Efficacy and Safety of Oral Betamethasone Mini-Pulses in Moderate to Severe Alopecia Areata
Rasha Moumna, Zineb Loubaris, Anas Ahmed Mountassir, Majdouline Obtel, Benzekri Laila, Mariame Meziane

TL;DR
This study shows that oral betamethasone mini-pulses are effective and safe for treating moderate to severe alopecia areata, with significant hair regrowth and minimal side effects.
Contribution
The study introduces oral betamethasone mini-pulses as a novel treatment option for moderate to severe alopecia areata in resource-limited settings.
Findings
62.5% of patients achieved ≥50% hair regrowth, with 25% experiencing complete regrowth.
Adverse events were mild and transitory, occurring in 20% of cases.
Patchy AA and lower baseline SALT scores were significantly associated with better treatment response.
Abstract
Introduction Alopecia areata (AA) is an acquired autoimmune disorder affecting hair follicles, responsible for non-scarring alopecia with an unpredictable clinical course. Systemic corticosteroids are commonly prescribed in acute or rapidly progressing forms, but their long-term use is limited by potential adverse effects. Intermittent oral corticosteroid regimens, referred to as mini-pulses, have emerged as a promising alternative. Objectives This study aims to assess the efficacy, safety, and sustainability of the response to oral betamethasone mini-pulses in patients with moderate to severe or refractory AA and to explore clinical and trichoscopic predictors of treatment response. Materials and methods We conducted a retrospective cohort study including 40 patients treated for AA at Ibn Sina University Hospital, Morocco, from 2022 to 2025. All patients received oral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
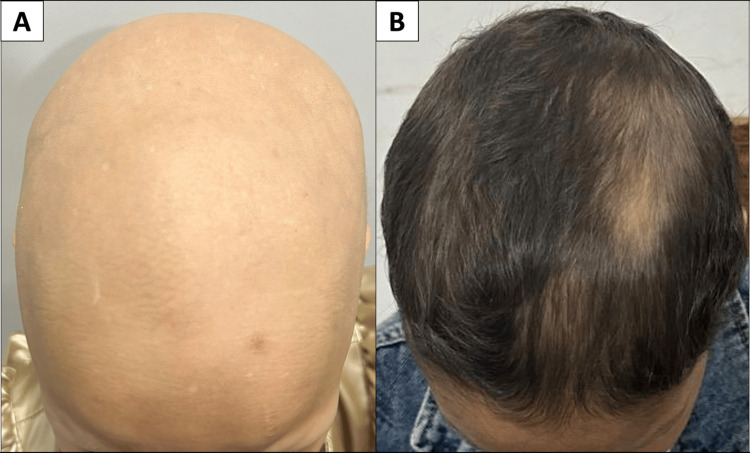 Figure 1
Figure 1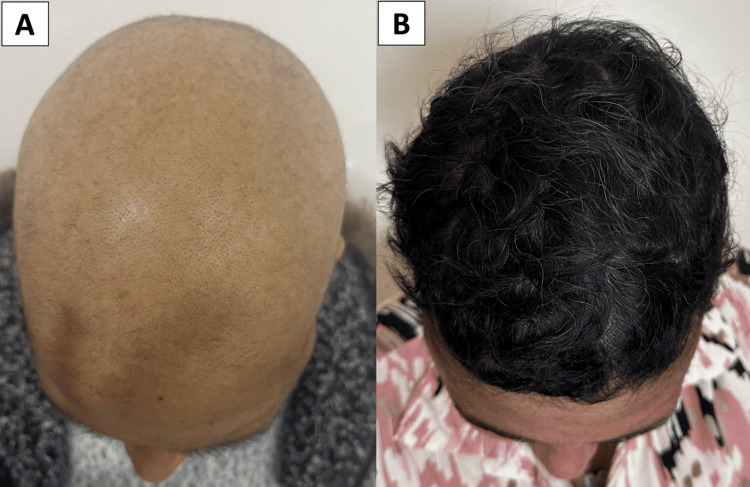 Figure 2
Figure 2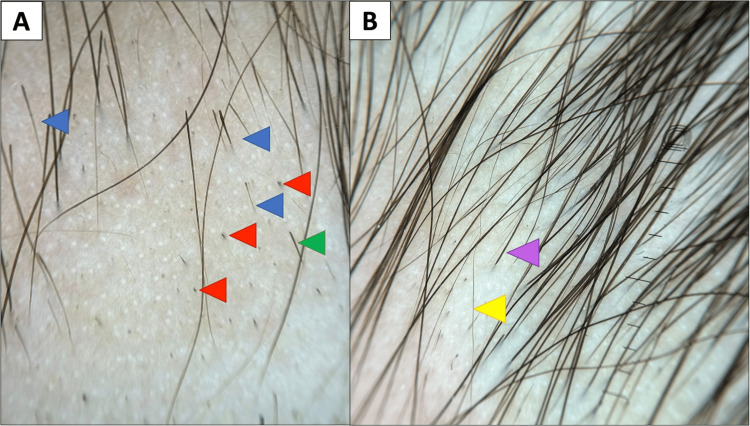 Figure 3
Figure 3| Outcome measure | Baseline | Post-treatment | p-value |
| SALT score (mean) | 54.1 | 24.9 | <0.001 |
| Eyebrow involvement (EBA 0-2, %) | 37.5% | 22.5% | 0.001 |
| Eyelash involvement (ELA 0-2, %) | 27.5% | 15% | 0.019 |
| Body hair involvement (B1-B2, %) | 20% | 7.5% | 0.026 |
| DLQI score (mean) | 5.2 | 1.8 | <0.001 |
| Trichoscopic feature | Baseline (%) | Post-treatment (%) |
| Activity signs | ||
| Black dots | 77.5 | 27.5 |
| Exclamation mark hairs | 72.5 | 20.0 |
| Broken hairs | 62.5 | 17.5 |
| Bent hairs | 20.0 | 7.5 |
| Pohl-Pinkus constrictions | 17.5 | 5.0 |
| Severity signs | ||
| White dots | 32.5 | 20.0 |
| Yellow dots | 17.5 | 7.5 |
| Absent follicular openings | 7.5 | 7.5 |
| Honeycomb pigmentation | 5.0 | 5.0 |
| Regrowth signs | ||
