., 2006). Accordingly, Factor 5 was designated health benefits in this study, capturing postpartum women’s expectations and subjective experiences regarding the physical and psychological improvements gained through the mobile application.
Model construction results
3.2
Hypothesis formulation
3.2.1
This study intends to employ linear regression analysis to examine further the relationships between the identified influencing factors and the intention to use the postpartum exercise rehabilitation mobile application. A behavioral model will also be constructed to understand better the users’ intention to use the mobile application. Before conducting the data analysis, the study proposes the following hypotheses, derived from the influencing factors identified in Section 3.1:
H1: “Exercise Safety Assurance” positively influences postpartum women’s intention to use the postpartum exercise rehabilitation mobile application.
H2: “Physical Activity Tracking” positively influences postpartum women’s intention to use the postpartum exercise rehabilitation mobile application.
H3: “Emotional Social Support” positively influences postpartum women’s intention to use the postpartum exercise rehabilitation mobile application.
H4: “Dialogue Support” positively influences postpartum women’s intention to use the postpartum exercise rehabilitation mobile application.
H5: “Health Benefits” positively influences postpartum women’s intention to use the postpartum exercise rehabilitation mobile application.
The hypothesized model is presented in Figure 3.
Hypothetical model of users’ intention to use.
For analysis, this study incorporated the well-established dimension of “Intention to Use” alongside the five identified factors to assess postpartum women’s intention to use the mobile application. To ensure that the inclusion of the “Intention to Use” dimension does not affect the other dimensions of the established evaluation scales, the study will combine the five factors with “Intention to Use” and perform both exploratory factor analysis and confirmatory factor analysis before conducting the formal linear regression analysis. This approach aims to verify strong discriminant validity between the six factors and that the items within each factor are appropriately aggregated.
Exploratory factor analysis of the behavioral model
3.2.2
In this study, exploratory factor analysis was employed to assess whether the inclusion of the “Intention to Use” dimension influenced the results of the evaluation scale developed. The findings in Table 9 indicate that the six factors are distinguishable, with the clustering of observed variables within each factor remaining unaffected by the other factors. Additionally, the evaluation scale’s results were not altered. Furthermore, the reliability coefficients for each factor exceeded 0.7, demonstrating satisfactory internal consistency. These findings support the suitability of confirming factor analysis for further validation.
Confirmatory factor analysis of the behavioral model
3.2.3
This study conducted confirmatory factor analysis to assess the degree of convergence among the observed variables within each factor and to evaluate the discriminant validity between factors. The results in Tables 10, 11 indicate that the standardized loadings of the observed variables for each factor exceed 0.5, the AVE values are greater than 0.36, and the CR values exceed 0.6. Additionally, the square roots of the AVE for each factor are higher than the correlation coefficients between that factor and the others. These findings suggest that each factor demonstrates strong discriminant validity and that the observed variables within each factor are well-converged. As such, the study is deemed suitable for further linear regression analysis.
Linear regression analysis
3.2.4
Building upon the theoretical assumptions outlined in Section 3.2.1, this study further examines the relationship between each factor and the intention to use the postpartum exercise rehabilitation mobile application through linear regression analysis. Factors 1 to 5 were treated as independent variables, with “Intention to Use” as the dependent variable. The results are presented in Table 12. The overall Durbin-Watson (DW) value is 1.906, and the Variance Inflation Factor (VIF) values for each path fall within the range of 0 to 10, indicating that the analysis is valid. The standardized regression coefficients for hypotheses H1 to H5 are 0.254, 0.205, 0.198, 0.015, and 0.142, respectively. The p-values for all hypotheses are below 0.05, except for H4, which has a p-value of 0.77, indicating that H1, H2, H3, and H5 are supported, while H4 is not. Based on these findings and the factor naming and linear regression analysis results, a behavioral model of users’ intention to use the postpartum exercise rehabilitation mobile application was developed, as shown in Figure 4.