| Vellus hairs | 15.0 | 50.0 |
| Upright regrowing hairs | 5.0 | 55.0 |
| Pigtail hairs | 5.0 | 17.5 |
| Baseline characteristics | Association | p-value | Statistical test |
| Patchy AA | Favorable response | 0.046 | Fisher’s exact test |
| Lower baseline SALT score | Favorable response | 0.027 | Mann–Whitney U test |
| Higher baseline SALT score | Poor response | 0.023 | Mann–Whitney U test |
| Rapidly progressive AA (RP-AA) | Poor response | 0.007 | Fisher’s exact test |
| Atopic background | Poor response | 0.046 | Fisher’s exact test |
| Autoimmune thyroiditis | Relapse | 0.045 | Fisher’s exact test |
| Vitamin D deficiency | Relapse | 0.024 | Fisher’s exact test |
| Study | n | Age range (years) | Regimen | ≥50% regrowth (%) | Relapse (%) | Adverse events (%) |
| Khaitan et al., 2004 | 16 | 14-36 | 5 mg/day, 2 days/week | 75 | 6.2 | 25 |
| Deshpande et al., 2011 | 15 | 7-45 | 0.1 mg/kg/day, 2 days/week + short contact anthralin + topical minoxidil | 73.3 | 13.3 | 13.3 |
| Gupta et al., 2019 | 21 | 24-27 | 5 mg/day, 2 days/week | 71.4 | 24 | 76 |
| Asilian et al., 2021 | 12 | 16-60 | 3 mg, 1 day/week | Median SALT reduced from 100% to 74% | Not reported | 0 |
| Present study | 40 | 6-50 | 2-4 mg/day, 2 days/week | 62.5 | 15 | 20 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHair Growth and Disorders · Dermatologic Treatments and Research
Introduction
Alopecia areata (AA) is a common autoimmune disease targeting the hair follicle, with multifactorial pathogenesis involving genetic, immunologic, and environmental contributors [1]. It usually presents as well-demarcated patches of non-scarring alopecia on the scalp. However, it can progress to more severe forms such as alopecia totalis (AT) or alopecia universalis (AU) and may also affect the eyebrows, eyelashes, body hair, and nails, contributing to its physical and psychosocial burden [1].
Systemic corticosteroids are a standard therapeutic option in acute or extensive forms of AA. However, their long-term use is limited by the relatively high risk of relapses and potential adverse effects [2]. To reduce these risks, intermittent oral corticosteroid regimens - commonly referred to as “mini-pulses” - have been proposed. These protocols typically involve administering corticosteroids two days per week to maintain efficacy while lowering cumulative toxicity [2]. However, oral corticosteroid mini-pulses for AA remain insufficiently studied and underdocumented in the literature [3]. Yet they represent a promising and affordable therapeutic approach, especially in resource-limited settings where access to advanced therapies such as Janus kinase (JAK) inhibitors is restricted.
This study aims to assess the efficacy and safety of oral betamethasone mini-pulse therapy in moderate to severe or refractory AA. Secondary objectives include evaluating the durability of regrowth after treatment cessation, identifying clinical and trichoscopic predictors of response, and comparing findings with existing literature.
Materials and methods
Study design and setting
This was a retrospective cohort study with both descriptive and analytical approaches, conducted at the Dermatology Department of Ibn Sina University Hospital in Rabat, Morocco, over a three-year period (February 2022 to February 2025).
Inclusion and exclusion criteria
Patients were included if they were at least five years old, had a diagnosis of AA confirmed by clinical and dermoscopic findings, and had received oral betamethasone mini-pulses for at least three months.
Patients were excluded if they had ongoing or recent (<1 month) systemic treatment for AA other than betamethasone mini-pulses, incomplete clinical documentation or photographic records, or were lost to follow-up.
Treatment protocol
In this cohort, all patients had received oral betamethasone mini-pulses at fixed doses of 2 mg/day for children and 4 mg/day for adults, administered two consecutive days per week. Treatment tapering was performed at variable times, depending on when cosmetically acceptable regrowth was achieved. Daily zinc supplementation and topical 2% minoxidil had also been routinely prescribed, and iron and vitamin D supplementation were added when deficiencies were documented.
Outcome measures
Treatment efficacy was assessed using the Severity of Alopecia Tool (SALT) [4], the Alopecia Areata Scale (AAS) [5], the Eyebrow (EBA) and Eyelash (ELA) Assessment Scales [6], the Dermatology Life Quality Index (DLQI) [7], and a visual analog scale for patient satisfaction (ranging from 0: not satisfied at all to 10: highly satisfied). Trichoscopy was also used in all patients to monitor disease activity and assess response to treatment.
Data collection
Data were extracted from patient medical records and standardized clinical photographs. In cases of missing clinical information, data were collected through follow-up with the patient or their family.
Statistical analysis
Descriptive statistics were used to summarize patient characteristics. Quantitative variables were expressed as means ± standard deviation or medians with interquartile ranges, depending on the distribution. Categorical variables were expressed as counts and percentages.
Analytical comparisons of pre- and post-treatment outcomes were performed using the Wilcoxon signed-rank test. Baseline factors associated with treatment response and relapse were analyzed using the Mann-Whitney U test for continuous variables and Fisher’s exact test for categorical variables. A p-value less than 0.05 was considered statistically significant.
Ethical considerations
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki [8]. As it was a retrospective study of anonymized patient records, formal ethical approval was not required according to our institutional policy. Informed consent was obtained from all patients or their legal guardians for the use and publication of their clinical data and photographs.
Results
Patient demographics and comorbidities
A total of 40 patients (n = 40) were included, with a female predominance (65%). The mean age was 16.5 years (range: 6-50), with children and adolescents representing 70% of the cohort and adults representing 30%. Comorbid conditions included atopic diseases (25%), autoimmune thyroiditis (17.5%), and psychiatric manifestations such as anxiety or depression (10%). A family history of AA was reported in 12.5% of cases.
Disease baseline characteristics
An identifiable trigger was reported by 50% of patients. Psychological stress was the most frequent (35%), followed by COVID-19 vaccination, infection, or post-partum status (each 5%). In 30% of cases, consultation was delayed for more than one year after disease onset.
At baseline, the mean SALT score was 54.1%. According to the AAS, 50% of patients had severe forms (SALT ≥ 50), including 42.5% with AT/AU; 40% had moderate AA (SALT 21-49), and 10% had mild but refractory forms (SALT ≤ 20). Rapidly progressive AA (RP-AA), defined as diffuse hair loss with ≥50% scalp involvement within less than three months [9], was observed in 22.5% of cases. Eyebrow involvement (EBA 0-2) was observed in 37.5% of patients, eyelash loss (ELA 0-2) in 27.5%, and body hair involvement (B1-B2) in 20%. The mean baseline DLQI score was 5.2, with 40% reporting a moderate to severe impact on quality of life.
Treatment efficacy
Treatment resulted in significant clinical improvement. The average time to visible regrowth was 2.7 months. A ≥50% reduction in SALT (SALT-50) was achieved in 62.5% of patients (Figure 1), and complete regrowth was observed in 25% (Figure 2).