Behavioral model of users’ intention to use the postpartum exercise rehabilitation mobile application.
Discussion
4
Discussion of model results
4.1
Based on the results of model construction, this study concluded that four factors, exercise safety assurance, physical activity tracking, emotional social support, and health benefits, significantly influence the intention to use the postpartum exercise rehabilitation mobile application. In contrast, dialogue support did not have a significant effect.
The path coefficient between exercise safety assurance and intention to use was the highest, at 0.254, indicating that exercise safety assurance is a core factor influencing postpartum women’s use of the mobile application. During the postpartum period, women are still undergoing physiological recovery. Fluctuations in hormone levels and reductions in muscle strength increase their vulnerability to injury, heightening their perception of exercise-related risks and potential complications (Soan et al., 2014; Tinius et al., 2021; Inge et al., 2022; Kettle et al., 2022). Mobile applications that provide evidence-based exercise guidance and professional supervision can reduce these perceived risks and significantly enhance exercise self-efficacy, increasing the likelihood of physical activity (Rosenstock, 1974; Bandura, 2004). Research by Evenson et al. also indicates that the perceived safety of exercise instructions substantially improves participation rates among postpartum women (Evenson et al., 2009). Therefore, exercise safety assurance addresses postpartum women’s most pressing safety concerns and functions as a foundational condition for the effectiveness of other features. It is critical in enabling safe participation, supporting habit formation, and strengthening the intention to use the mobile application. However, caution should be exercised to avoid overemphasizing exercise risks and safety warnings within the mobile application. Excessive emphasis on safety may intimidate users, ultimately diminishing their motivation to engage (Witte, 1992). Additionally, as individuals’ health status and birth experiences can vary widely, a one-size-fits-all solution often fails to meet the diverse needs of users (Pescatello, 2014). Exercise programs should be tailored to individual health status, functional capacity, and stage of recovery to minimize unnecessary risks of injury.
Physical activity tracking can directly influence users’ intention to use the postpartum exercise rehabilitation mobile application. This aligns with self-regulation theory (Carver and Scheier, 1982) and the PSD model (Oinas-Kukkonen and Harjumaa, 2018), both of which emphasize that self-monitoring (tracking steps, calories burned) enhances intrinsic motivation and persistence. Exercise tracking and progress management are key design elements for improving behavioral monitoring and feedback, strengthening users’ sense of purpose and commitment to their goals (Carver and Scheier, 1982; Locke and Latham, 2002; Gagnon et al., 2018). These features have been identified as some of the most favored by female exercisers (Ehlers and Huberty, 2014; Li et al., 2021). In the context of postpartum exercise rehabilitation, physical activity tracking can enhance the perceived utility and value of the mobile application. It significantly contributes to the perceived usefulness of the mobile application among postpartum women, thus boosting their motivation to exercise and increasing their intention to use the mobile application. However, concerns regarding data privacy may hinder some users’ willingness to engage with the mobile application (Malhotra et al., 2004; Hernandez et al., 2011). Therefore, it is crucial to implement robust privacy protections during data tracking to alleviate such concerns.
Emotional social support can directly influence users’ intention to use the postpartum exercise rehabilitation mobile application. The companionable and interactive features of the mobile application, coupled with the encouragement and support from family and friends, can make postpartum women feel understood and motivated to engage in physical activity. Social behavior theory suggests that support for family, friends, or peers effectively enhances adherence to health behaviors (Cohen and Wills, 1985). Emotional support is particularly crucial during the postpartum period, when mothers often experience both physical and psychological stress. Empirical studies have shown a positive association between social support and physical activity levels in postpartum women (Bennetter et al., 2023), with cooperation and companionship from family members and peers significantly increasing exercise participation (Evenson et al., 2009). Thus, incorporating social features into mobile applications can enhance user engagement and increase postpartum mothers’ intention to use the mobile application. However, the effectiveness of emotional social support is limited by the user’s social network’s activity level and cultural dynamics. For users who are more isolated or uncomfortable with online sharing, the impact of this support may be reduced (Thoits, 2011). Furthermore, while virtual social interaction can be beneficial, it cannot fully replace the value of real-life companionship, and social features should not be relied upon as a sole means of addressing emotional needs (Rains and Young, 2009). Therefore, it is essential to focus on evidence-based education regarding exercise rehabilitation, which can improve family and friends’ understanding of and support for postpartum women’s behaviors.