Marked clinical improvement in an eight-year-old patient with alopecia universalis following oral betamethasone mini-pulse therapy(A): Baseline presentation showing complete scalp hair loss(B): Significant regrowth (≥50%) observed after six months of treatment, with restored scalp coverage and hair density
Complete hair regrowth in a 30-year-old patient with alopecia totalis following six months of oral betamethasone mini-pulse therapy(A): Baseline presentation showing total scalp hair loss(B): Marked regrowth of dense, pigmented scalp hair after treatment
The mean SALT score decreased from 54.1% to 24.9% (p < 0.001). Eyebrow, eyelash, and body hair involvement also decreased significantly. DLQI scores improved from a mean of 5.2 to 1.8 (p < 0.001), and 77.5% of patients reported being satisfied or highly satisfied with treatment. The main outcome measures are summarized in Table 1.
Trichoscopic evaluation at the end of treatment showed a marked reduction in disease activity markers. Observed trends included a decrease in black dots from 77.5% to 27.5%, exclamation mark hairs from 72.5% to 20%, and broken hairs from 62.5% to 17.5%. In parallel, signs of regrowth increased considerably: vellus hairs from 15% to 50%, upright regrowing hairs from 5% to 55%, and pigtail hairs from 5% to 17.5% (Table 2, Figure 3).
Trichoscopic evolution in a patient treated with oral betamethasone mini-pulses(A): Before treatment, showing predominance of disease activity markers: black dots (red arrows), exclamation mark hairs (blue arrows), and broken hairs (green arrow)(B): After treatment, marked predominance of regrowth indicators: vellus hairs (yellow arrow) and upright terminal hairs (purple arrow)
Tolerability
The treatment was well tolerated. Adverse events occurred in 20% of patients, the most common being mild hypertrichosis (12.5%), which may have been related to topical minoxidil use, as it was consistently localized to the face and neck. Other side effects included cushingoid facies, sleep disturbances, and rosacea flare, each observed in a single patient (2.5%). No serious adverse events were reported.
Follow-up and relapse
The average total treatment duration was 9.9 months. At a mean follow-up of 10 months, 88% (22 of 25) of patients who achieved a favorable response (≥50% regrowth) maintained their results after stopping treatment, with no relapse.
Relapse was observed in 15% of patients. Half of them (7.5%) had shown poor initial response (<25% regrowth), while the remaining half had achieved satisfactory improvement (≥50% regrowth) during treatment.
Predictive factors
Statistical analysis identified several baseline factors associated with treatment outcomes. Patients with patchy AA and lower baseline SALT scores were significantly more likely to respond favorably to mini-pulse therapy. In contrast, poor response was associated with higher baseline SALT scores, rapidly progressive disease, and atopic background. Although relapse was infrequent, it was significantly more common in patients with autoimmune thyroiditis or vitamin D deficiency (Table 3).
Table 3: Baseline characteristics associated with treatment response and relapseAssociations were analyzed using the Mann–Whitney U test for continuous variables and Fisher’s exact test for categorical variables. A favorable response was defined as ≥50% hair regrowth (SALT-50), and a poor response as <25% regrowth. A p-value less than 0.05 was considered statistically significant.AA: alopecia areata; SALT: Severity of Alopecia Tool; RP-AA: rapidly progressive alopecia areata
Discussion
Oral corticosteroids are commonly used in the management of moderate to severe or rapidly progressing AA. According to the 2024 European consensus on the treatment of AA, systemic corticosteroids may be considered as a first-line option in adults with recent (<6 months) and active moderate to severe AA. However, their long-term use - especially in children - is not recommended due to concerns regarding tolerability and safety [5]. Oral corticosteroid mini-pulses are intermittent regimens that offer the advantage of reduced cumulative toxicity, allowing for prolonged treatment courses with improved tolerability [2].
In recent years, JAK inhibitors have emerged as a promising therapeutic class, supported by clinical trial data and increasing regulatory approvals. However, their high cost and limited accessibility remain major barriers in many low-income and developing countries [10]. In this context, oral corticosteroid mini-pulses represent an accessible and promising alternative that remains highly relevant in real-world practice.
Nevertheless, betamethasone mini-pulse therapy remains underdocumented in the literature. To date, no large-scale randomized controlled trials have evaluated its efficacy or long-term outcomes [3]. Table 4 provides a comparative summary of published studies using oral betamethasone mini-pulses for AA [11-14].
Although study outcomes varied slightly, most reported ≥50% regrowth rates between 62.5% and 75%, with relapse rates ranging from 6.2% to 24%. Moreover, no serious adverse events were reported across all four studies; side effects were consistently mild and transient [11-14]. These results align with our findings, further supporting the potential value of this regimen in real-world practice.