The health benefits factor has the smallest path coefficient of 0.135, indicating a weaker effect on the intention to use than the other factors. This may be attributed to health benefits being categorized as an “Outcome Expectation,” representing a more future-oriented cognitive evaluation (Bandura, 2004). As a result, users tend to assign less importance to such long-term outcomes when making decisions (Frederick et al., 2002). Empirical research indicates that the motivational influence of distant outcomes is generally weaker than that of immediate self-efficacy-related experiences. As such, postpartum women, who are uncertain about their future recovery, are more likely to prioritize immediate, visible risk signals or benefits over potential future health improvements. Nonetheless, health benefits remain a crucial factor influencing the adoption of new technologies or products. This aligns with the concept of “Perceived Usefulness” in both the Health Belief Model (Champion and Skinner, 2008) and the Technology Acceptance Model (TAM) (Davis, 1989), which suggests that individuals are more inclined to use a mobile application when they believe it will yield significant benefits. From a postnatal health perspective, exercise has been shown to alleviate symptoms of postnatal depression and anxiety, aid in returning to pre-pregnancy weight, and enhance physical strength (DiPietro et al., 2019; Brites-Lagos et al., 2023). However, caution is necessary to avoid overstating or exaggerating the potential effects of exercise rehabilitation within mobile applications. Overpromising results may lead to unrealistic expectations among postpartum women (Oliver, 1980; Bhattacherjee, 2001), resulting in user disengagement if the promised benefits are not realized.
The linear regression analysis revealed that H4 does not hold, indicating that dialogue support does not directly affect users’ intention to use the mobile application. Several factors may explain this outcome. First, postpartum women often face significant time constraints and prefer quick and convenient access to information (Evenson et al., 2009). As such, frequent interactions with dialogue support may be perceived as an additional burden, conflicting with the user’s demand for simplicity and ease of use (Ng et al., 2024). Second, overly frequent or undifferentiated push notifications can lead to alert fatigue, where users become desensitized to the notifications or choose to block them, thus diminishing their effectiveness in influencing behavior (Mehrotra et al., 2016). Furthermore, encouragement, reminders, and rewards are external incentives. Existing research suggests that users’ behavior and intention to use are primarily driven by intrinsic motivation (personal interest, values, and satisfaction) and the tool’s inherent usefulness and usability, rather than by additional interactive features (Cerasoli et al., 2014; Ng et al., 2024). The impact of external incentives is considerably reduced if users lack interest in the activity or do not perceive it as contributing to their goals. Self-Determination Theory (SDT) also posits that excessive reliance on external incentives can undermine intrinsic motivation (Deci et al., 1999). Consequently, balancing external incentives with inherent motivation is crucial when designing postpartum exercise rehabilitation mobile applications. For example, incorporating progressive rewards can enhance users’ self-efficacy and sense of achievement, while personalized reminder frequencies can help avoid repetitiveness and prevent feelings of coercion.