Furthermore, Gupta et al. [13] demonstrated that betamethasone mini-pulses were more effective than weekly azathioprine pulses in inducing hair regrowth. In another study, Asilian et al. [14] reported that combining methotrexate with betamethasone mini-pulses led to superior outcomes compared to either agent used alone, highlighting the potential benefit of combination regimens in severe or refractory cases.
Other corticosteroids have also been used in mini-pulse regimens for AA, including prednisolone and dexamethasone. Studies using dexamethasone mini-pulses (typically 2.5-5 mg/day for two days weekly) have reported SALT-50 responses between 50% and 68%, with complete regrowth rates varying from 15% to 30% [15-17]. Prednisolone-based regimens show comparable outcomes but may carry a higher risk of side effects [18-19]. Overall, while efficacy appears similar between molecules, betamethasone offers a favorable balance between potency and safety in low-dose intermittent regimens.
Beyond efficacy comparisons, several studies have highlighted baseline characteristics that may influence the response to mini-pulse corticosteroid therapy. Kar et al. (2005) [18] reported better treatment outcomes in patients with recent disease onset, limited scalp involvement, and no history of atopy. Bajaj et al. (2008) [19] observed greater efficacy in patchy-type AA. Finally, Sánchez-Díaz et al. (2022) [16] and Lobato-Berezo et al. (2022) [17] noted reduced response rates in patients with autoimmune hypothyroidism. These trends are consistent with our findings. Nevertheless, further research is needed to better define the clinical profile of patients most likely to benefit from mini-pulse regimens, particularly when using betamethasone.
To the best of our knowledge, this is the largest cohort study to date assessing betamethasone mini-pulses in AA and the first to do so in a Moroccan cohort. Strengths of the study include the integration of clinical, dermoscopic, and quality-of-life outcomes. However, its retrospective design, limited sample size, and absence of a control group restrict the strength of interpretation. Larger controlled studies are needed to confirm these results, refine patient selection, and optimize treatment protocols.
Conclusions
Our findings suggest that oral betamethasone mini-pulses may represent a safe and effective therapeutic option for moderate to severe or refractory AA. Good to excellent regrowth was achieved in the majority of patients, with favorable tolerance and sustained results in most responders. The use of trichoscopy provided additional non-invasive insights into disease activity and regrowth, reinforcing its value as a complementary monitoring tool.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alopecia areata: understanding the pathophysiology and advancements in treatment modalities Cureus Abarca YA Scott-Emuakpor R Tirth J 017202510.7759/cureus.78298 PMC 1187217340026917 · doi ↗ · pubmed ↗
- 2Update on pulse corticosteroid therapy for themanagement of alopecia areata EADV Clin Pract Bernhardt J Wenzel J 96297132024
- 3The efficacy and adverse effects of corticosteroid pulse therapy in alopecia areata: a review article Dermatol Pract Concept Rastaghi F Kaveh R Yazdanpanah N Sahaf AS Ahramyanpour N 11113202310.5826/dpc.1304 a 255PMC 1065613537992355 · doi ↗ · pubmed ↗
- 4Alopecia areata investigational assessment guidelines - Part II. National Alopecia Areata Foundation J Am Acad Dermatol Olsen EA Hordinsky MK Price VH 4404475120041533798810.1016/j.jaad.2003.09.032 · doi ↗ · pubmed ↗
- 5European expert consensus statement on the systemic treatment of alopecia areata J Eur Acad Dermatol Venereol Rudnicka L Arenbergerova M Grimalt R 6876943820243816908810.1111/jdv.19768 · doi ↗ · pubmed ↗
- 6Hair loss profiles and Ritlecitinib efficacy in patients with alopecia areata: post hoc analysis of the ALLEGRO Phase 2b/3 study Dermatol Ther (Heidelb) Thaçi D Tziotzios C Ito T 262126341320233770776410.1007/s 13555-023-00997-x PMC 10613177 · doi ↗ · pubmed ↗
- 7Dermatology Life Quality Index (DLQI) - a simple practical measure for routine clinical use Clin Exp Dermatol Finlay AY Khan GK 210216191994803337810.1111/j.1365-2230.1994.tb 01167.x · doi ↗ · pubmed ↗
- 8World Medical Association Declaration of Helsinki: ethical principles for Medical Research involving human subjects JAMA World Medical Association 2191219431020132414171410.1001/jama.2013.281053 · doi ↗ · pubmed ↗