Additionally, as the sample in this study predominantly consists of participants from China, the results may be influenced to some extent by traditional Chinese cultural values, particularly in the areas of “Exercise Safety Assurance” and “Emotional Social Support.” In the traditional Chinese “postnatal confinement” culture, new mothers are often encouraged to rest at home and avoid strenuous physical activity to promote recovery and prevent postnatal illnesses. Family and friends usually discourage any intention to engage in physical exercise (Zhang et al., 2023). As a result, Chinese postpartum women may be susceptible to concerns regarding exercise safety and emotional support from family members. This may have led to a heightened influence of these factors on their intention to use the mobile application in this study. However, existing research suggests that the “postnatal confinement” culture is not unique to China. Many other cultures, including those in Southeast Asia (Withers et al., 2018), Latin America (Chapman and Coups, 1999), and West Africa (Dennis et al., 2007), have similar postnatal resting and isolation practices, albeit under different names. While the specifics of these traditions vary, they share a common concern for the physical vulnerability of postpartum women. It can be inferred that the “Exercise Safety Assurance” factor is also crucial in these cultural contexts. Providing evidence-based guidance and monitoring safe exercise remains central to promoting user adoption across cultures. Similarly, while the sources of emotional support for postpartum women, such as family members, spouses, friends, and professional services, may vary across cultural contexts (McLeish et al., 2021; Qi et al., 2022; Stumbar and Minor, 2023), the emphasis of “Emotional Social Support” on familial and community encouragement reflects a universal human need for social connection. Prior research has consistently shown that robust emotional support enhances psychological well-being and promotes behavioral adherence among postpartum women, regardless of cultural background (Khademi and Kaveh, 2024). The sources of such support can be adapted and expanded to fit different sociocultural settings. Consequently, the findings of this study are considered to have a degree of cross-cultural applicability.
Overall, postpartum women using exercise rehabilitation mobile applications were primarily concerned with the practical attributes of the mobile application, particularly the safety and efficacy of the exercises and the emotional and social support it provided. The findings emphasize that aligning the mobile application’s practical benefits and users’ personal health goals is a key driver of usage behavior. This alignment significantly boosted users’ self-efficacy and enhanced their overall perception of the mobile application’s usefulness, strengthening their intention to use it. In contrast, dialogue support did not significantly influence the intention to use, indicating that postpartum users preferred low-interaction information access rather than two-way communication that demands additional time and effort. Simplicity, directness, and efficiency should remain the main design principles for postpartum women. Furthermore, although the results of this study are generalizable, differences in behavioral norms and sources of social support across cultures should be acknowledged. Future research could employ the same scales and methods to compare multiple cultural contexts, thereby validating these factors’ cross-cultural stability and relative influence. This approach would enhance the artistic sensitivity and generalizability of the model.
Design and management recommendations
4.2
Recommendations based on exercise safety assurance
4.2.1
An examination of the specific items included in the exercise safety assurance indicates that postpartum women prefer the involvement of a professional in customizing and monitoring their exercise program. Consequently, postpartum exercise rehabilitation mobile applications should integrate experts or experienced practitioners in fields such as exercise science and postpartum rehabilitation. These professionals should form a multidisciplinary coaching and health assessment team to provide high-quality, evidence-based exercise guidance for postpartum women.
First, the expert team should personalize the exercise program for postpartum women based on their body characteristics and postnatal injury status. To facilitate postpartum exercise rehabilitation, mobile applications should allow first-time users to input relevant personal information, including delivery details, desired recovery outcomes, and postnatal injury status. Second, to prevent sports injuries resulting from improper movements, the mobile application should provide instructional videos, demonstrated and explained by professionals, when users encounter new exercises or training routines. The mobile application should also incorporate cameras and sensors to monitor users’ exercise postures in real time and offer corrective feedback, thereby enhancing user trust and improving the overall experience. Finally, postpartum exercise rehabilitation mobile applications should incorporate regular assessments of users’ exercise performance and recovery status, enabling timely adjustments to the intensity, frequency, and type of exercise. Thereby enhancing rehabilitation outcomes and reducing exercise-related risks.
Recommendations based on physical activity tracking
4.2.2
An in-depth analysis of the components within physical activity tracking reveals that accurate data collection and feedback, timely knowledge updates, and data security are key factors in enhancing postpartum women’s intention to use the program. First, the mobile application should track key indicators such as exercise duration, calorie expenditure, workout intensity, and weight changes, presenting these results to users through intuitive visualization charts at different stages. This will enable users to perceive the effectiveness of the mobile application in improving postnatal symptoms and enhancing physical fitness, thereby boosting their self-efficacy and increasing their motivation to continue using the mobile application.
Second, the mobile application should promptly integrate and deliver the latest rehabilitation advice and exercise tips, ensuring all content aligns with authoritative medical standards and current research findings. This will enhance the mobile application’s credibility and encourage users to rely on it for long-term support. Additionally, given the significant amount of personal and exercise-related data stored on the platform, it is essential to implement robust data encryption and identity verification mechanisms to protect users’ privacy and safeguard data security.
Recommendations based on emotional social support
4.2.3
In this study, emotional social support primarily refers to mutual encouragement among postpartum women and their recognition and support from friends and family. Analysis of this dimension suggests that establishing an online communication platform and facilitating group exercise activities are effective strategies for enhancing interaction among postpartum users. Therefore, postpartum exercise rehabilitation mobile applications should include an online community feature that fosters a safe, inclusive, and supportive environment. This can help prevent psychological harm caused by weight-related stigma or stereotypical judgments of postpartum body image. Within this community, users can share experiences related to postpartum life and rehabilitation and initiate or join group activities. Such peer interaction has the potential to boost self-confidence and further motivate sustained participation in physical activity.
Moreover, the mobile application should address the lack of understanding and discouragement from friends and relatives regarding postpartum exercise, which may arise due to local cultural practices. To this end, the mobile application could provide educational videos and readings about postpartum exercise rehabilitation, help family members and friends correct misconceptions, and offer them tools to provide positive and sustained support for postpartum women’s exercise behaviors.
Recommendations based on health benefits
4.2.4
In this study, health benefits emphasize the positive impact of postpartum exercise rehabilitation mobile applications on reducing postpartum weight, improving physical fitness, and encouraging the adoption of a healthy lifestyle. To achieve these objectives, mobile applications must offer well-structured, medically-supported exercise programs that encompass a variety of exercise forms and progressively tailored training goals. By guidelines provided by the World Health Organization (WHO) and the American College of Obstetricians and Gynecologists (ACOG), postpartum women are advised to avoid sedentary behavior and, when physically able, engage in at least 150 min of moderate-intensity aerobic exercise per week (Brites-Lagos et al., 2023). This should be complemented by moderate muscle-strengthening and stretching exercises. As recovery progresses, exercise frequency, intensity, and duration should gradually increase.
The mobile application should also offer guidance on healthy routines and meal management to help users develop a sustainable and healthy lifestyle throughout their recovery.
For detailed design and managerial recommendations, see Table 13.
Conclusion
5
Research conclusion
5.1
With the growing attention to the needs of postpartum women and the rapid advancement of mobile health technology, this study addresses the gap in research on the user experience of postpartum rehabilitation mobile applications. It explores the key factors influencing postpartum women’s use of exercise rehabilitation mobile applications from a user experience perspective, employing both qualitative and quantitative research methods. The study developed an evaluation scale and a behavioral model to assess users’ intention to use the postpartum exercise rehabilitation mobile application, offering corresponding design and managerial recommendations. The primary factors influencing postpartum women’s use of these mobile applications were exercise safety assurance, physical activity tracking, emotional and social support, and health benefits. Dialogue support was found to have no direct effect on users’ intention to use the mobile application.
This suggests that postpartum women prioritize the practical attributes of such mobile applications, highlighting the significance of self-efficacy and outcome expectations in behavioral psychology. Additionally, this finding underscores the importance of aligning functional benefits with user goals in designing postpartum mobile applications. This study contributes to the theoretical foundation of mobile health products in postpartum rehabilitation and is a reference for cross-disciplinary research integrating psychology, public health, and interaction design.
Limitations and prospects
5.2
Although this study is pioneering in developing an evaluation scale and behavioral model to assess the intention to use a postpartum exercise rehabilitation mobile application and identify the direct factors influencing users’ intention to use it, several limitations remain.
First, since the research for this study was primarily conducted in China, the findings may be influenced by traditional Chinese cultural norms surrounding the puerperium. While the results and recommendations share some cultural commonalities, differences in postpartum behavior across cultures should be considered. Therefore, future studies could compare the same scales and methods across urban and rural contexts, varying income levels, and diverse cultures to assess the factors’ cross-cultural stability and relative impact, thus enhancing the cultural sensitivity and generalizability of the model.
Secondly, in developing the user experience evaluation scale, this study predominantly relied on self-reported data, such as user interviews, which may introduce subjectivity into the findings. Although efforts were made to supplement this with a comprehensive literature review, potential biases still exist. Future studies could incorporate more objective data on user behavior, such as mobile application usage logs or professional monitoring tools like eye-tracking devices. This would help corroborate the self-reported data and improve the validity and reliability of the evaluation scale.
Finally, while the model developed in this study highlighted the direct positive effects of exercise safety assurance, physical activity tracking, emotional social support, and health benefits on postpartum women’s intention to use the mobile application, the study’s cross-sectional nature limits the model’s comprehensiveness. Several relevant factors, such as affordability, time constraints, lack of time, and fatigue, previously identified in the literature as influencing postpartum physical activity, were not included. Therefore, future research could enhance the model of intention to use postpartum exercise rehabilitation mobile applications by expanding the sample size, broadening the measurement dimensions, and adopting a longitudinal design. Such efforts would contribute to a more robust theoretical framework and offer stronger practical guidance for designing and implementing mobile health interventions in postpartum rehabilitation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Artymuk N. V.Khapacheva S. Y. (2022). Device-assisted pelvic floor muscle postpartum exercise programme for the management of pelvic floor dysfunction after delivery. J. Matern. Fetal Neonatal Med. 35, 481–485. doi: 10.1080/14767058.2020.1723541, PMID: 32019378 · doi ↗ · pubmed ↗
- 2Bandura A. (2004). Health promotion by social cognitive means. Health Educ. Behav. 31, 143–164. doi: 10.1177/1090198104263660, PMID: 15090118 · doi ↗ · pubmed ↗
- 3Bane S. M. (2015). Postpartum exercise and lactation. Clin. Obstet. Gynecol. 58, 885–892. doi: 10.1097/GRF.0000000000000143, PMID: 26398298 · doi ↗ · pubmed ↗
- 4Barrera M.Jr. (1986). Distinctions between social support concepts, measures, and models. Am. J. Community Psychol. 14, 413–445. doi: 10.1007/BF 00922627 · doi ↗
- 5Bennetter K. E.Richardsen K. R.Vøllestad N. K.Jenum A. K.Robinson H. S.Mdala I.. (2023). Associations between social support and physical activity in postpartum: a Norwegian multi-ethnic cohort study. BMC Public Health 23:702. doi: 10.1186/s 12889-023-15507-z, PMID: 37069637 PMC 10111809 · doi ↗ · pubmed ↗
- 6Bhattacherjee A. (2001). Understanding information systems continuance: an expectation-confirmation model. MIS Q. 25, 351–370. doi: 10.2307/3250921 · doi ↗
- 7Birsner M. L.Gyamfi-Bannerman C. (2020). Physical activity and exercise during pregnancy and the postpartum period ACOG committee opinion summary, number 804. Obstet. Gynecol. 135, E 178–E 188. doi: 10.1097/AOG.000000000000377232217980 · doi ↗ · pubmed ↗
- 8Brewer L. C.Fortuna K. L.Jones C.Walker R.Hayes S. N.Patten C. A.. (2020). Back to the future: achieving health equity through health informatics and digital health. JMIR Mhealth Uhealth 8:e 14512. doi: 10.2196/14512, PMID: 31934874 PMC 6996775 · doi ↗ · pubmed ↗